
Persistence of primary vitreous in premature babies: A Case Report
Persistence of primary vitreous
Authors
Abstract
IntroductionPersistent primary vitreous is a rare congenital ocular anomaly caused by failure of regression of the fetal hyaloid system. It is usually unilateral and detected in full-term infants.
Case PresentationWe report a case of bilateral persistent primary vitreous in a 35-week preterm infant presenting with bilateral leukocoria and mild respiratory distress. Radiological evaluation revealed mild hydrocephalus, colpocephaly, and bilateral persistent primary vitreous. Ophthalmologic examination confirmed persistence of the posterior hyaloid system.
ConclusionPersistent primary vitreous is a rare condition requiring early diagnosis and individualized management to improve visual outcomes.
Keywords
Introduction
Persistent primary vitreous is a congenital anomaly related to the persistence of the fetal hyaloid system and hyperplastic primary vitreous.1 Remnants of the fetal hyaloid system can induce the growth of a fibrovascular retrolental mass of variable size that can impede proper retinal development and lead to varying degrees of microphthalmia accompanied by lens opacification.
It is an isolated and unilateral condition that usually occurs in full-term infants; it is most often revealed by leukocoria. The diagnosis is based on a precise and complete examination of the child’s eye, often under general anesthesia, supplemented by ocular ultrasound. Although the etiology is assumed to be identical in each of its three variants, the persistent hyperplastic vitreous is further subdivided into three clinical forms; this classification depends on the ocular structures affected; we thus distinguish the anterior form, which corresponds to the classic description and the posterior form which is rarer, their association at all possible degrees being the most frequent form clinically. The treatment is adapted to the case by case; amblyopia must be managed throughout the sensitive period. The prognosis of this malformation is both anatomical and functional, in fact, today, the treatment of children with persistent hyperplastic vitreous is focused on the recovery of useful vision as well as obtaining an acceptable aesthetic result.
In this work, we report a case of bilateral persistence of the primary vitreous in a premature baby of 35 weeks of amenorrhea, which manifested at birth by bilateral leukocoria.
Case Presentation
It was a premature baby of 35 weeks of the female sex, 2nd of a family of 2 of a mother aged 27, born to 1st-degree consanguineous parents, by vaginal delivery at the end of pregnancy followed complicated by a threat of premature delivery with the notion of premature rupture of membranes of 3 days, clear amniotic fluid, the mother was immune to toxoplasmosis and rubella and had in the history three spontaneous abortions. The Apgar score was 9 to 1,10 to 5,10 at 10 min of life. From birth, we noticed early respiratory distress (Silverman 1/10) and bilateral leukocoria. On clinical examination, there was no malformation syndrome.
The radiological assessment revealed slight hydrocephalus on transfontanellar ultrasound and colpocephaly associated with the persistence of the bilateral primary vitreous on a brain scan (Figure 1).
Ophthalmologic examination showed persistence of the posterior hyaloid system in the vitreous cavity (Figure 2).
Surgical treatment is discussed for our patient.
Ethical ApprovalEthics committee approval was not required for this case report.
Reporting GuidelinesThis case is reported in accordance with the CARE guidelines.
Discussion
Persistent primary vitreous is a rare condition; its incidence is estimated at 1/30,000 births, and its frequency is underestimated because a certain number of them are probably considered a simple cataract. It usually occurs in children without family or personal history, born at term after a normal pregnancy. Our work concerns a case of prematurity.
In most cases, hyperplastic persistence of the primary vitreous is most often unilateral (90%),1 persistence of the bilateral primary vitreous is rare and occurs only in 10%.
As reported in the literature, diagnosis is usually early. Immediately after birth or in the first weeks of life.2
Three main forms of clinical expression can occur: anterior, posterior (this is the case of our patient), and mixed or combined, 25% of hyperplastic persistences of the primary vitreous are purely anterior, in this form, the posterior pole is entirely normal. The posterior form represents 12% of hyperplastic persistences of the primary vitreous in the literature, and in contrast to the clinical presentation of the anterior form, posterior persistence of the primary vitreous involves relative involvement of the posterior pole. The mixed or combined form is the most frequent, with 77% in the Alexandrakis et al. series and 63% in others.
For many authors, the spontaneous evolution of typical forms of persistent primary vitreous inevitably ends in severe complications (glaucoma, hemorrhages, retinal detachment, uveitis) requiring evisceration or enucleation.3
On the contrary, other publications have shown that this condition is not always progressive and that some unoperated eyes would reach adulthood in a better condition than if they had undergone surgery with all its iatrogenic risks.3
Therapeutic management of primary vitreous aims to restore vision by clearing the visual axis and to avoid complications that can lead to enucleation (or evisceration).4
Limitations
This report describes a single case, which limits the generalizability of the findings.
Conclusion
Persistent vitreous is a rare ocular abnormality whose origin remains unknown. All studies support the value of early diagnosis and early intervention to maximize visual potential. Management varies according to studies, and indications are not codified.
Declarations
Ethics Declarations
The authors declare that all procedures performed in this study were conducted in accordance with institutional, national, and international ethical standards.
Animal and Human Rights Statement
All procedures involving human participants were conducted in accordance with the Declaration of Helsinki and its later amendments.
Informed Consent
Written informed consent for publication was obtained from the patient’s legal guardian.
Data Availability
The authors are responsible for the scientific content of the manuscript, including study design, data collection, analysis, manuscript preparation, and approval of the final version.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: F.Z.A., A.B.
Methodology: F.Z.A., I.E.
Investigation: F.Z.A., L.E.L., I.Z.
Data curation: F.Z.A.
Writing – original draft: F.Z.A.
Writing – review & editing: I.E., N.A., A.B.
Supervision: A.B.
Abbreviations
CT: Computed tomography
NICU: Neonatal intensive care unit
PFV: Persistent fetal vasculature
References
-
Silbert M, Andrew S, Gurwood. Persistent hyperplastic primary vitreous: Clinical review; Clin. Eye Vision Care . 2000;12(1):131-137. doi:10.1016/s0953-4431(00)00054-0
-
Kumar A, Jethani J, Shetty S, Vijayalakshmi P. Bilateral persistent fetal vasculature: A study of 11 cases. J. AAPOS. 2010;14(1):345-348. doi:10.1016/j.jaapos.2010.05.007
-
Ahmiti I, Ahbeddou S, El khaoua M, Tzili N, Alami F, Bencherifa F, et al. Persistance du vitré primitif chez le prématuré. Maroc Médical. 2013;35(4):253-261.
-
Hamdi R, Krifa F, Ferid Z, Eloumari K, Yacoubi S, Knani L, et al. L’hyperplasie du vitre primitif : Prise en charge therapeutique.[Primitive vitreous hyperplasia: Therapeutic management]J. Fr. Ophtalmol. 2008;31(Suppl.):70. doi:10.1016/s0181-5512(08)70781-2
Figures
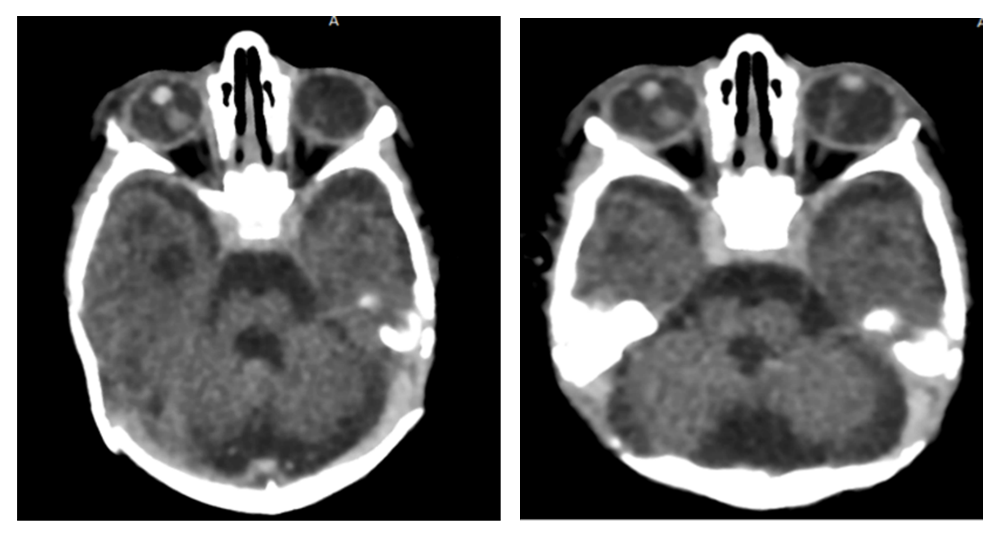
Figure 1. Transverse CT sections showing persistence of bilateral primary vitreous
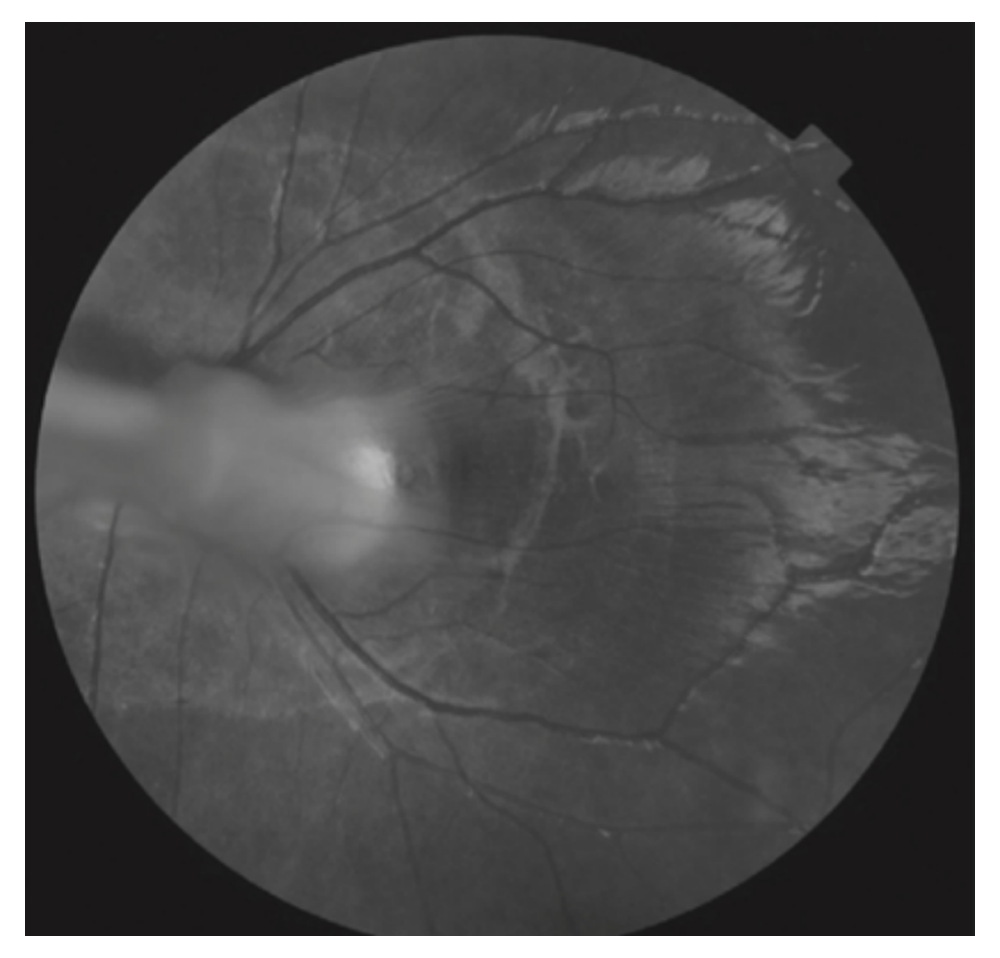
Figure 2. Hyperplastic persistence of the primitive vitreous in its posterior form: papillary attachment band extending towards the temporal region
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Fatima Zahra Arif, İlham Elouardighi, Lamiae El laziji, Imane Zizi, Najat Amalik, Amina Barkat. Persistence of primary vitreous in premature babies: A Case Report. Ann Clin Anal Med 2026;17(6):638-640. doi:10.4328/ACAM.22435
- Received:
- October 3, 2024
- Accepted:
- January 13, 2025
- Published Online:
- February 10, 2025
- Printed:
- June 1, 2026