
The prognostic role of whole blood viscosity and bone marrow fibrosis inpredicting survival outcomes in new diagnosis multiple myeloma patients
Blood viscosity and fibrosis in myeloma
Authors
Abstract
AimThis study aimed to evaluate the prognostic role of whole blood viscosity and bone marrow fibrosis in predicting survival outcomes and relationships with prognostic predictors, such as international scoring system albumin levels, beta2-microglobulin, total protein, albumin, and lactate dehydrogenase in newly diagnosed multıple myeloma patients.
MethodsWe retrospectively evaluated 108 patients diagnosed with multıple myeloma between 2015-2022. Whole blood viscosity was calculated using the Simone formula, incorporating the hematocrit and total protein values. Bone marrow fibrosis was graded as mild ‘2’, significant ‘3’, or advanced. Comparisons of grade 0-3 bone marrow fibrosis and high-low calculated whole blood viscosity groups in terms of overall survival were conducted using the Kaplan-Meier survival curve and log-rank test.
ResultsThe median follow-up period was 16 months, and 57.4% of patients died during follow-up. The median overall survival was 26 months. The calculated whole blood viscosity (c-WBV) value predicted mortality with 88.7% sensitivity and 45.7% specificity. Patients with a high c-WBV (≥17.14 208 mPa-s) had significantly lower one- and two-year survival rates than those with a low c-WBV (<17.14 208 mPa-s) (p<0.001). Bone marrow fibrosis was inversely related to survival, with higher grades being associated with lower survival rates. The two-year expected survival time, respectively, bone marrow fibrosis 2 and 3 was determined to be 56.7%, 43.6%, 41.4%, and 23.3% (p<0.001).
ConclusionThis study highlights the potential of whole blood viscosity and bone marrow fibrosis as prognostic markers in patients with newly diagnosed multiple myeloma patients. Incorporating these parameters into the existing staging systems may enhance prognostic prediction and guide treatment decisions. Further prospective studies are warranted to validate these findings and explore the mechanistic links between whole blood viscosity, bone marrow fibrosis, and MM pathophysiology.
Keywords
Introduction
Multiple myeloma (MM) is a blood cancer marked by abnormal plasma cell proliferation inside and outside the bone marrow. It accounts for 1% of all cancers and 10% of hematologic cancers. In 2022, there were 187,952 new cases and 121,388 deaths. MM predominantly affects males over 50, causing complications like renal failure, hypercalcemia, anemia, immune deficits, bone lesions, hyperviscosity syndrome, and neuropathy.1,2 Prognostic factors, including the International Scoring System (ISS) and Durie–Salmon classification, guide treatment planning and life expectancy predictions. ISS uses albumin (alb) and β2-microglobulin (β2mg) to classify MM into three stages, with stage III having a life expectancy of 29 months, half that of stage I.3 In 2015, the Revised ISS (R-ISS) added serum lactate dehydrogenase (LDH) and chromosomal abnormalities.4 In 2022, the European Myeloma Network (EMN) introduced R2-ISS, adding the chromosomal abnormality 1q+ and defining four categories.5
Hemorheology, which examines the flow and deformation of blood and its elements, has been extensively studied in MM patients compared to healthy individuals. The most common irregularities in MM are anemia and elevated erythrocyte sedimentation rate, while leukopenia and thrombocytopenia are less frequent.6 Hemorheological assessments show increased whole blood and plasma viscosities and decreased erythrocyte deformability in MM patients. A relationship exists between measured plasma viscosity and calculated WBV (c-WBV).7 WBV is crucial in MM pathophysiology, influencing thrombotic event risk and clinical management. The IMPEDEVTE score indicated increased calculated blood viscosity in patients at “intermediate+high” risk. Although low albumin and ISS III suggest potential as predictive markers for WBV, statistical significance was not achieved. Nevertheless, WBV and thrombosis relationships can predict prognosis.8
Bone marrow fibrosis (BMF) is influenced by nonmalignant, clonal, or nonclonal neoplastic cells, resulting from cytokines and growth factors like FGF, TGF-β, and BMP released by malignant hematopoietic stem cells. Myelofibrosis involves the activation of cellular fibrogenic pathways, causing excessive extracellular matrix deposition. Effector cells facilitate mesenchymal stem cell differentiation and production of extracellular matrix and collagen.9 Elevated BMF leads to increased apoptosis in the bone marrow niche, impaired cellular proliferation, and increased extramedullary and medullary hematopoiesis. BMF was found in 38% of MM patients, who had a reduced life expectancy of 4.4 to 5 years compared to those with low or no fibrosis.10
Recently, hemorheological parameters have gained importance in MM and various hematological cancers. WBV is a critical factor, especially relevant in hyperviscosity. Our study retrospectively calculated WBV for MM patients diagnosed at our center, evaluating the results concerning fibrosis, an indicator of the bone marrow microenvironment. We aimed to include WBV as a prognostic parameter in MM patients and explore the correlation between BMF, hemorheological profile, and survival analyses in the literature.
Materials and Methods
We retrospectively evaluated 108 MM patients diagnosed between 2015 and 2022 at Afyonkarahisar Health Sciences University Medical Faculty Hospital. The cohort included 65 males and 43 females, all over the age of 18. Exclusion criteria included infectious diseases, end-stage liver failure, rheumatic and autoimmune diseases, non-MM hematological or oncological malignancies, solitary plasmacytomas, and those receiving active chemotherapy and steroid treatment. MM was diagnosed according to its subtypes by bone marrow biopsy. We assessed hemoglobin concentration (HGB), hematocrit (HCT), platelet count (PLT), total protein (TP), alb, creatinine (Crea), lactate dehydrogenase (LDH), calcium (Ca+2), β2mg, and C-reactive protein (CRP) using the Cobas 6000 analyzer (Roche, Switzerland). The ISS classification was based on serum alb and β2mg at diagnosis: serum alb > 3.5 g/dl and β2mg < 3.5 mg/l indicated stage 1 (ISS-1); serum β2mg >5.5 mg/l indicated stage 3 (ISS-3); other cases were stage 2 (ISS-2). Total plasma protein levels, measured in g/L via the colorimetric method, were used to calculate WBV using de Simone’s formula: WBV = (0.12 × HCT) + 0.17 × (TP – 2.0). Bone marrow reports were reviewed for fibrosis presence, evaluated with reticulin staining, and graded 0 to 3: 0 normal, 1 loose, 2 focal bundles, and 3 coarse bundles.
Ethical ApprovalThis study was approved by the Ethics Committee of Afyonkarahisar Health Sciences University (Date: 03.05.2024, Decision No: 2024/89).
Statistical AnalysisCategorical variables are presented as percentages and frequencies. Continuous variables were assessed for normal distribution using visual methods (histograms) and the Shapiro-Wilk test. Normally distributed continuous variables are expressed as mean ± standard deviation (mean ± SD), and non-normally distributed continuous variables are expressed as median (quartile 1-3). The chi-square test and Fisher’s exact test were used to compare categorical variables between groups. The independent samples t-test was used for conditions with normal distribution, and the Mann-Whitney U test was applied for conditions without normal distribution. Receiver operating characteristic (ROC) curves were used to determine the viscosity value that could distinguish between patients who died and those who survived. The Youden index was used to calculate the optimal cutoff value. Comparisons of high- and low-viscosity groups in terms of OS were conducted using the Kaplan-Meier survival curve and log-rank test. All p values were two-sided, and statistical significance was defined as p<0.05. Statistical analyses were performed using the SPSS 26.0 (IBM Corp. 2019 IBM SPSS Statistics for Windows, version 26.0. Armonk, NY: IBM Corp.) package program.
Reporting GuidelinesThe study was reported in accordance with the STROBE guideline.
Results
The study was conducted on 108 patients with MM. The median age of the patients was 68 (Q1-Q3 = 65-74.75) years. Of these, 60.2% (n = 65) were male, and 39.8% (n = 43) were female. The median follow-up period was 16 (Q1-Q3 = 5-38) months.
During follow-up, 57.4% (n = 62) of patients died. The median OS was 26 months (95% CI=16.2-35.8 months). The general characteristics of the surviving and deceased patients are presented in Table 1.
Receiver operating characteristic (ROC) analysis for viscosity demonstrated that a viscosity value of 17.14 could predict mortality with a sensitivity of 88.7% and specificity of 45.7% (AUC = 0.667, 95% CI = 0.558-0.775, p=0.003). Figure 1 illustrates the ROC curve of the predictive power of viscosity for mortality. Subjects were categorized into two groups: those with viscosity ≥ 17.14 and those with viscosity <17.14 and subsequently compared. Of the participants, 74.1% (n = 80) were in the high-WBV group, whereas 25.9% (n = 28) were in the low-viscosity group. Table 2 presents a comparison of the high- and low-viscosity groups.
One- and two-year survival in the high-viscosity group were 59.8% and 40.4%, respectively, while those in the low WBV group were 85.7% and 81.8%, respectively. Overall survival (OS) in the low-WBV group was significantly higher (p<0.001). Figure 2 shows a comparison of survival between the high- and low-viscosity groups.
Upon examination of the effect of reticular fiber degree on survival, no mortality was observed in the cohort with reticular fiber degree “0”. The one- and two-year survival rates for subjects with a reticular fiber degree of “1” were 85.7% and 71.7%, respectively. For those with a reticular fiber degree of “2”, the rates were 56.7% and 43.6%, while for those with a reticular fiber degree of “3”, the rates were 41.4% and 23.3%, respectively. A statistically significant inverse relationship was observed between survival and the degree of reticular fiber (p<0.001). Figure 3 illustrates a comparative analysis of survival among the reticular fiber degree groups.
Discussion
This study provides valuable insights into the prognostic factors affecting survival in patients with MM. The median age of the study cohort was 68 years, and the findings revealed that a significant proportion of patients experienced poor OS, with a median OS of 26 months. The diversity of laboratory findings has identified various prognostic markers, notably through the ISS staging system developed by Greipp, which includes β2-MG and serum albumin. In 2015, the International Myeloma Working Group (IMWG) integrated LDH and cytogenetic features into the ISS.11 One of the primary observations was the strong association between the ISS stage and patient outcomes. Patients in ISS stage III had significantly worse survival compared to those in earlier stages. Low albumin, high β2mg, elevated LDH, and creatinine levels were found to correlate with increased mortality, emphasizing the importance of these parameters in staging and risk stratification. This is consistent with prior studies that demonstrate the prognostic value in MM, as these markers reflect both tumor burden and the patient’s general health status (Table 1). The correlation of these results with studies in the literature was further supported.12
The hypercoagulable state in cancer patients is linked to procoagulant factors (thrombin products, and elevated activity of tissue factor, FVII, FVIII, vWF, fibrinogen, procoagulant phospholipids, IL-6, TNF-α, and M proteins), fibrinolytic, or proteolytic factors from tumor cells and inflammatory cytokines affecting coagulation.13 MM should be considered separately regarding thrombosis due to elevated M proteins, which slow blood flow through increased contact and friction, raising stasis and thrombosis risk. Plasma proteins significantly influence coagulation by affecting blood properties like viscosity and erythrocyte aggregation, though the exact mechanical connections to disease symptoms are not fully understood. Immunoglobulins, a component of total protein, can alter blood viscosity directly or by increasing erythrocyte aggregation, making calculated WBV (c-WBV) particularly relevant in MM patients.14 When plasma viscosity is assessed alongside classical risk factors, its predictive value for cardiovascular disease and mortality is highlighted, enhancing the differentiation between cardiovascular events and mortality, starting from the increased thrombosis risk in MM.15
Increased viscosity leads to intensified inflammation and vascular damage, resulting in elevated NO release, which lowers vascular resistance but can become exhausted and toxic in systemic circulation.16 Besides, high protein levels, changes in erythrocyte behavior, and increased erythrocyte count also affect slow blood flow, a topic largely studied due to its link with higher thrombotic risk in patients, yet its prognostic and survival evaluation remains underexplored. Elevated c-WBV increases the risk of vascular occlusion by slowing blood flow, a crucial factor in thrombosis prognosis.17 Due to the retrospective nature of the study design, direct WBV calculation was not feasible. Instead, the de Simone formula, a simple and non-invasive method incorporating hematocrit and total protein parameters, was used to calculate c-WBV. While this formula may sufficiently evaluate WBV influenced by these factors, it may not fully account for the effects of erythrocyte aggregation and deformability. The literature review revealed no studies on the relationship between c-WBV and mortality in diseases with dysproteinemia. Although limited studies have examined the relationship between WBV and mortality, one study demonstrated significantly higher mortality in COVID-19 patients with high WBV compared to those with low WBV, and another large-scale prospective study highlighted the relationship between plasma and blood viscosity and mortality in heart disease patients.15,18
This study identified c-WBV as a significant mortality predictor. Increased plasma viscosity, a key WBV component, is linked to thrombotic complications and poor outcomes.19,20 Our findings showed a significant difference in mortality rates between groups with high (20.18 ± 3.5) and low c-WBV values (p=0.016) (Table 1). Hemoglobin and total protein values, essential for the Simone formula calculation for c-WBV, were significantly different (p<0.05). ROC analysis confirmed c-WBV’s predictive power for mortality, with a threshold of 17.14 showing 88.7% sensitivity (AUC = 0.667, p=0.003) (Figure 1). The low c-WBV group had significantly higher OS (p<0.001) (Figure 2), with one- and two-year survival rates at 85.7% and 81.8%, respectively, compared to 59.8% and 40.4% in the high c-WBV group (Table 2). Low albumin was significantly associated with high c-WBV, indicating its role as a negative prognostic factor. The total protein value significantly differed in the high c-WBV group (p<0.001), while hematocrit did not show a significant difference despite its general prognostic value (Table 2). This suggests that hyperproteinemia, often due to elevated immunoglobulin levels, contributes to increased blood viscosity and associated risks. Lower albumin levels in the high-WBV group further link hypoalbuminemia to poor prognosis in MM patients. High c-WBV (≥17.14) values also correlated with higher ISS stage 3 prevalence, likely related to low albumin. No significant correlation was found between c-WBV and β2-MG, calcium, LDH, creatinine, and platelet values (Table 2). Significant relationships were identified between ISS, calcium, LDH, β2-MG, platelet, hematocrit, protein, and albumin values and survival (Table 1) (p<0.05). Protein value alone predominantly determined the c-WBV value in the evaluation of the relationship with other prognostic markers. Apart from the association with mortality and OS, although not statistically significant, it was observed that the group with high c-WBV (≥17.14) values demonstrated higher prevalence, particularly in ISS stage 3, which appears to be related to the correlation with low albumin. A noteworthy observation is the absence of a significant correlation between β2-MG, calcium, LDH, creatinine, and platelet values, and c-WBV (Table 2). In the analysis of general characteristic features, a significant relationship was identified between ISS, calcium, LDH, β2-MG, PLT, Htc, protein, and albumin values and survival (Table 1) (p<0.05). Our study revealed that the protein value alone played a predominant role in determining the c-WBV value. There is no consensus on the proper diagnosis and standard interpretation of reticulin staining density (RLD) in MM, and myelofibrosis should not be equated with fibrosis. A lower RLD value in MM may yield a more precise assessment. RLD, reflecting the bone marrow microenvironment, has been linked to decreased OS and mortality in MM, a disease with established survival relationships. It also correlates with various clinical pathological factors.21 This study found a significant inverse relationship between bone marrow RLD and survival, with higher reticular fiber grades (grades 2 and 3) showing substantially lower two-year survival rates of 43.6% and 23.3%, respectively, compared to 71.7% for grade 1 and no mortality for grade 0. These results suggest that BMF, linked to increased production of fibrogenic cytokines like TGF-β and IL-6 due to tumor burden, is crucial for MM prognosis. The correlation between higher RLD and poor survival underscores the importance of bone marrow microenvironment changes in disease progression. High levels of M protein, related to disease burden, may increase cytokine production associated with fibrosis.22 A statistically significant difference was found between the RLD-3 group and the high c-WBV group (Table 2). Incorporating c-WBV and RLD into routine clinical assessments could improve risk stratification and guide therapeutic decisions. Addressing hyperviscosity and managing BMF may enhance patient outcomes, warranting future prospective studies to validate these findings and explore targeted interventions for patients with high c-WBV and advanced BMF.
Limitations
Our study was a retrospective, single-center investigation with a limited sample size. A larger, multicenter, prospective study could provide more reliable results. Some patients lacked cytogenetic examination data, but exploring the relationship between cytogenetic results and c-WBV remains feasible and potentially valuable. The relationship between PFS and c-WBV could not be established due to the unavailability of PFS results. Additionally, the inability to determine patients’ causes of death required calculating mortality related to thrombotic events.
Conclusion
The study underscores the pivotal influence of clinical and laboratory markers on MM prognosis and survival, incorporating advanced staging systems like the R-ISS. The retrospective analysis highlights c-WBV as a potential prognostic marker associated with both thrombosis risk and survival outcomes, filling a gap in the literature where no prior studies have examined the relationship between c-WBV and MM prognosis. This study reveals that elevated c-WBV values correlate with decreased survival and increased prognosis in MM beyond their effectiveness in thrombosis and vascular events. Data analyses showed no significant differences among MM subtypes and ISS, with primary determinants being low albumin and increased total protein levels. The findings suggest increased globulin production, inflammation, and the negative impact of elevated cytokines on albumin production as potential explanations. The simplicity of calculating these parameters suggests their broader application, advocating for their automatic inclusion in biochemistry results to enhance accessibility. Early anticoagulant initiation in patients with elevated blood viscosity might positively impact life expectancy and mortality. Additionally, bone marrow RLD, indicative of BMF, was linked to shorter survival in patients with higher fibrosis grades, adding depth to the MM prognostic evaluation. The study suggests that RLD, c-WBV, and key markers like protein levels should be integrated into comprehensive patient prognosis assessments. The research advocates incorporating parameters like c-WBV and RLD into routine clinical evaluations to refine prognostic accuracy and tailor patient management, especially for those at higher risk of adverse outcomes. Future prospective studies are necessary to validate these findings and explore their role in guiding therapeutic decisions. The aim is to enhance hemorheological evaluation by addressing current limitations and providing more comprehensive data with a larger sample size, considering factors like cytogenetic abnormalities.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or compareable ethical standards.
Informed Consent
Written informed consent was obtained from all participants included in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
BMF: Bone marrow fibrosis
CRP: C-reactive protein
c-WBV: Calculated whole blood viscosity
HCT: Hematocrit
HGB: Hemoglobin
ISS: International Staging System
LDH: Lactate dehydrogenase
MM: Multiple myeloma
OS: Overall survival
PLT: Platelet count
R-ISS: Revised International Staging System
RLD: Reticulin staining density
ROC: Receiver operating characteristic
TP: Total protein
WBV: Whole blood viscosity
β2MG: Beta-2 microglobulin
References
-
Landgren O, Rajkumar SV. New developments in diagnosis, prognosis, and assessment of response in multiple myeloma. Clin Cancer Res. 2016;22(22):5428-5433. doi:10.1158/1078-0432.ccr-16-0866
-
Veljkovikj I, Ilbawi AM, Roitberg F, et al. Evolution of the joint International Atomic Energy Agency, International Agency for Research on Cancer, and WHO cancer control assessments: imPACT reviews. Lancet Oncol. 2022;23(10):1261-1269.
-
Greipp PR, San Miguel J, Durie BG, et al. International staging system for multiple myeloma. J Clin Oncol. 2005;23(15):3412-3420. doi:10.1200/jco.2005.04.242
-
Fonseca R, Bergsagel PL, Drach J, et al. International Myeloma Working Group molecular classification of multiple myeloma: spotlight review. Leukemia. 2009;23(12):2210-2221. doi:10.1038/leu.2009.174
-
D’Agostino M, Cairns DA, Lahuerta JJ, et al. Second revision of the International Staging System for overall survival in multiple myeloma: a European Myeloma Network report within the HARMONY project. J Clin Oncol. 2022;40(36):364-373. doi:10.1200/jco.22.02228
-
Caimi G, Carlisi M, Montana M, et al. Erythrocyte deformability and hemorheological profile in multiple myeloma. Clin Hemorheol Microcirc. 2018;68(1):37-45. doi:10.3233/ch-170267
-
Carlisi M, Mancuso S, Lo Presti R, Siragusa S, Caimi G. Comparison between WBV measured and calculated in subjects with monoclonal gammopathy of undetermined significance and in patients with multiple myeloma: re-evaluation of our survey. Clin Hemorheol Microcirc. 2021;79(3):273-280. doi:10.3233/ch-211198
-
Carlisi M, Lo Presti R, Mancuso S, Siragusa S, Caimi G. Thrombotic risk and calculated whole blood viscosity in a cohort of patients with new diagnosis of multiple myeloma. Clin Appl Thromb Hemost. 2024;30:10760296231222477. doi:10.1177/10760296231222477
-
Dees C, Chakraborty D, Distler JHW. Cellular and molecular mechanisms in fibrosis. Exp Dermatol. 2021;30(1):24-31. doi:10.1111/exd.14193
-
Ziogas DC, Dimopoulos MA, Kastritis E. Prognostic factors for multiple myeloma in the era of novel therapies. Expert Rev Hematol. 2018;11(11):863-879. doi:10.1080/17474086.2018.1537776
-
Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised International Staging System for multiple myeloma: a report from International Myeloma Working Group. J Clin Oncol. 2015;33(26):2863-2869. doi:10.1200/jco.2015.61.2267
-
Chen YK, Han SM, Yang Y, et al. Early mortality in multiple myeloma: experiences from a single institution. Hematology. 2016;21(7):393-398. doi:10.1080/10245332.2015.1101969
-
Zangari M, Fink L, Zhan F, Tricot G. Low venous thromboembolic risk with bortezomib in multiple myeloma and potential protective effect with thalidomide/lenalidomide-based therapy: review of data from phase 3 trials and studies of novel combination regimens. Clin Lymphoma Myeloma Leuk. 2011;11(2):228-234. doi:10.1016/j.clml.2011.03.006
-
Kwaan HC. Role of plasma proteins in whole blood viscosity: a brief clinical review. Clin Hemorheol Microcirc. 2010;44(3):167-176. doi:10.3233/ch-2010-1271
-
Peters SA, Woodward M, Rumley A, Tunstall-Pedoe HD, Lowe GD. Plasma and blood viscosity in the prediction of cardiovascular disease and mortality in the Scottish Heart Health Extended Cohort Study. Eur J Prev Cardiol. 2017;24(2):161-167. doi:10.1177/2047487316672004
-
Alexy T, Detterich J, Connes P, et al. Physical properties of blood and their relationship to clinical conditions. Front Physiol. 2022;13:906768. doi:10.3389/fphys.2022.906768
-
Ay C, Pabinger I, Cohen AT. Cancer-associated venous thromboembolism: burden, mechanisms, and management. Thromb Haemost. 2017;117(2):219-230. doi:10.1160/th16-08-0615
-
Choi D, Waksman O, Shaik A, et al. Association of blood viscosity with mortality among patients hospitalized with COVID-19. J Am Coll Cardiol. 2022;80(4):316-328. doi:10.1016/j.jacc.2022.04.060
-
Truong AD, Auld SC, Barker NA, et al. Therapeutic plasma exchange for COVID-19-associated hyperviscosity. Transfusion. 2021;61(4):1024-1031. doi:10.1111/trf.16218
-
Maier CL, Truong AD, Auld SC, Polly DM, Tanksley CL, Duncan A. COVID-19-associated hyperviscosity: a link between inflammation and thrombophilia? Lancet. 2020;395(10239):1758-1759. doi:10.1016/s0140-6736(20)31209-5
-
Hu X, Dai X, Guo X, et al. Bone marrow fibrosis in newly diagnosed multiple myeloma and its correlation with clinicopathological factors. Diagn Pathol. 2024;19(1):99. doi:10.1186/s13000-024-01516-y
-
Babarović E, Valković T, Štifter S, et al. Assessment of bone marrow fibrosis and angiogenesis in monitoring patients with multiple myeloma. Am J Clin Pathol. 2012;137(6):870-878. doi:10.1309/ajcpt5y2jriuucub
Figures
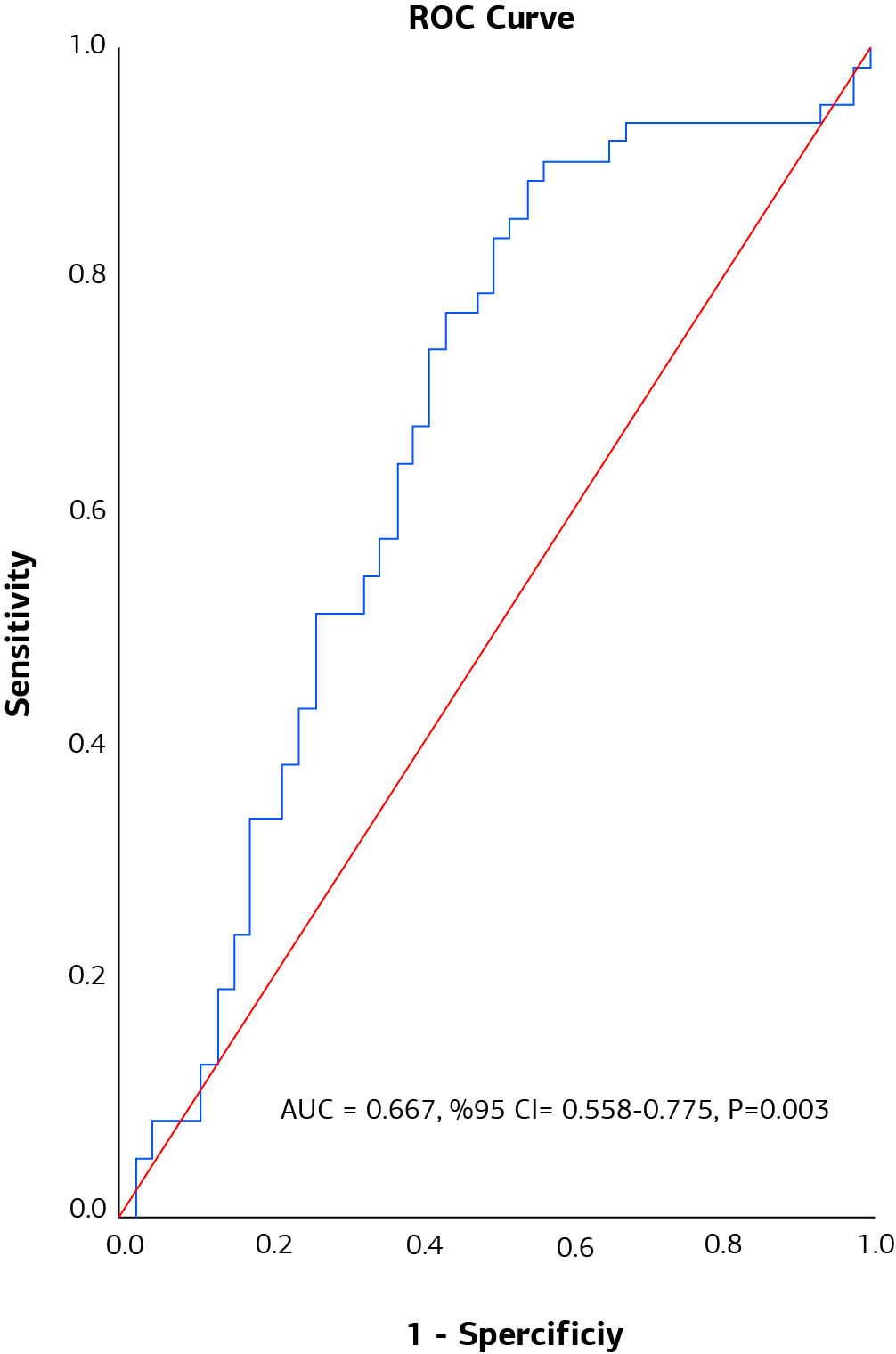
Figure 1. ROC curve for the predictive power of whole blood viscosity on mortality

Figure 2. Comparison of WBV groups in terms of survival

Figure 3. Comparison of survival among RLD groups
Tables
Table 1. Comparison of patients’ general characteristics according to their final status
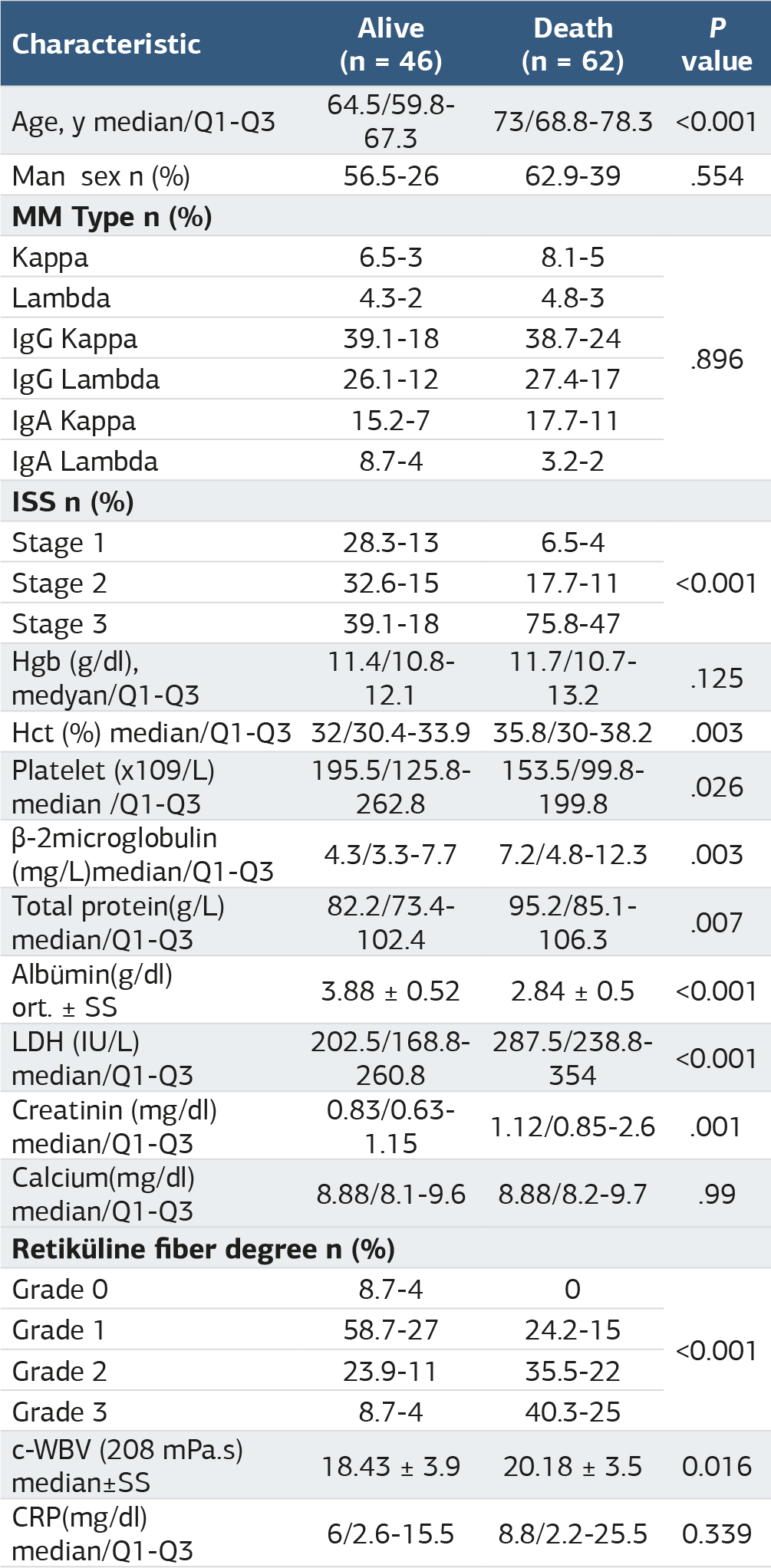
Table 2. Comparison of low and high viscosity groups in terms of general characteristics

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mustafa Duran, Nermin Keni Begendi, Çiğdem Özdemir, Sinan Kazan, Yiğit Senol. The prognostic role of whole blood viscosity and bone marrow fibrosis inpredicting survival outcomes in new diagnosis multiple myeloma patients. Ann Clin Anal Med 2025;16(4):309-314. doi:10.4328/ACAM.22452
- Received:
- October 12, 2024
- Accepted:
- November 18, 2024
- Published Online:
- November 23, 2024
- Printed:
- April 1, 2025