
Effect of bispectral index monitoring on desflurane consumption, extubation and recovery times in anesthesia management for arthroscopic surgery
Bispectral index in arthroscopy
Authors
Abstract
AimThe bispectral index (BIS) assesses the hypnotic effects of anesthetic agents. It has been reported that the incidence of postoperative cognitive dysfunction is reduced, and wake-up and recovery times are shortened with the use of BIS monitoring. The aim was to evaluate the effect of BIS monitoring on hemodynamic parameters, recovery times, and desflurane consumption in patients who underwent arthroscopic surgery.
MethodsThe patients were classified into two groups: the control group, which received standard anesthesia monitoring, and the BIS group, which received both standard and BIS monitoring. The two groups were compared in terms of hemodynamic parameters, desflurane consumption, spontaneous eye-opening time, recovery time, and side effects.
ResultsThere were no significant differences between the groups in terms of the course of perioperative hemodynamic parameters over time. The groups were comparable regarding side effects, including hypotension, nausea, vomiting, bradycardia, and laryngospasm. Spontaneous eye-opening time and recovery time were shorter in the BIS group. The amount of desflurane consumed per unit time was found to be lower in the BIS group.
ConclusionBIS monitoring shortened desflurane consumption, spontaneous eye-opening, and recovery times, indicating that BIS monitoring can be safely used to monitor the depth of anesthesia by providing ideal inhalation anesthetic titration.
Keywords
Introduction
Balanced anesthesia, in other words, appropriate depth of anesthesia, has three main components: adequate analgesia, hypnosis, and muscle relaxation. As known, very deep anesthesia can cause unwanted hemodynamic changes, while very light anesthesia carries a high risk of awareness.1 Therefore, monitoring the depth of anesthesia is of great importance during any surgical procedure, particularly for preventing awareness. In this context, the bispectral index (BIS), based on the analysis of the electroencephalogram (EEG) of patients, is the first FDA-approved method to assess the hypnotic effects of anesthetic agents.2 BIS is a parameter that measures the level of sedation, loss of consciousness, and recall, ranging from 0, an indicator of complete brain inactivity, to 100, an indicator of alertness. BIS values between 40 and 60 represent adequate general anesthesia for surgery and prevent awareness. In addition, the amount of anesthetic drug is reduced, and postoperative alertness becomes better with the use of BIS monitoring. Moreover, it has been reported that wake-up and recovery times are shortened, the incidence of postoperative cognitive dysfunction and delirium is reduced, and hospital costs are decreased without an increase in undesirable clinical responses.3,4,5,6,7
In this study, the effect of BIS monitoring on hemodynamic parameters, desflurane consumption, wake-up, and recovery times was aimed to be evaluated in patients who underwent elective arthroscopic surgery.
Materials and Methods
Patient SelectionAfter obtaining approval from the local ethics committee, adult patients who were scheduled for elective arthroscopic meniscopathy surgery in Ankara Numune Training and Research Hospital were included in the study. All patients were informed about the operation and anesthesia methods preoperatively. The patients were randomly and equally assigned to two groups: the control group, which received standard anesthesia monitoring (non-invasive blood pressure, ECG, SpO₂, and EtCO₂), and the BIS group, which received both standard and BIS monitoring. The two groups were compared in terms of perioperative hemodynamic parameters, anesthetic inhalation agent (desflurane) consumption, spontaneous eye-opening, and recovery times.
The patients less than 18 years old, who had ≥3 ASA status, central neurological disease, and drug (anticonvulsant) sensitivity that may affect the neurological response, chronic drug (opioid, benzodiazepine, etc.) and alcohol use, and those with mean arterial pressure (MAP) above 60 mmHg and heart rate (HR) below 50 beats/minute were excluded from the study. If the operation lasted less than 20 minutes or more than 60 minutes, data from those patients were also excluded from the statistical analysis.
Anesthesia ManagementAll patients fasted for at least 8 hours before the operation. In order not to affect the BIS value, sedative premedication was not applied. In all patients, 0.9% NaCl infusion was started through the back of the hand, and 0.5 mg atropine was administered. The patients were randomly divided into two groups: the control group, who received standard routine anesthesia, and the BIS group. Standard monitoring included electrocardiogram (ECG), HR, MAP, peripheral oxygen saturation (SpO₂), and end-tidal carbon dioxide (EtCO₂) values. In addition, BIS values were measured with Aspect Medical system A-2000 and BIS sensor in the BIS group.
All patients were preoxygenated with 100% oxygen for 3 minutes, and initial monitoring values were recorded. During anesthesia induction, a bolus of 2 µg/kg fentanyl and 2 mg/kg propofol was administered. After ensuring sufficient depth of anesthesia, the appropriate laryngeal mask was placed.
For anesthesia maintenance, 4 L/min oxygen-nitrous oxide mixture (40% O₂-60% N₂O) and 2-6% desflurane were given in the first 5 minutes. Meanwhile, hemodynamic parameters and BIS values were recorded. Then, the O₂-N₂O mixture was reduced to 2 L/min in both groups. Hemodynamic parameters and BIS values were also noted every 10 minutes from the incision to the end of the surgery. The depth of anesthesia was evaluated according to the changes in hemodynamic parameters in the control group and BIS values (keeping between 40 and 60) in the BIS group. In both groups, 0.5 µg/kg fentanyl was administered 3 minutes before the incision to suppress the sensation related to the surgical incision, and the desflurane flow percentage was increased by an average of 2% (range 2-6%).
In the presence of findings indicating superficial anesthesia (20% increase in systolic pressure compared to the initial value, 20% increase in heart rate in one minute, sweating, tears, significant movement, swallowing, eye-opening, grimacing) or if the BIS value is 60 and above, the anesthetic gas concentration increased by 25%. If the findings persisted, 0.5-1 µg/kg fentanyl was given.
If the changes in hemodynamic parameters were high or low but the depth of anesthesia was sufficient (that is, the BIS value was between 40 and 60 in the BIS group, and there was no movement in the control group), auxiliary anesthesia drugs were used. If systolic artery pressure was 20% above the baseline value, 0.1 mg IV permanganate was administered. When a 20% decrease in systolic artery pressure compared to the initial value was observed, 10 mg IV ephedrine was administered, and if HR was below 50/min, 0.01-0.02 mg/kg IV atropine was administered.
At the end of the operation, the time for spontaneous eye opening was recorded. In the BIS group, patients were taken to the recovery room when their BIS scores at the end of surgery were above 90 and close to the initial BIS score. Before removing the laryngeal mask, 10 mg IV metoclopramide was administered to prevent postoperative nausea and vomiting, and 100 mg IV tramadol was given to prevent postoperative pain.
In the postoperative period, patients were evaluated every 5 minutes with the Modified Alderete Postanesthetic Recovery Scoring. The patients who reached 13 or higher scores were sent to their clinics.
Ethical ApprovalThis study was approved by the Ethics Committee of Ankara Numune Training and Research Hospital (Date: 14.09.2005, Decision No: 1).
Statistical AnalysisData analysis was done using the SPSS package program. Continuous variables were shown as mean and standard deviation, while categorical variables were presented as frequency and percentage. The Repeated Measures Analysis of Variance was used to evaluate whether the changes in HR, MAP, SPO₂, and ETCO₂ levels during the follow-ups, the differences between the groups, and whether the effect of the group on the changes occurring over time was statistically significant. Mann Whitney U test was used to compare the groups in terms of age, spontaneous eye-opening time, and recovery time. Differences in terms of anesthesia duration and amount of desflurane consumed per unit time (ml/min) were examined using Student’s t-test. A value of p<0.05 was considered statistically significant.
Reporting GuidelinesThis study was reported in accordance with the CONSORT guideline.
Results
A total of 40 patients with a mean age of 38.2 years old were randomly and equally assigned to two groups: a control group and the BIS group. The groups were statistically similar in terms of age, gender, ASA status, body mass index, and anesthesia time (p>0.05).
In both groups, HR, MAP, SpO₂, and EtCO₂ values were recorded at those times: before induction (baseline), during induction, just after LMA insertion, 10 minutes after LMA insertion, during incision, 10 minutes after incision, after LMA removal, and during recovery (Figure 1A).
In the statistical analysis of HR, the change in HR over time was found to be statistically significant (p<0.001). In both the control group and BIS group, HR values measured after LMA insertion, at the 10th minute of LMA insertion, and during the incision were significant compared to the baseline values (p<0.01). There was no statistically significant difference between the groups in terms of the course of HR over time (p=0.653).
In the statistical analysis of MAP, the change in MAP over time was found to be statistically significant (p<0.001). In both groups, MAP values measured after LMA insertion, at the 10th minute of LMA insertion, and during the incision were lower and significant compared to the baseline values (p<0.01). MAP values measured after the incision were found to be similar to the baseline values in both groups (p>0.05). There was no statistically significant difference between the groups in terms of the course of MAP over time (p=0.899) (Figure 1B).
In statistical analysis of SpO₂ , the change in SpO₂ over time was found to be borderline statistically significant (p=0.003). In both groups, there was an increase in SpO₂ values during induction and after LMA compared to the initial SpO2 values, but it was not statistically significant (p>0.01). There was no statistically significant difference between the groups in terms of the course of SpO₂ over time (p=0.604) (Figure 1C).
In statistical analysis of ETCO₂ measurements, the change in ETCO₂ over time was found to be statistically significant (p<0.001). In the control group, there was a significant decrease at the 10th minute of LMA insertion, during and after the incision, compared to the baseline ETCO₂ values (p<0.01). The change in ETCO₂ values measured in the BIS group was not significant in comparison to the baseline ETCO₂ values (p>0.01). There was no statistically significant difference between the groups in terms of the course of ETCO₂ over time (p=0.675) (Figure 1D).
Both groups were compared with each other in terms of side effects (Table 1). The most frequent side effect was hypotension. Six patients in the control group and four patients in the BIS monitoring group developed hypotension, all of whom were easily treated with adequate fluid support and vasoactive drugs (ephedrine) when necessary. The second most common side effect was nausea/vomiting. Although antiemetic prophylaxis (10 mg IV metoclopramide before LMA removal) was routinely administered, postoperative nausea and vomiting were observed in five patients in the control group and three patients in the BIS group. All of those patients were successfully treated with additional antiemetic medication. Laryngospasm, which developed during LMA removal in one patient in each group, was corrected with pressurized O₂ .
Finally, the groups were compared in terms of spontaneous eye-opening time, recovery time, and amount of desflurane consumed per unit time (mL/min). Spontaneous eye-opening time and recovery time were shorter in the BIS group (p=0.041 and p=0.014, respectively). The amount of desflurane consumed per unit time was found to be lower in the BIS group (p=0.008) (Table 2).
Discussion
Unpredictable and unwanted responses associated with anesthetic agents carry potential risks for anesthesiologists. Today, there is no ideal anesthetic agent that provides appropriate depth of anesthesia, causes early and rapid recovery, and has a minimal side effect profile. In addition, the exact dosage of anesthetics to be administered remains a great challenge. To date, clinical symptoms such as corneal and eyelash reflexes, pupil size, pupil reaction to light, tearing, eyeball movements, hemodynamic parameters such as blood pressure and heart pulse, and motor response to skin incision have been used to determine the depth of anesthesia. The hemodynamic changes are not sufficient to determine the depth of anesthesia because they can be affected by many factors. Over the last two decades, BIS, which shows electrical activity in the deep cortical brain layers, has become increasingly used in the evaluation of the depth of anesthesia.8,9 However, there are many studies with conflicting results regarding the benefits of BIS monitoring. It should be stated here that some of those conflicting results are related to inappropriate study designs, including different patient populations and different anesthesia protocols. In the present study, the BIS and control groups consisted of patients with similar clinical and surgical features. The hemodynamic parameters were then compared between the groups. The fact that basic hemodynamic changes in both groups were statistically similar also allowed us to provide more accurate statistical analyses. Burrow et al. also found that patients who underwent BIS monitoring had better respiratory functions and were more alert and more active when they came to the recovery room. Additionally, hemodynamic data in the BIS group were closer to preoperative values compared to other patients.3
The main focus of our study was whether the use of BIS monitoring was beneficial in three parameters related to anesthesia management, including spontaneous eye-opening time, recovery time, and amount of desflurane consumed per unit time. Besides, side effects related to anesthetics were the other endpoint in the present study. According to the results obtained from the study, BIS monitoring provided significant reductions in spontaneous eye-opening time, recovery time, and amount of desflurane consumed.
The value of BIS in evaluating the depth of anesthesia has been proven by many studies.9,10,11,12,13 In those works, keeping the BIS values under 60 during anesthesia was reported to be essential for adequate hypnosis and preventing awareness.9,14 In parallel, BIS values were between 40 and 60 in all patients, and the course of the BIS values was almost always consistent with the clinical parameters. In addition, all patients in both groups stated that they did not remember anything about the operation when questioned in the postoperative period.
In previous studies, BIS was found to be a good monitoring method to evaluate loss of consciousness caused by different anesthetic agents such as thiopental, propofol, midazolam, and isoflurane.15,16,17 We used propofol for anesthesia induction and desflurane for maintenance. In our study, time for spontaneous eye opening was one of the primary endpoints and was found to be significantly reduced in the BIS group compared to the non-BIS group. Similarly, BIS monitoring provided a reduction in time for spontaneous eye-opening in the majority of clinical studies.15,18,19,20
In our study, recovery time was also found to be decreased in the BIS group, consistent with the majority of previous studies.20,21 It is well known that recovery time can be affected by the duration of anesthesia. In our study, there was no significant difference between the groups in terms of anesthesia time. Johansen and Sigl reported in their studies that patients’ extubation times were shortened, and hospital costs were reduced by using BIS monitoring.22
In the literature, several studies reported that the use of BIS caused a decrease in the consumption of anesthetic drugs.21,23 Similarly, we found that desflurane consumption was significantly lower in the BIS monitoring group compared with the control group. As known, high-dose desflurane is associated with serious side effects such as airway irritation, cough, and laryngospasm. In our study, only one patient in each group developed laryngospasm during laryngeal mask removal and was treated with pressurized oxygen. Desflurane also causes postoperative nausea and vomiting due to its irritating smell. A meta-analysis showed that the use of BIS monitoring in patients undergoing outpatient anesthesia reduced the likelihood of nausea and vomiting by 38%.23 In our study, the patients in the BIS monitoring group had developed less postoperative nausea and vomiting, although not statistically significant.
The use of IV fluids and anticholinergics has been recommended to prevent hypotension and bradycardia that may occur during the use of opioids and desflurane.24 In our study, all cases were given 7 ml/kg of IV fluid and 0.5 mg atropine before the operation. No statistically significant difference was observed between the groups in terms of the development of hypotension and bradycardia. Postoperative pain, nausea, and vomiting are among the most important reasons for delayed patient discharge. Therefore, titrating general anesthetics with BIS monitoring may reduce these side effects and shorten discharge times.23 However, discharge time was not evaluated in our study.
Limitations
The single-center design and small sample size are the main limitations of this study.
Conclusion
There was no significant difference between the BIS monitoring group and the standard monitoring group in terms of perioperative hemodynamic parameters and side effects. However, BIS monitoring shortened desflurane consumption, spontaneous eye opening, and recovery times, indicating that BIS monitoring can be safely used to monitor the depth of anesthesia by providing ideal inhalation anesthetic titration.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
ASA: American Society of Anesthesiologists
BIS: Bispectral index
ECG: Electrocardiogram
EtCO₂: End-tidal carbon dioxide
HR: Heart rate
LMA: Laryngeal mask airway
MAP: Mean arterial pressure
SpO₂: Peripheral oxygen saturation
References
-
Froese L, Dian J, Gomez A, et al. Association between processed electroencephalogram-based objectively measured depth of sedation and cerebrovascular response: a systematic scoping overview of the human and animal literature. Front Neurol. 2021;12:692207. doi:10.3389/fneur.2021.692207
-
Li Z, Cai J, Li J, Xu X, Zheng L. Comparative evaluation of the bispectral index and BISpro during propofol anaesthesia. J Int Med Res. 2021;49(4):3000605211001705. doi:10.1177/03000605211001705
-
Burrow B, McKenzie B, Case C. Do anaesthetized patients recover better after bispectral index monitoring? Anaesth Intensive Care. 2001;29(3):239-245. doi:10.1177/0310057x0102900303
-
Lewis SR, Pritchard MW, Fawcett LJ, Punjasawadwong Y. Bispectral index for improving intraoperative awareness and early postoperative recovery in adults. Cochrane Database Syst Rev. 2019;9(9). doi:10.1002/14651858.cd003843.pub4
-
Long Y, Feng X, Liu H, et al. Effects of anesthetic depth on postoperative pain and delirium: a meta-analysis of randomized controlled trials with trial sequential analysis. Chin Med J (Engl). 2022;135(23):2805-2814. doi:10.1097/cm9.0000000000002449
-
Sumner M, Deng C, Evered L, et al. Processed electroencephalography-guided general anaesthesia to reduce postoperative delirium: a systematic review and meta-analysis. Br J Anaesth. 2023;130(2). doi:10.1016/j.bja.2022.01.006
-
Xie T, Wang Y, Liu Y, Li J, Li W, Xu H. Accuracy of closed-loop and open-loop propofol delivery systems by bispectral index monitoring in breast surgery patients: a prospective randomized trial. Braz J Anesthesiol. 2024;74(2):744438. doi:10.1016/j.bjane.2023.05.003
-
Kabukcu HK, Sahin N, Ozkaloglu K, Golbasi I, Titiz TA. Bispectral index monitoring in patients undergoing open heart surgery. Braz J Cardiovasc Surg. 2016;31(2):178-182. doi:10.5935/1678-9741.20160038
-
McGuigan S, Scott DA, Evered L, Silbert B, Liley DTJ. Performance of the bispectral index and electroencephalograph-derived parameters of anesthetic depth during emergence from xenon and sevoflurane anesthesia. J Clin Monit Comput. 2023;37(1):71-81. doi:10.1007/s10877-022-00860-y
-
Rosow C, Manberg PJ. Bispectral index monitoring. Anesthesiol Clin North Am. 2001;19(4):947-966. doi:10.1016/s0889-8537(01)80018-3
-
Lysakowski C, Dumont L, Pellegrini M, Clergue F, Tassonyi E. Effects of fentanyl, alfentanil, remifentanil, and sufentanil on loss of consciousness and bispectral index during propofol induction of anaesthesia. Br J Anaesth. 2001;86(4):523-527. doi:10.1093/bja/86.4.523
-
Choi WJ, Kim YH. How do you use bispectral index effectively for preventing re-awareness during general anesthesia? Korean J Anesthesiol. 2012;62(1):1-2. doi:10.4097/kjae.2012.62.1.1
-
Okamoto A, Kamata K, Miyata T, et al. Bispectral index-guided propofol sedation during endoscopic ultrasonography. Clin Endosc. 2022;55(4):558-563. doi:10.5946/ce.2022.001
-
Myles P, Leslie K, McNeil J, Forbes A, Chan MT. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet. 2004;363(9423):1757-1763. doi:10.1016/s0140-6736(04)16300-9
-
Aimé I, Verroust N, Masson-Lefoll C, et al. Does monitoring bispectral index or spectral entropy reduce sevoflurane use? Anesth Analg. 2006;103(6):1469-1477. doi:10.1213/01.ane.0000246838.93153.23
-
Park JH, Lee SE, Kang E, et al. Effect of depth of anesthesia on the phase lag entropy in patients undergoing general anesthesia by propofol: a STROBE-compliant study. Medicine (Baltimore). 2020;99(30). doi:10.1097/md.0000000000021303
-
Yoo JH, Ok SY, Kim SH, et al. Comparison of bispectral index and phase lag entropy during general anesthesia: sevoflurane or propofol anesthesia. Medicine (Baltimore). 2022;101(44). doi:10.1097/md.0000000000031191
-
Ibraheim O, Alshaer A, Mazen K, et al. Effect of bispectral index monitoring on postoperative recovery and sevoflurane consumption among morbidly obese patients undergoing laparoscopic gastric banding. Middle East J Anaesthesiol. 2008;19(4):819-830.
-
Kamal NM, Omar SH, Radwan KG, Youssef A. Bispectral index monitoring tailors clinical anesthetic delivery and reduces anesthetic drug consumption. J Med Sci. 2009;9(1):10-16.
-
Chiang MH, Wu SC, Hsu SW, Chin JC. Bispectral index and non-bispectral index anesthetic protocols on postoperative recovery outcomes. Minerva Anestesiol. 2018;84(2):216-228. doi:10.23736/s0375-9393.17.12033-x
-
Oliveira CR, Bernardo WM, Nunes VM. Benefit of general anesthesia monitored by bispectral index compared with monitoring guided only by clinical parameters: systematic review and meta-analysis. Braz J Anesthesiol. 2017;67(1):72-84. doi:10.1016/j.bjane.2015.09.001
-
Klopman MA, Sebel PS. Cost-effectiveness of bispectral index monitoring. Curr Opin Anaesthesiol. 2011;24(2):177-181. doi:10.1097/aco.0b013e328343eb19
-
Liu SS. Effects of bispectral index monitoring on ambulatory anesthesia: a meta-analysis of randomized controlled trials and a cost analysis. Anesthesiology. 2004;101(2):311-315. doi:10.1097/00000542-200408000-00010
-
Guignard B, Menigaux C, Dupont X, Fletcher D, Chauvin M. The effect of remifentanil on the bispectral index change and hemodynamic responses after orotracheal intubation. Anesth Analg. 2000;90(1):161-167. doi:10.1097/00000539-200001000-00034
Figures
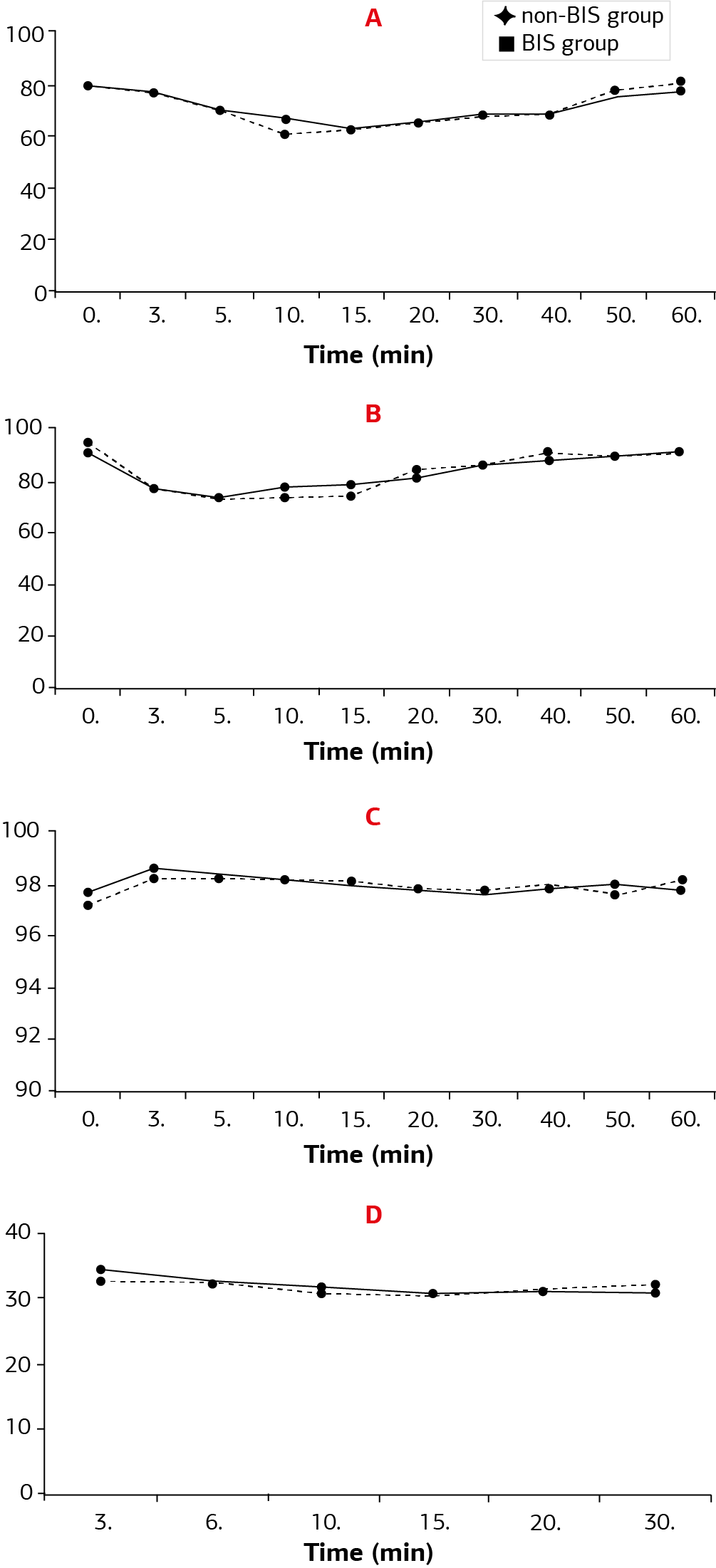
Figure 1. The courses of (A) HR, (B) MAP, (C) SpO₂, and (D) EtCO₂ during the anesthesia period
Tables
Table 1. Comparison of the two groups in terms of side effects
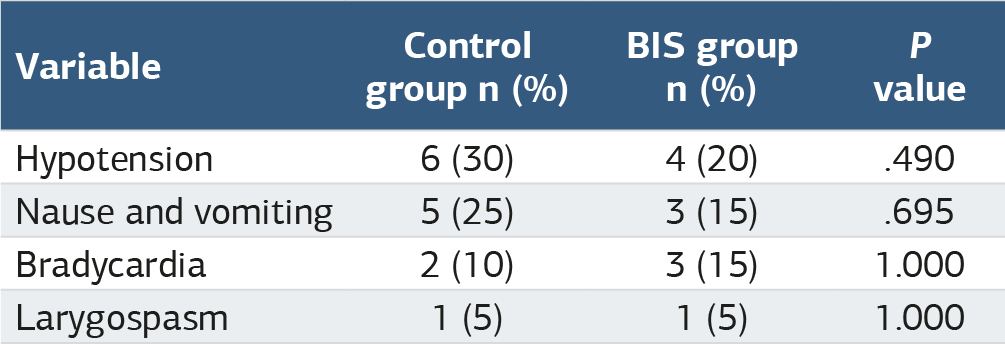
Table 2. Comparison of the two groups in terms of spontaneous eye-opening time, recovery time, and amount of desflurane consumed per unit time (mL/min)

Desflurane consumption was defined as the amount of desflurane consumed per unit of time min: minute, mL: mililiter.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Sadık Özkavak, Hatice Adsan, Yeliz Kılıç, Pınar Erdaloğlu, Nermin Göğüş. Effect of bispectral index monitoring on desflurane consumption, extubation and recovery times in anesthesia management for arthroscopic surgery. Ann Clin Anal Med 2025;16(4):304-308. doi:10.4328/ACAM.22446
- Received:
- October 9, 2024
- Accepted:
- November 18, 2024
- Published Online:
- November 25, 2024
- Printed:
- April 1, 2025