
Comparing letrozole versus clomiphene citrate for ovulation induction in polycystic ovary syndrome: a retrospective study
Ovulation induction in PCOS
Authors
Abstract
AimThis study compares the effects of clomiphene citrate (CC) and letrozole on pregnancy outcomes in infertile patients with polycystic ovary syndrome (PCOS) and examines the influence of mild hyperprolactinemia on these outcomes. There is limited research examining the effect of mildly elevated prolactin (PRL) levels during ovulation induction cycles in PCOS patients.
MethodsA retrospective analysis was conducted on 226 primary infertile PCOS patients with an infertility duration of 1-3 years. Patients were treated with either CC or letrozole as oral ovulation induction agents. Statistical analysis was performed using R software, applying Welch’s t-test, Student’s t-test, Mann-Whitney U test, Pearson chi-square test, and Fisher-Freeman-Halton test. A p-value of <0.05 was considered statistically significant.
ResultsThe letrozole group exhibited more mono follicular development compared to the CC group (92.52% vs. 83.54%; RR=1.11,[95% CI, 0.99 to 1.23] p=0.037). The mean endometrial thickness was significantly greater in the letrozole group (9.86 ± 2.70 mm) compared to the CC group (8.77 ± 2.68 mm). No significant differences were found in clinical pregnancy rates (29.93% vs. 29.11%; RR=1.03,[95% CI, 0.67 to 1.57] p=0.898) and live birth rates (25.85% vs. 22.78%; RR=1.13,[95% CI, 0.70 to 1.85] p=0.611) between the two groups. PRL levels did not significantly differ between the clinically pregnant and nonpregnant groups.
ConclusionWe found no difference in pregnancy or live birth rates between CC and letrozole. Letrozole increased endometrial thickness and mono-follicular development. Minimal PRL elevation did not affect pregnancy outcomes, suggesting treatment may be unnecessary.
Keywords
Introduction
Infertility is described as the inability to conceive after one year of trying for women under 35 years of age and after six months for women above 35 who do not use any contraception method.1 Infertility may result from male, female, or combined reasons. Anovulation is the cause of infertility in 25% of couples.2 The most common cause of anovulation is PCOS. PCOS is a complex disease encompassing metabolic and reproductive disorders. According to the 2023 International Evidence-based Guideline Criteria, to confirm the diagnosis of PCOS, at least two out of the following three criteria must be met: clinical or biochemical hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology.3 Management strategies for subfertility linked to PCOS typically focus on lifestyle modifications, drug treatments, surgical interventions, and the use of assisted reproductive technologies. Letrozole should be used as the first-line ovulation induction agent, followed by CC as the second option. Letrozole, a widely used selective non-steroidal third-generation aromatase inhibitor, is primarily utilized for ovulation induction. It acts by inhibiting the secretion of estradiol in the ovaries. Letrozole continues to be used off-label for ovulation induction despite not having approval from the US Food and Drug Administration (FDA) for this specific use.4 CC has been used for many years as a selective estrogen receptor modulator, it antagonizes the negative effects of estrogen in the hypothalamus and stimulates follicular development as an endogenous gonadotropin.5 Contrary to the multi-follicular development in CC, mono-follicular development in LE has been shown to reduce the risk of multiple pregnancies.6 In many studies conducted on PCOS patients, LE is superior to CC regarding ovulation, pregnancy, and live birth.7,8
Elevated or reduced PRL levels can lead to infertility by causing anovulation or infrequent ovulation (oligo-ovulation) through mechanisms related to hormonal imbalances, with abnormal PRL activity occurring both in the blood and within ovarian tissues.9,10 Hyperprolactinemia was classified into three levels by the Canadian Medical Association: mild (serum PRL levels under 50 ng/mL), moderate (serum PRL levels ranging from 50 to 100 ng/mL), and severe (serum PRL levels exceeding 100 ng/mL).11 In 30% of patients with PCOS, elevated levels of serum PRL are observed during both the follicular and luteal phases of the menstrual cycle.12,13 A meta-analysis investigating PRL concentrations in women with PCOS versus those without shows generally elevated PRL concentrations in women diagnosed with PCOS, proposing that these could serve as a potential diagnostic indicator for PCOS.14
In this study, we compared the ovulation induction parameters, clinical pregnancy, abortion, and live birth rates in groups using oral ovulation induction agents CC or letrozole in infertile PCOS patients. We also investigated whether mild PRL elevation in PCOS patients affected pregnancy outcomes.
Materials and Methods
Patient records were accessed from the computer system and infertility forms in the file archives of the Konya City Hospital IVF unit between the years 2018 and 2022. Age, body mass index (BMI), basal hormone profiles on day 2 of menstruation, dominant follicle size, endometrial thickness on the day of dominant follicle measurement, sperm parameters, clinical pregnancy, live birth, abortion, birth week parameters were compared between the groups using letrozole and CC for ovulation induction.
Inclusion-exclusion criteria
For this study, we included the first treatment cycle of primary infertile patients who had a history of infertility of at least one year but not exceeding three years and who were diagnosed with PCOS according to the Rotterdam criteria and used CC or letrozole as an oral ovulation induction agent. Information about the patients was obtained retrospectively from files and computer records. All patients had confirmed tubal patency via hysterosalpingography (HSG), and normal spermiogram values were observed. PRL levels measured on the 2nd or 3rd day of the menstrual cycle, ranging between 20-50 ng/mL, were considered as mild hyperprolactinemia. In our laboratory, the upper limit of normal PRL levels is deemed to be 20 ng/mL. Hyperprolactinemia treatment was not administered to these patients.
Patients whose BMI exceeds 30 kg/m², those with endometrioma/endometriosis, endometrial pathologies, and mullerian anomaly, detected tubal factors, systemic or immunological diseases, and patients with serum PRL levels of 50 ng/mL were excluded from the study.
Ovulation Induction ProtocolAll patients were assessed on the 2nd or 3rd day of menstruation for basal hormone profile and were screened for persistent cysts using transvaginal ultrasound before starting CC (Klomen, Koçak Farma, Istanbul, Turkey) or letrozole (Femara, Novartis, Istanbul, Turkey) at a dose of 2x50mg or 2x2.5mg. In our infertility clinic, we primarily prefer letrozole as the oral agent. However, when the government does not cover this medication or patients sometimes choose not to use it for various reasons, we prescribe CC, which is covered by the government and is less expensive. After taking the medication for 5 days, patients were instructed to take a 5-day break and then invited to the hospital for folliculometry. When the endometrial thickness reached >7 mm, and the follicle diameter reached at least 20 mm, patients were recommended to engage in sexual intercourse every other day. They were called back to the hospital 15 days later for a pregnancy test. Patients who showed a heartbeat on transvaginal ultrasound were considered to have a clinical pregnancy positive, and those who delivered a live birth weighing 500 grams or more or after 24 weeks were considered to have a live birth.
Ethical ApprovalThis study was approved by the Ethics Committee of Karatay University Faculty of Medicine (Date: 15.02.2024, Decision No: 2024/027).
Statistical AnalysisThe study was designed to achieve a power of 80% to detect an absolute difference in pregnancy rate between treatment groups using Pearson’s chi-square test at a two-sided significance level of 0.05 and a medium effect size of 0.5. We estimated that the analysis would need a sample size of 75 patients per treatment group, which was increased to 100 to account for a potential 10% dropout rate.
Baseline characteristics were reported as counts (n) and proportions (%), or mean ± standard deviation and median with ranges (minimum-maximum) or inter-quartiles [1st quartile–3rd quartile]. A Welch’s t-test, student’s t-test, Mann-Whitney U test, Pearson chi-square test, and Fisher-Freeman-Halton test were used to compare the baseline characteristics of the participants between drug groups. A two-sided p-value of less than 0.05 was considered to indicate statistical significance. All statistical analyses were performed with R software, version 4.2.1. (The R Foundation for Statistical Computing, Vienna, Austria).
Reporting GuidelinesThe study was reported in accordance with the STROBE guideline.
Results
Patients who used the LE drug were older than those who used the CC (29.44 ± 5.84 years vs. 26.10 ± 4.86 years, p<0.001). The BMI, FSH (follicle-stimulating hormone), and basal estradiol levels of the two trial groups were similar. Compared with patients who received CC, patients who received letrozole demonstrated higher LH (luteinizing hormone) levels (10.97 ± 2.96 IU/mL vs. 9.33 ± 3.21 IU/mL, p<0.001) and less PRL levels (28 ng/dl [IQR, 25–33] vs. 31 ng/dl,[IQR, 25–36] p=0.005). The mean endometrial thickness was measured at 9.86 ± 2.70 mm for the letrozole group and 8.77 ± 2.68 mm in those receiving CC, and this high measure was statistically significant. The sperm volume was significantly lower in the letrozole group (2.5 ml [IQR, 2–3] vs. 3 ml,[IQR, 2.5–3.35] p=0.007). There was no evidence of sperm motility and TPMS (total progressively motile sperm) count between groups. The baseline characteristics of participants are presented in Table 1.
The reproductive outcomes of the study participants are presented in Table 2. The clinical pregnancy (29.93% vs. 29.11%, RR=1.03,[95% CI, 0.67 to 1.57] p=0.898) and live birth (25.85% vs. 22.78%, RR=1.13,[95% CI, 0.70 to 1.85] p=0.611) rates in the letrozole group were slightly higher than that in the CC group, but the differences were not statistically significant. The patients who received letrozole had more mono follicular development than the patients who received CC (92.52% vs. 83.54%, RR=1.11,[95% CI, 0.99 to 1.23] p=0.037). 16.46% (13 out of 79 patients) of patients who received CC and 6.80% (10 out of 147) of those who received letrozole developed multifollicular growth, therefore letrozole was associated with a 59% (RR=0.41,[95% CI, 0.19 to 0.90] p=0.022) reduction in the risk of multi follicular development.
Table 3 compares the characteristics of the groups with and without clinical pregnancy. There was no difference in PRL levels between the groups who did and did not become pregnant (p=0.592).
Discussion
We did not observe any difference in clinical pregnancy and live birth rates between the groups using CC and letrozole in PCOS patients. We concluded that minimal PRL elevation has no adverse effects on clinical pregnancy and live births. Literature includes studies on the impact of elevated PRL levels on IVF outcomes, but there is limited research examining the effect of mildly elevated PRL during ovulation induction cycles in PCOS patients on pregnancy outcomes.
The treatment of infertility due to anovulation in women with PCOS requires a multifaceted approach. According to Balen et al.15 lifestyle interventions are recommended as the initial treatment, especially for obese patients, to enhance the effectiveness of subsequent therapies. Pharmacologically, CC is commonly used, but letrozole may offer better ovulation and pregnancy rates. For resistant cases, options like bariatric surgery or IVF are considered, though they carry inherent risks. According to a comprehensive individual participant data (IPD) meta-analysis, letrozole significantly improves live birth and clinical pregnancy rates in women with PCOS compared to CC. Notably, the efficacy of letrozole is further enhanced in women with higher baseline serum total testosterone levels. This finding suggests that letrozole may be particularly beneficial for a subgroup of PCOS patients characterized by higher androgen levels, supporting a more personalized approach to treatment.16
The management of infertility in women with PCOS continues to evolve, particularly in the context of selecting optimal ovulation induction agents. The studies by Bahawi et al. and Wang et al.17,18 along with our data, provide insights into the effectiveness of letrozole and CC in inducing ovulation and achieving pregnancy in PCOS patients. Both Bahawi et al. and our study reported slightly higher pregnancy rates with LE compared to CC, but this was not statistically significant. Wang et al.18 also noted superior endometrial receptivity in the letrozole group, which could theoretically lead to higher pregnancy rates, though this was not directly compared in our study.
Patients in the Bahawi et al.17 study required fewer treatment cycles when using letrozole compared to CC, a finding somewhat echoed in our data, where letrozole also demonstrated a higher rate of mono follicular development. This could indicate a more targeted and efficient follicular response with letrozole, reducing the risk of multi-follicular development and its associated complications, such as ovarian hyperstimulation syndrome. The collective findings underscore the potential benefits of letrozole in treating infertility associated with PCOS, particularly in terms of endometrial receptivity and the efficiency of achieving pregnancy. However, the absence of significant differences in live birth rates and the similar overall pregnancy rates observed in our study suggests that both medications remain viable first-line options, with the choice potentially guided by patient-specific factors such as tolerance to medication and specific endocrine profiles.
PRL, traditionally associated with lactation and reproductive functions, also plays a significant role in metabolic regulation, which is particularly relevant in the context of PCOS. Research indicates that PRL levels may influence various metabolic processes in PCOS, affecting glucose and lipid metabolism and overall metabolic homeostasis.19 PCOS is often accompanied by hormonal imbalances that include not only the well-known issues of hyperandrogenism and insulin resistance but also varied PRL levels. Elevated PRL levels, or hyperprolactinemia, can exacerbate the symptoms of PCOS, including menstrual irregularities and infertility, by impacting ovarian function directly and by altering metabolic functions.19 Interestingly, while extremely high or deficient PRL levels are linked to adverse metabolic effects, a specific range of elevated PRL levels might be beneficial, potentially enhancing metabolic stability in PCOS patients. This suggests a nuanced role of PRL, where its concentration-dependent effects could either contribute to or mitigate metabolic dysfunctions associated with PCOS.20
While there are studies in the literature on the impact of elevated PRL levels on IVF outcomes, there is no research on the effect of mild PRL elevation during ovulation induction cycles in patients with PCOS on pregnancy outcomes. A study examines serum PRL level changes during Intracytoplasmic Sperm Injection (ICSI) in 90 patients and their impact on pregnancy rates. Results indicate a significant increase in PRL levels post-ovum pickup, which normalized before embryo transfer and did not affect pregnancy outcomes. A positive correlation was found between early PRL levels and higher-quality embryos, suggesting that early PRL measurements may help predict embryo quality.21
Another study complementing this research examined the correlation between serum PRL levels and cumulative pregnancy outcomes in in-vitro fertilization and intracytoplasmic sperm injection (IVF/ICSI) cycles. The study suggests that higher baseline PRL levels, particularly those below 50 ng/mL, might positively influence the number of oocytes retrieved and embryos and increase the rates of clinical pregnancies and live births. The study explores the potential positive implications of maintaining mildly elevated PRL levels during IVF/ICSI treatments, challenging previous assumptions about the need to suppress high PRL levels.22 In contrast to these studies, a series of 20,877 patients examined the relationship between PRL levels and live birth in patients without PCOS, indicating that there is a significant relationship between serum PRL levels and live birth rates. Specifically, PRL levels below 14.8 ng/mL positively correlate with higher live birth rates. However, once PRL levels exceed this threshold, the relationship becomes insignificant, suggesting an optimal range for PRL that may influence pregnancy outcomes positively.23
In our study, when we compared PRL levels between the group with clinical pregnancies and the group without, although the PRL levels were slightly higher in the group with clinical pregnancies (27.70 ± 9.05 ng/mL vs. 28.40 ± 8.92 ng/mL), this difference was not statistically significant (p=0.592).
Limitations
Limitations of the study are: first, it was a retrospective study with a small sample size. Secondly, we recommended coitus every other day, but we did not check for ovulation or whether the patient’s coitus regularly and at the recommended time. Age values were significantly higher in the letrozole group compared to the CC group, which may be one of the reasons for the lack of statistically significant high pregnancy rates in the letrozole group. On the other hand, the reason why PRL levels did not affect pregnancy outcomes may be that the patients in the study did not have very high PRL levels. Therefore, it may not be correct to conclude that high prolactin levels do not affect pregnancy outcomes based on our results.
Conclusion
In conclusion, we observed no difference in clinical pregnancy and live birth rates between groups using CC and letrozole. Consistent with the literature, we found that the group using letrozole had greater endometrial thickness and higher rates of mono follicular development compared to the CC group. Additionally, we discovered that minimal PRL elevation was not statistically significant between the groups who did and did not become pregnant. This research contributes to our understanding of how PRL might affect fertility outcomes. It may assist clinicians in deciding whether or not to treat minimal PRL elevation.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all patients.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
BMI: Body mass index
CC: Clomiphene citrate
FDA: Food and Drug Administration
FSH: Follicle-stimulating hormone
HSG: Hysterosalpingography
ICSI: Intracytoplasmic sperm injection
IVF: In vitro fertilization
LE: Letrozole
LH: Luteinizing hormone
PCOS: Polycystic ovary syndrome
PRL: Prolactin
RR: Relative risk
TPMS: Total progressively motile sperm
References
-
Practice Committee of the American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertil Steril. 2020;113(3):533-535. doi:10.1016/j.fertnstert.2019.11.025
-
Weiss RV, Clapauch R. Female infertility of endocrine origin. Arq Bras Endocrinol Metabol. 2014;58(2):144-152. doi:10.1590/0004-2730000003021
-
Teede HJ, Tay CT, Laven JJ, et al. Recommendations from the 2023 International Evidence-Based Guideline for the assessment and management of polycystic ovary syndrome. Eur J Endocrinol. 2023;189(2):G43-G64. doi: 10.1093/ejendo/lvad096
-
Tanbo T, Mellembakken J, Bjercke S, Ring E, Åbyholm T, Fedorcsak P. Ovulation induction in polycystic ovary syndrome. Acta Obstet Gynecol Scand. 2018;97(10):1162-1167. doi:10.1111/aogs.13395
-
Cunha A, Póvoa AM. Infertility management in women with polycystic ovary syndrome: a review. Porto Biomed J. 2021;6(1):e116. doi:10.1097/j.pbj.0000000000000116
-
Kamath MS, George K. Letrozole or clomiphene citrate as first line for anovulatory infertility: a debate. Reprod Biol Endocrinol. 2011;9:1-4. doi:10.1186/1477-7827-9-86
-
Misso ML, Wong JL, Teede HJ, et al. Aromatase inhibitors for PCOS: a systematic review and meta-analysis. Hum Reprod Update. 2012;18(3):301-312. doi:10.1093/humupd/dms003
-
Roy KK, Baruah J, Singla S, et al. A prospective randomized trial comparing the efficacy of letrozole and clomiphene citrate in induction of ovulation in polycystic ovarian syndrome. J Hum Reprod Sci. 2012;5(1):20-25. doi:10.4103/0974-1208.97789
-
Auriemma RS, Del Vecchio G, Scairati R, et al. The interplay between prolactin and reproductive system: focus on uterine pathophysiology. Front Endocrinol (Lausanne). 2020;11:594370. doi:10.3389/fendo.2020.594370
-
Štelcl M, Vrublovský P, Machač Š. Prolactin and alteration of fertility. Ceska Gynekol. 2018;83(3):232-235.
-
Serri O, Chik CL, Ur E, Ezzat S. Diagnosis and management of hyperprolactinemia. CMAJ. 2003;169(6):575-581.
-
Davoudi Z, Araghi F, Vahedi M, Mokhtari N, Gheisari M. Prolactin level in polycystic ovary syndrome: an approach to the diagnosis and management. Acta Biomed. 2021;92(5).
-
Kim SI, Yoon JH, Park DC, Yang SH, Kim YI. What is the optimal prolactin cutoff for predicting the presence of a pituitary adenoma in patients with polycystic ovary syndrome? Int J Med Sci. 2023;20(4):463-467. doi:10.7150/ijms.80891
-
Saei Ghare Naz M, Mousavi M, Mahboobifard F, Niknam A, Ramezani Tehrani F. A meta-analysis of observational studies on prolactin levels in women with polycystic ovary syndrome. Diagnostics (Basel). 2022;12(12):2924. doi:10.3390/diagnostics12122924
-
Balen AH, Morley LC, Misso M, et al. The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Hum Reprod Update. 2016;22(6):687-708. doi:10.1093/humupd/dmw025
-
Wang R, Li W, Bordewijk EM, et al. First-line ovulation induction for polycystic ovary syndrome: an individual participant data meta-analysis. Hum Reprod Update. 2019;25(6):717-732. doi:10.1093/humupd/dmz029
-
Bahawi YO, Radwan EM, Khouj MA, et al. Pregnancy rates in women with polycystic ovary syndrome using letrozole versus clomiphene citrate: a retrospective record review. Cureus. 2023;15(7): e42257. doi:10.7759/cureus.42257
-
Wang L, Lv S, Li F, Bai E, Yang X. Letrozole versus clomiphene citrate and natural cycle: endometrial receptivity during implantation window in women with polycystic ovary syndrome. Front Endocrinol (Lausanne). 2021;11:532692. doi:10.3389/fendo.2020.532692
-
Mastnak L, Herman R, Ferjan S, Janež A, Jensterle M. Prolactin in polycystic ovary syndrome: metabolic effects and therapeutic prospects. Life (Basel). 2023;13(11):2124. doi:10.3390/life13112124
-
Szukiewicz D. Current insights in prolactin signaling and ovulatory function. Int J Mol Sci. 2024;25(4):1976. doi:10.3390/ijms25041976
-
Kamel A, Halim AA, Shehata M, et al. Changes in serum prolactin level during intracytoplasmic sperm injection, and effect on clinical pregnancy rate: a prospective observational study. BMC Pregnancy Childbirth. 2018;18(1):141. doi:10.1186/s12884-018-1783-4
-
Zhang D, Yuan X, Zhen J, Sun Z, Deng C, Yu Q. Mildly higher serum prolactin levels are directly proportional to cumulative pregnancy outcomes in in vitro fertilization/intracytoplasmic sperm injection cycles. Front Endocrinol (Lausanne). 2020;11:584. doi:10.3389/fendo.2020.00584
-
Xu X, Yang A, Han Y, Wang W, Hao G, Cui N. The association between serum prolactin levels and live birth rates in non-PCOS patients: a retrospective cohort study. PLoS One. 2023;18(11):e0295071. doi:10.1371/journal.pone.0295071
Tables
Table 1. Baseline characteristics of participants
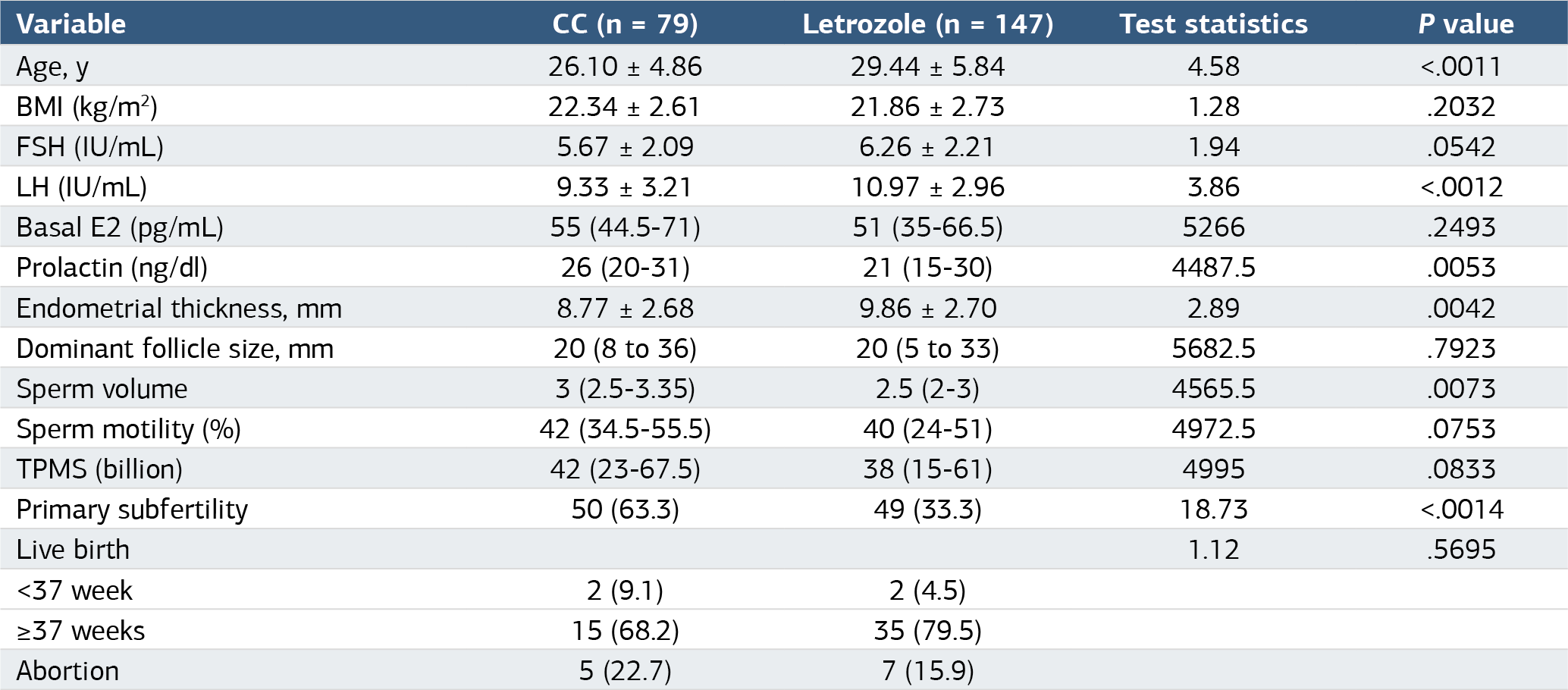
1 Welch’s t-test; 2 student’s t-test; 3 Mann-Whitney U test; 4 Pearson chi-square test; 5 Fisher-Freeman-Halton test. Numerical data were presented as mean ± standard deviation or median with quartiles [1st quartile – 3rd quartile]. Categorical data were described as count (n) and percentage (%). CC: clomiphene citrate, BMI: body mass index, FSH: follicle stimulating hormone, LH: luteinizing hormone, TPMS: total progressive motile sperm.
Table 2. Outcomes for letrozole versus CC as a primary treatment-intention-to-treat analysis
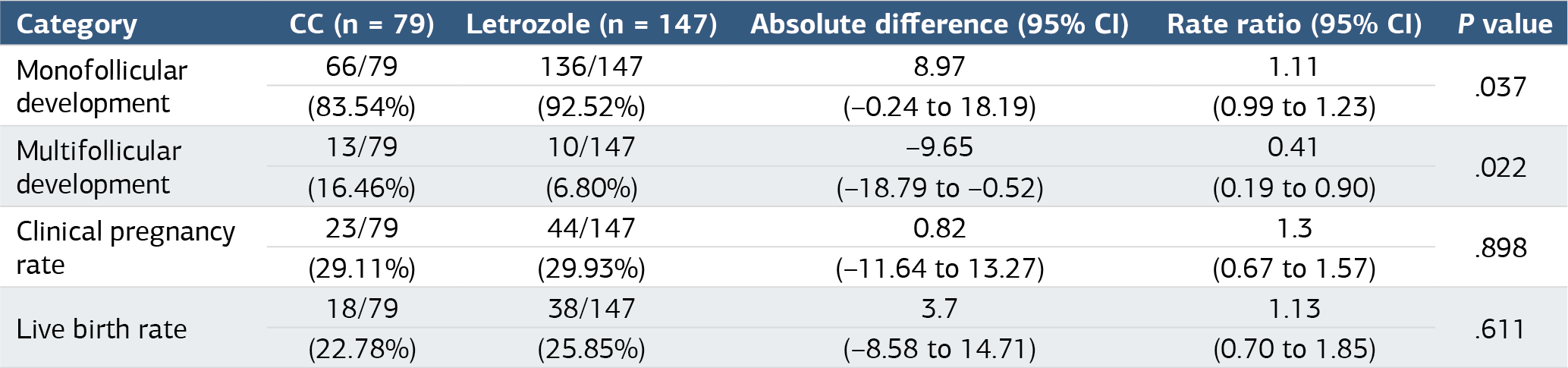
Table 3. Comparison of the characteristics of the clinical pregnancy positive and negative groups
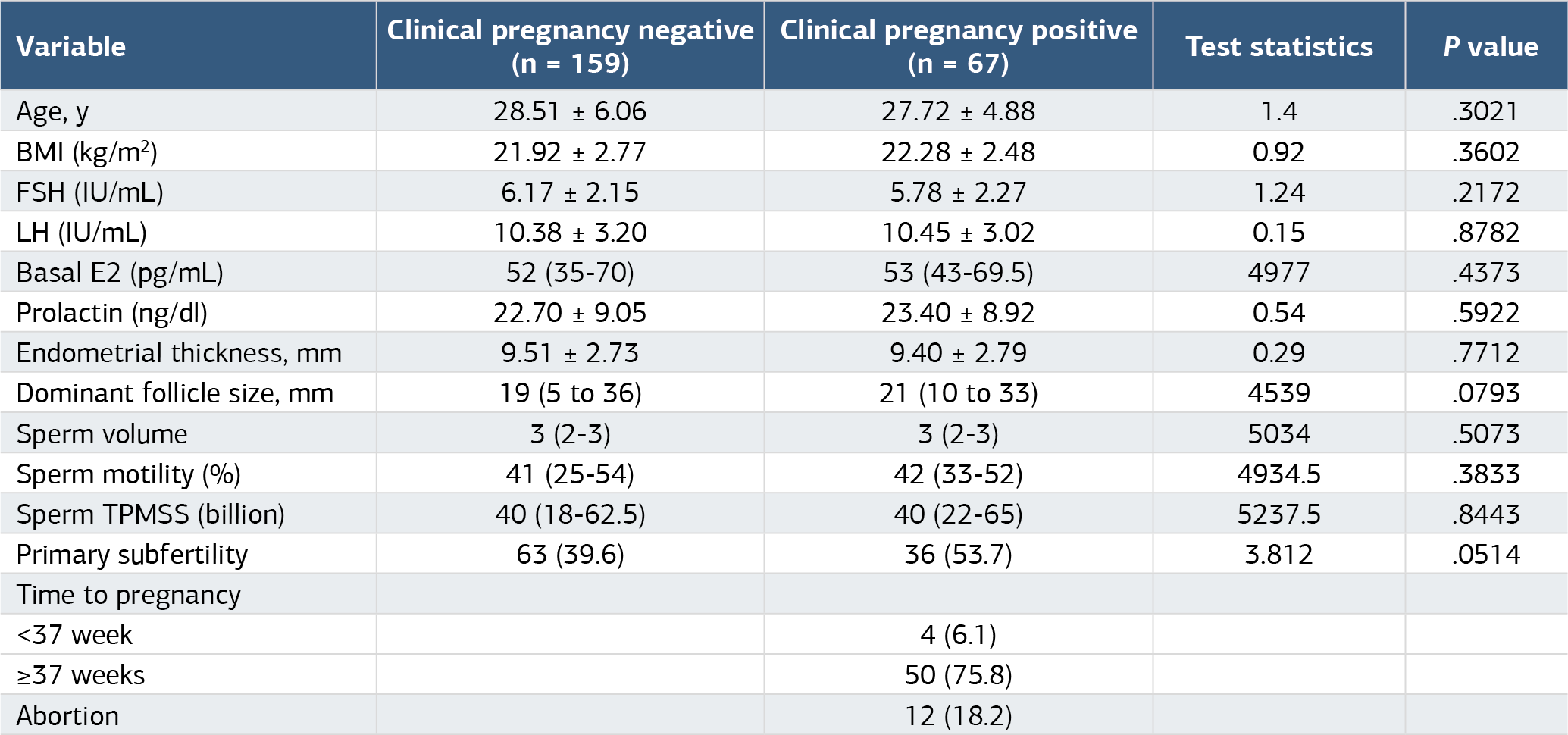
1 Welch’s t-test; 2 student’s t-test; 3 Mann-Whitney U test; 4 Pearson chi-square test Numerical data were presented as mean ± standard deviation or median with quartiles [1st quartile – 3rd quartile]. Categorical data were described as count (n) and percentage (%).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Dilay Gok Korucu, Sevcan Sarıkaya, Melike Unlu, Oguzhan Gunenc, Muslu Kazım Korez. Comparing letrozole versus clomiphene citrate for ovulation induction in polycystic ovary syndrome: a retrospective study. Ann Clin Anal Med 2025;16(4):298-303. doi:10.4328/ACAM.22434
- Received:
- October 3, 2024
- Accepted:
- November 11, 2024
- Published Online:
- November 20, 2024
- Printed:
- April 1, 2025