
The seasonal variation in pancreatitis attacks among emergency department admissions
Seasonal variation in pancreatitis
Authors
Abstract
AimSeasonal variations have previously been examined in numerous gastrointestinal diseases, particularly in etiological factors. This study aimed to investigate the seasonal variation of acute pancreatitis (AP) cases commonly seen in emergency departments (ED).
MethodsThis study was retrospective, cross-sectional, and descriptive. Data were collected from patients diagnosed with AP who presented to the ED. Demographic information (age and gender), laboratory data (complete blood count, liver function tests, amylase and lipase levels), and the admission season were recorded. The etiological factors triggering AP were categorized into biliary and non-biliary groups.
ResultsA total of 203 patients were included in the study. Of these, 91 (44.8%) were male and 112 (55.2%) were female. The mean age of the patients was 60.37 ± 18.15 years. The number of AP cases admitted to the ED was higher in the spring 62 (30.5%) and summer 67 (33%) compared to autumn 39 (19.2%) and winter 35 (17.2%). When patients were grouped by season, no statistically significant differences were found regarding age or gender. A comparison of laboratory values showed a statistically significant difference in aspartate aminotransferase (AST) levels between seasons (highest in autumn, lowest in summer). Analysis of AP etiology revealed that 146 patients (71.9%) had biliary pancreatitis, while 57 patients (28.1%) had non-biliary pancreatitis. There was no significant difference in the etiology of AP (biliary vs. non-biliary) between different seasons.
ConclusionThe incidence of AP is higher in the spring and summer months, indicating that ED physicians should be more vigilant during these seasons. Furthermore, elevated AST levels in autumn may suggest a worse prognosis for AP during this period.
Keywords
Introduction
Acute pancreatitis (AP) is defined as a reversible inflammation of the pancreatic parenchyma, with severity ranging from mild edematous pancreatitis to severe necrotizing pancreatitis. The etiology of AP is diverse, with more than half of the cases caused by gallstones, while alcohol consumption, hyperlipidemia, abdominal surgery, and various medications also contribute. Many authors propose a common pathway in the pathogenesis of AP, where inappropriate intracellular proteolysis of digestive enzymes leads to auto-digestion and parenchymal inflammation.1,2 Due to its diverse etiology and variability, the incidence of AP is known to differ between countries and even regions. A continuous increase in the incidence of AP has been reported over time, particularly in Western countries.3 Despite the publication of various management strategies in recent years, the overall mortality rate of AP remains high, ranging from 1.5% to 17%, primarily due to systemic inflammatory response syndrome (SIRS) and organ failure.4,5
Since the most common symptom of AP is abdominal pain, patients often present first to the ED. Identifying AP cases and initiating treatment promptly in the ED is crucial, given the potential for fatal complications.
Seasonal variations have previously been studied in various gastrointestinal diseases, particularly about etiological factors.6 Although demographic and etiological studies have been conducted on AP, which is common in all age groups due to its diverse etiology and severe complications, studies examining the impact of climate and seasonal differences on AP rates are limited. This study aimed to investigate the seasonal variation of AP cases frequently seen in emergency departments.
Materials and Methods
This retrospective, cross-sectional, descriptive investigation was undertaken from June 1, 2021, to May 31, 2024. Data were retrieved by scanning patient digital records via the hospital information management system.
The study’s inclusion criteria were established as presenting to the emergency department during the designated date range, being above 18 years of age, and possessing a diagnosis of Acute Pancreatitis. Cases of acute pancreatitis were identified with ICD-10 codes, with diagnoses corroborated through clinical observations, physical examinations, laboratory data, and imaging studies. The study’s exclusion criteria encompassed pregnant women, individuals under 18 years of age, and cases of chronic pancreatitis, all of which were eliminated from the study.
Demographic information (age and gender), laboratory data (complete blood count, liver function tests, amylase and lipase levels), and the admission season were recorded. Etiological factors triggering AP were classified into biliary and non-biliary categories.
Ethical ApprovalThis study was approved by the Ethics Committee of Konya City Hospital (Date: 05.09.2024, Decision No:10-74).
Statistical AnalysisThe data collected from the study were imported into a computer system, and the Statistical Package for the Social Sciences (SPSS) version 18.0 for Windows (SPSS Inc., Chicago, IL, US) was utilized for the statistical analysis of the results. Descriptive statistical techniques (count(N), percentage, Mean ± Standard Deviation) were employed in the data evaluation. The data’s normality was assessed utilizing the Kolmogorov-Smirnov test. The chi-square (χ2) test was employed for categorical data comparison, inter-group comparisons were performed using ANOVA and Welch tests, and the Levene test was utilized to assess the homogeneity assumption.
The threshold for statistical significance was established at p<0.05.
Reporting GuidelinesThe study was reported in accordance with STROBE.
Results
A total of 203 patients were included in the study. Of these, 91 (44.8%) were male and 112 (55.2%) were female (Figure 1). The mean age of the patients was 60.37 ± 18.15 years (min=22, max=98). The number of AP cases presenting to the ED was higher in spring 62 (30.5%) and summer 67 (33%) compared to autumn 39 (19.2%) and winter 35 (17.2%). The demographic characteristics of the patients by season of admission are summarized in Table 1.
No statistically significant differences were found between the groups regarding age or gender when patients were grouped by season. The laboratory findings of patients by season of admission are summarized in Table 2.
A comparison of laboratory values showed no statistically significant differences in white blood cell (WBC) count, alanine aminotransferase (ALT), gamma-glutamyl transferase (GGT), amylase, and lipase levels between seasons. However, a statistically significant difference in aspartate aminotransferase (AST) levels was observed between seasons (highest in autumn, lowest in summer).
Analysis of AP etiology revealed that 146 patients (71.9%) had biliary pancreatitis, while 57 patients (28.1%) had non-biliary pancreatitis. The relationship between AP etiology and the season of admission is summarized in Table 3. These results indicate no statistically significant relationship between the season and the presence of gallstones. In other words, there is no significant difference in the etiology of AP (biliary vs. non-biliary) between different seasons.
Discussion
In this study, we investigated whether there is a seasonal variation in the number of patients admitted to the ED with AP and found that the number of AP admissions was higher in the spring and summer than in autumn and winter. There were no gender or age differences among patients presenting with AP across different seasons. However, AST levels were significantly higher in autumn and lower in summer. No statistically significant association was found between season and the etiology of AP (biliary vs. non-biliary).
The literature on seasonal variations in AP is limited. In a retrospective study conducted in Sweden from 2003 to 2012 with 1457 AP patients (83% non-alcoholic, 17% alcoholic), no significant seasonal differences in AP incidence were observed in.7 Similarly, a retrospective cohort study conducted in South Korea among 9023 AP patients reported no clear seasonal variations.6 A retrospective cohort study in Chicago with 460 patients also found no effect of seasons on AP etiology.8 However, other studies support our findings. A retrospective study in Italy involving 1883 consecutive cases of AP identified a significant peak in AP incidence during the summer. Additionally, older individuals had an increased incidence of AP in autumn and summer compared to other seasons.9 Another Italian study involving 549 cases of AP reported a significantly higher frequency of cases in the spring.10
In our study, we did not observe a significant relationship between AP etiology and season. However, a recent study involving 3597 AP cases found that idiopathic and biliary cases were significantly more common from May to July, with most drug-induced AP cases identified in the winter and a significant peak in alcohol-induced pancreatitis during summer and fall.11 Li et al. evaluated the short-term effect of temperature on the risk of AP in 2822 patients in China, reporting that higher daily average temperatures increased the occurrence of nonbiliary pancreatitis but not biliary pancreatitis.12
From a pathophysiological perspective, seasonal biological changes that may influence the onset of AP, such as the secretion of pancreatic enzymes or bile acids, are not yet well understood. It can be hypothesized that dehydration may trigger changes in bile secretion, leading to bile sludge formation and eventual stone deposition.13 Additionally, summer is typically associated with increased alcohol consumption, which could be a significant factor in the incidence of AP. However, no seasonal differences in AP etiology were found in this study. We identified a statistically significant difference in AST levels among seasons, with the highest levels observed in autumn and the lowest in summer. Previous studies have reported that serum AST levels are positively correlated with the severity of pancreatitis.14,15 AST is also part of the Ranson criteria used at admission, which is an important prognostic factor in AP.16,17 Therefore, elevated AST levels in autumn may indicate a worse prognosis for AP during this season. Data on seasonal differences in AP mortality rates are limited. Gallerani et al. reported that the percentage of fatal events was significantly higher in December through February. However, larger studies on AP outcomes across different seasons are needed.
Limitations
This was a retrospective, single-center study with a relatively short time frame and a limited number of AP cases admitted to the ED during this period. Additionally, since treatment and follow-up were not conducted in the ED, we did not evaluate patient outcomes or mortality. Another limitation of our study is the inability to identify etiological factors beyond gallstones in cases of acute pancreatitis due to the retrospective nature of the study.
Conclusion
In this study, we found that the incidence of AP was higher during the spring and summer seasons. Additionally, elevated AST levels in autumn may indicate a worse prognosis for AP during this season. Further research is needed to better understand the seasonal variations in AP and their potential impact on clinical outcomes. Our results suggest that ED physicians should be more vigilant about AP during the spring and summer months.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
ALT: Alanine aminotransferase
AP: Acute pancreatitis
AST: Aspartate aminotransferase
CBC: Complete blood count
ED: Emergency department
GGT: Gamma-glutamyl transferase
ICD: International classification of diseases
SD: Standard deviation
SIRS: Systemic inflammatory response syndrome
WBC: White blood cell
References
-
Lee PJ, Papachristou GI. New insights into acute pancreatitis. Nat Rev Gastroenterol Hepatol. 2019;16(8):479-496. doi:10.1038/s41575-019-0158-2
-
Li CL, Jiang M, Pan CQ, Li J, Xu LG. The global, regional, and national burden of acute pancreatitis in 204 countries and territories, 1990-2019. BMC Gastroenterol. 2021;21(1):332. doi:10.1186/s12876-021-01906-2
-
Iannuzzi JP, King JA, Leong JH, et al. Global incidence of acute pancreatitis is increasing over time: a systematic review and meta-analysis. Gastroenterology. 2022;162(1):122-134. doi:10.1053/j.gastro.2021.09.043
-
Mederos MA, Reber HA, Girgis MD. Acute pancreatitis: a review. JAMA. 2021;325(4):382-390. doi:10.1001/jama.2020.20317
-
Greenberg JA, Hsu J, Bawazeer M, et al. Clinical practice guideline: management of acute pancreatitis. Can J Surg. 2016;59(2):128-140. doi:10.1503/cjs.015015
-
Yoon JY, Cha JM, Kim HI, Kwak MS. Seasonal variation of peptic ulcer disease, peptic ulcer bleeding, and acute pancreatitis: a nationwide population-based study using a common data model. Medicine (Baltimore). 2021;100(21). doi:10.1097/md.0000000000025820
-
Bertilsson S, Håkansson A, Kalaitzakis E. Acute pancreatitis: impact of alcohol consumption and seasonal factors. Alcohol Alcohol. 2017;52(3):383-389. doi:10.1093/alcalc/agx005
-
Jaiswal P, Wang Y, Elkhouly M, Simons-Linares RC. Is there a weather seasonal effect on acute pancreatitis etiology and outcomes? Am J Gastroenterol. 2017;112. doi:10.14309/00000434-201710001-00077
-
Guarino M, Bologna A, Ursini F, et al. Chronobiology of acute pancreatitis in a single Italian centre. Eur Rev Med Pharmacol Sci. 2020;24(4):1988-1994. doi:10.26355/eurrev_202002_20376
-
Gallerani M, Boari B, Salmi R, Manfredini R. Seasonal variation in the onset of acute pancreatitis. World J Gastroenterol. 2004;10(22):3328-3331. doi:10.3748/wjg.v10.i22.3328
-
Sirtl S, Hohmann E, Beyer G, Hamm J, Neesse A, Ammer-Herrmenau C. The four seasons of pancreatitis: etiology of acute pancreatitis during the course of the year. Z Gastroenterol. 2024;62(8):1207-1210. doi:10.1055/a-2293-7813
-
Li B, Huang W, Chen P, Chen J, Biviano I, Wang Z. Effect of ambient temperature on daily hospital admissions for acute pancreatitis in Nanchang, China: a time-series analysis. Int J Environ Health Res. 2022;32(10):2260-2270. doi:10.1080/09603123.2021.1952166
-
Park BK, Chung JB, Lee JH, et al. Role of oxygen free radicals in patients with acute pancreatitis. World J Gastroenterol. 2003;9(10):2266-2269. doi:10.3748/wjg.v9.i10.2266
-
Güngör B, Çağlayan K, Polat C, Seren D, Erzurumlu K, Malazgirt Z. The predictivity of serum biochemical markers in acute biliary pancreatitis. ISRN Gastroenterol. 2011;2011:279607. doi:10.5402/2011/279607
-
Liu W, Du JJ, Li ZH, Zhang XY, Zuo HD. Liver injury associated with acute pancreatitis: the current status of clinical evaluation and involved mechanisms. World J Clin Cases. 2021;9(34):10418-10429. doi:10.12998/wjcc.v9.i34.10418
-
Metri A, Bush N, Singh VK. Predicting the severity of acute pancreatitis: current approaches and future directions. Surg Open Sci. 2024;19:109-117. doi:10.1016/j.sopen.2024.03.012
-
Şenkal N, Karahan L, Bardak AE, et al. Erratum to: assessment of the Ranson score in acute pancreatitis: its value in an emergency setting upon admission. J Ist Faculty Med. 2023;87(1):101. doi:10.26650/iuitfd.1272976
Figures

Figure 1. Seasonal gender distribution
Tables
Table 1. Demographic features of the patients regarding admission season

1. The data has been represented as N, %, Mean±SD 2. p<0.05 was considered statistically significant. The Chi-squared test (χ²) was employed in statistical analysis
Table 2. Laboratory data of the patients regarding admission season
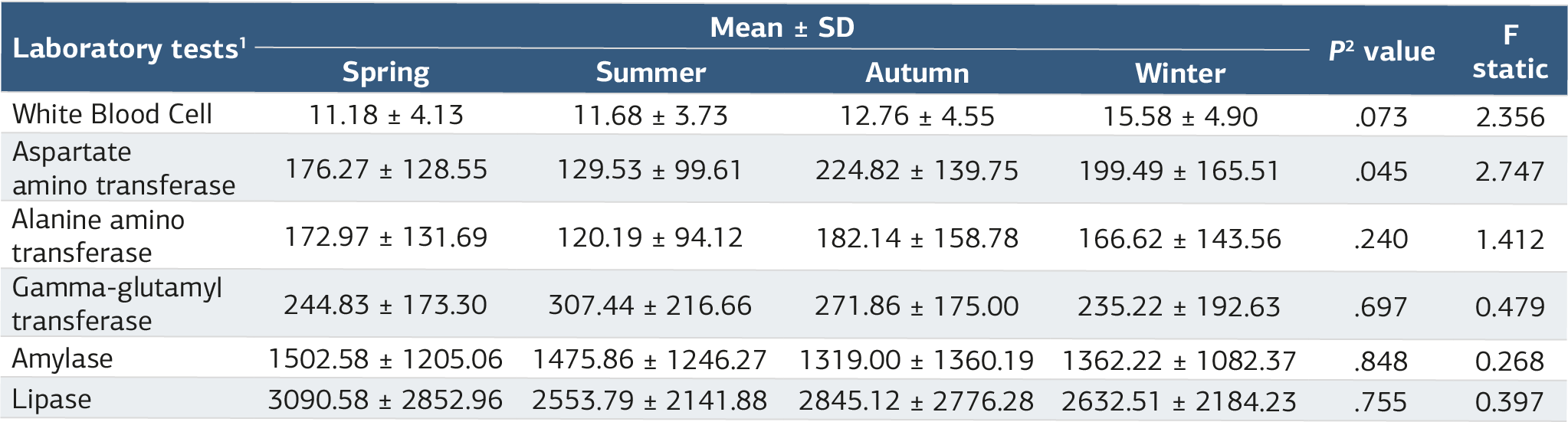
1. The data has been represented as Mean±SD. 2. p<0.05 was considered statistically significant. Levene's test, Analysis of variance, ANOVA test (F), and Welch's ANOVA test were employed in statistical analysis
Table 3. Etiology of AP regarding admission season

1. The data has been represented as N, % 2. p<0.05 was considered statistically significant. The Chi-squared (Likelihood Ratio) test (χ²) was employed in statistical analysis
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Demet Acar, Fatih Cemal Tekin, Emin Fatih Vişneci, Mehmet Gül. The seasonal variation in pancreatitis attacks among emergency department admissions . Ann Clin Anal Med 2025;16(1):15-34. doi:10.4328/ACAM.22457
- Received:
- October 15, 2024
- Accepted:
- November 18, 2024
- Published Online:
- November 29, 2024
- Printed:
- January 1, 2025