
Evaluation of patients with vertebral osteomyelitis diagnosis: ten years of experience
Vertebral osteomyelitis: 10-year experience
Authors
Abstract
AimAn infection of the vertebrae and intervertebral disc is known as vertebral osteomyelitis (VO). Examining the demographics, comorbidity variables, etiologies, significant laboratory results, and diagnostic and therapeutic techniques of VO cases that were monitored and treated over a ten-year period was the goal of this study.
MethodsDemographic information, clinical symptoms, chronic illnesses, history of vertebral operations, involved vertebral levels, diagnostic methods, leukocyte count (WBC), erythrocyte sedimentation rate (ESR), serum C-reactive protein level (CRP), amount of hematocrit (HTC), results of microbiological cultures, and agent-specific serology results of the cases followed up with VO diagnosis between January 1, 2014 and January 1, 2024 were collected and analyzed from patient files.
ResultsThe mean age of the 125 cases included in the study was 57.5±13.8 years, and the M/F ratio was 1/1.7. The presenting complaints were pain (100%), neurological symptoms (60%), fever (15.2%), fatigue (12%), night sweats (4.8%), and weight loss (0.8%). The cases were diagnosed by imaging methods (92%) or microbiological methods (8%). Comorbidities observed included diabetes (20.8%), renal disease (10.4%), rheumatological disease (3.2%), malignancy (1.6%), history of spinal surgery (31.2%), trauma (13.6%), urinary tract infection (7.2%), nonspecific infection (6.4%), and a history of cerebrovascular events (0.8%). The average response time for ESR and CRP related to pain was found to be around the third week.
ConclusionEvaluating pain symptoms, planning imaging methods, confirming diagnosis through biopsy, and initiating pathogen-targeted treatment will be significant steps in enhancing the success of VO treatment. ESR and CRP serve as early indicators for follow-up.
Keywords
Introduction
Vertebral osteomyelitis (VO) is a pyogenic, granulomatous or parasitic infection of the vertebrae and intervertebral disc. Although it usually develops via hematogenous route, it may also occur via neighborhood or direct inoculation.1 In the literature, risk factors for the development of VO include diabetes mellitus (DM), immunosuppression, chronic heart disease, liver cirrhosis, intravenous drug use, Human Immunodeficiency Virus (HIV) infection, history of spinal surgery, presence of a foreign body in the vertebra, chronic kidney disease, presence of intravenous catheter, and history of bacteremia.2 There has been an increase in the incidence of VO over the years due to the prolongation of life expectancy in society, the increase in the incidence of chronic diseases with advancing age, and the widespread use of spinal surgical interventions and other invasive interventions that may trigger bacteremia. This increase is especially evident in the elderly age group who need healthcare services more frequently and more frequently.3,4 Pain is the most common complaint that brings patients to the physician. Fever is a relatively less common symptom. Diagnosis is usually made by blood cultures, biopsy cultures and imaging methods in the presence of clinical findings, especially pain.5,6 In our country, brucellosis-related VO is still common in patients with a history of unpasteurized milk and dairy product consumption and animal husbandry. In these patients, the diagnosis is made with the help of detailed anamnesis and serologic tests.7 In addition to all risk factors, an increase in the risk of VO is observed especially in the elderly population.8 With the increase in the elderly population, easier access to healthcare services and widespread use of invasive medical interventions, VO has become an important infectious disease that infectious diseases specialists follow up with long-term antibiotic treatment. The aim of this study was to evaluate the demographic characteristics, comorbidity factors, etiologies, important laboratory findings, and diagnostic and therapeutic modalities of VO cases followed and treated in the infectious diseases unit of our hospital.
Materials and Methods
The study was designed as retrospective and observational. The data of all cases followed up with the diagnosis of VO in the infectious diseases clinic and outpatient clinic of our hospital in the ten-year period between January 1, 2014 and January 1, 2024 were obtained through the hospital information system. Patients who were diagnosed with VO both clinically and by imaging methods (magnetic resonance imaging (MRI) or computed tomography (CT)) and treated were included in the study. Patients with missing data were excluded. Demographic data, clinical symptoms, chronic diseases, vertebral operation history, diagnostic methods, leukocyte count (WBC), erythrocyte sedimentation rate (ESR), serum C-reactive protein level (CRP), hematocrit (HTC), microbiological culture results and agent-specific serology results were recorded. Data on the treatments administered to the patients, treatment durations and clinical response status of the patients were obtained from the patient files.
Ethical ApprovalThis study was approved by the Ethics Committee of İzmir Buca Seyfi Demirsoy Training and Research Hospital (Date: 24.04.2024, Decision No: 2024/270).
Statistical AnalysisDescriptive statistics of the study were performed using the R program (Version 2024.04.1 + 748, Copyright (C) 2024 by Posit Software, PBC). The conformity of continuous variables to normal distribution was evaluated by Shapiro-Wilk test. Data conforming to normal distribution were expressed as mean and standard deviation, and data not conforming to normal distribution were expressed as median, Q1 and Q3. Descriptive statistics were performed using “dplyr” and “psych” packages in R.
Reporting GuidelinesThis study was reported in accordance with the STROBE guideline.
Results
A total of 125 patients were included in the study. The mean age was 57.5 ± 13.8 years, 36.8% (n = 46) were male and 63.2% (n = 79) were female. When the presenting complaints were evaluated, pain symptoms were observed in all cases. Neurologic symptoms were present in 60%, fever in 15.2%, fatigue in 12%, night sweats in 4.8%, and weight loss in 0.8%. Imaging methods were used in 92% of the cases and microbiologic methods in 8%. The most common finding on imaging methods was an abscess (19.2% of cases) and the most common location was the paravertebral region (54%, n = 13/24). Mortality was not observed in any of the cases. Demographic and clinical characteristics of the cases are shown in Table 1.
When the causes were evaluated, it was seen that brucellosis infection was the cause of VO in 10 cases (8%). In only 8 cases (6.4%), culture samples were taken from the site of involvement for diagnostic purposes. No growth was detected in 6 of these cases, 1 had methicillin-sensitive Staphylococcus aureus (MSSA) and 1 had extended spectrum betalactamase (ESBL) positive Klebsiella pneumoniae.
The cases were analyzed in terms of risk factors for the development of VO. Diabetes was present in 20.8%, renal disease in 10.4%, rheumatologic disease in 3.2%, and malignancy in 1.6%. In addition, 31.2% had a history of spinal surgery, 13.6% trauma, 7.2% urinary tract infection (UTI), 6.4% nonspecific infection, and 0.8% cerebrovascular accident (CVA) (Table 2).
When the laboratory results of the patients were analyzed, the median leukocyte count was 7800 103/uL, the median CRP was 21 mg/L, the median ESR was 51 mm/h and the median HTC was 35.5% (Table 3).
The mean duration of initial parenteral treatment was 3 weeks, the mean duration of oral maintenance treatment was 6 weeks, and the mean duration of improvement of laboratory results was 3 weeks. The mean duration of pain response with treatment was found to be 21 days.
Discussion
Vertebral osteomyelitis is a disease with an increasing incidence, affecting especially the population over the age of 50, requiring a multidisciplinary approach to diagnosis and treatment.9,10 In our study, it was observed that the majority of the patients diagnosed with VO were females and all of them had complaints of low back pain. Low back pain is reported to be the most common symptom in the literature.5,6 In our study, the second most common symptom was neurologic disorder, the majority of which was difficulty in walking. Fever, which may be more indicative of the diagnosis of infection, was found in 15% of the patients. In a study conducted in Turkey between 2000 and 2007 by Mete B. et al. in which 100 cases were included, it was reported that fever was found in 50% of the cases.5 In our study, 10 of 125 cases were diagnosed with brucellosis, whereas in the study by Mete B. et al. 24 of 100 cases were diagnosed with brucellosis and 32 with tuberculosis.5 Although we are in a country where brucellosis and tuberculosis diseases are endemic, there were no patients diagnosed with tuberculosis in our cases and our brucellosis diagnosis was low. In the study conducted by Elbahr et al. between 2009 and 2019, in which 100 cases were included, 26 of the VO cases were diagnosed with tuberculosis and 15 with brucellosis. It was found that fever symptoms were most common in VO cases diagnosed with brucellosis, with a total rate of 33%.11 In another study conducted in Turkey, it was reported that the presence of fever was statistically significant in VO cases diagnosed with brucellosis.12
When the studies in the literature are evaluated, it is noteworthy that Staphylococcus aureus and Mycobacterium tuberculosis are the most frequently detected agents in cases of VO.11,13 The reason for the low number of patients from whom the causative agent could be isolated in our study was the low rate of vertebral biopsy.
When the cases were analyzed in terms of comorbid conditions, spinal surgery, trauma, DM, renal disease, urinary tract infection, nonspecific infection and rheumatologic disease were found most frequently in our study. There were no patients with a history of intravenous drug use or living with HIV. Similarly, the most common predisposing conditions observed in studies conducted in Turkey were reported to be spinal surgery intervention and DM.11 In a study conducted in the United States of America, the most common comorbid conditions were hypertension and DM, and the rates of HIV infection and substance abuse were higher.14
Guidelines recommend imaging-guided biopsy cultures for the diagnosis of VO.15 However, this is not possible in practice. Magnetic resonance imaging has been reported to have high sensitivity and specificity in many studies and has been accepted as the gold standard imaging for diagnosis.16,17 MRI results of all patients diagnosed with VO included in our study were compatible with VO.
When we examined the laboratory tests that may help the diagnosis in our study, we observed that the median leukocyte value was normal. CRP median value was 21 mg/L, ESR median value was 51 mm/h and HTC median value was 35.5%. It was observed that leukocyte and HTC values would not help the diagnosis. In previous studies, it has been reported that CRP and ESR values are high during diagnosis and prevent delay in diagnosis.11,18,19 In the guidelines, it is stated that these parameters can be used for monitoring the response to treatment and that it would be appropriate to check the values at four-week intervals.15 Yoon SH et al. reported that elevated CRP and ESR values in the fourth week of VO follow-up were associated with treatment failure.20 In our study, it was observed that treatment response was detectable at the end of 3 weeks based on a decrease of more than 25% in ESR and CRP values. Based on this result, we think that CRP and ESR can be checked earlier in follow-up. Thus, when treatment failure is suspected, earlier follow-up imaging or treatment change may be considered.
Monitoring of pain is also very important in the follow-up of treatment response in patients. There is no single clear criterion for the follow-up of treatment failure in the guidelines. For this reason, clinicians follow up with clinical, laboratory and imaging methods.15 In our study, it was observed that the average duration of pain relief was 21 days. It was observed that the laboratory response characterized by regression in CRP and ESR values and the pain response occurred on similar days. In a meta-analysis, it was reported that treatment failure may occur when pain response is not obtained in the fourth week.21
There is no clear duration for the duration of treatment of pyogenic VO. The Infectious Diseases Society of America (IDSA) guideline suggests that 6 weeks of treatment is sufficient.15 Recommendations for the duration of treatment vary from 6 weeks to 3 months, and there is no clear recommendation in the guidelines for the duration of intravenous treatment.15,22,23 In our study, it was observed that the mean duration of parenteral treatment was 3 weeks and the mean duration of oral maintenance treatment was 6 weeks.
Limitations
There were some limitations of our study, which we think were mainly due to its retrospective nature. There may have been missed cases and we were not able to obtain information on whether there was a recurrence in the cases included in the study. Our most important limitation was the lack of biopsy culture results in most patients since imaging-guided biopsy was not performed in our hospital.
Conclusion
In conclusion, our study provides updated data that can contribute to the literature on VO cases in the last decade. In particular, confirmation of the diagnosis with biopsy and initiation of agent-specific treatment will be an important step in increasing treatment success. In regions where brucellosis is endemic, imaging methods such as MRI and CT should be used early to detect vertebral osteomyelitis in the early period. In our study, we found that CRP and ESR values decreased significantly at the 3rd week on average and we think that they can be used for follow-up. It is one of the important conclusions of our study that the decrease in pain in the 3rd week at clinical follow-up can be used together with CRP and ESR values. Our results are also instructive for clinical applications that question the necessity of long-term antibiotic treatment.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
The requirement for informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
CRP: C-reactive protein
CT: Computed tomography
DM: Diabetes mellitus
ESR: Erythrocyte sedimentation rate
HTC: Hematocrit
MRI: Magnetic resonance imaging
VO: Vertebral osteomyelitis
WBC: White blood cell count
References
-
Nickerson EK, Sinha R. Vertebral osteomyelitis in adults: an update. Br Med Bull. 2016;117(1):121-138. doi:10.1093/bmb/ldw003
-
Akiyama T, Chikuda H, Yasunaga H, Horiguchi H, Fushimi K, Saita K. Incidence and risk factors for mortality of vertebral osteomyelitis: a retrospective analysis using the Japanese Diagnosis Procedure Combination database. BMJ Open. 2013;3(3). doi:10.1136/bmjopen-2012-002412
-
Mustapić M, Višković K, Borić I, Marjan D, Zadravec D, Begovac J. Vertebral osteomyelitis in adult patients: characteristics and outcome. Acta Clin Croat. 2016;55(1):9-15. doi:10.20471/acc.2016.55.01.2
-
D’Agostino C, Scorzolini L, Massetti AP, et al. A 7-year prospective study on spondylodiscitis: epidemiological and microbiological features. Infection. 2010;38(2):102-107. doi:10.1007/s15010-009-9340-8
-
Mete B, Kurt C, Yilmaz MH, et al. Vertebral osteomyelitis: 8 years’ experience of 100 cases. Rheumatol Int. 2012;32(11):3591-3597. doi:10.1007/s00296-011-2233-z
-
Mylona E, Samarkos M, Kakalou E, Fanourgiakis P, Skoutelis A. Pyogenic vertebral osteomyelitis: a systematic review of clinical characteristics. Semin Arthritis Rheum. 2009;39(1):10-17. doi:10.1016/j.semarthrit.2008.03.002
-
Eren Gök S, Kaptanoğlu E, Celikbaş A, et al. Vertebral osteomyelitis: clinical features and diagnosis. Clin Microbiol Infect. 2014;20(10):1055-1060.
-
Courjon J, Lemaignen A, Ghout I, et al. Pyogenic vertebral osteomyelitis of the elderly: characteristics and outcomes. PLoS One. 2017;12(12). doi:10.1371/journal.pone.0188470
-
Fantoni M, Trecarichi EM, Rossi B, et al. Epidemiological and clinical features of pyogenic spondylodiscitis. Eur Rev Med Pharmacol Sci. 2012;16(suppl 2):2-7.
-
Pola E, Taccari F, Autore G, et al. Multidisciplinary management of pyogenic spondylodiscitis: epidemiological and clinical features, prognostic factors, and long-term outcomes in 207 patients. Eur Spine J. 2018;27(suppl 2):229-236. doi:10.1007/s00586-018-5598-9
-
Elbahr UŞ, Özdemir Y, Karaali R, et al. Vertebral osteomyelitis: what has changed in last 10 years? Phnx Med J. 2023;5(2):87-93. doi:10.38175/phnx.1239682
-
Turunc T, Demiroglu YZ, Uncu H, Colakoglu S, Arslan H. A comparative analysis of tuberculous, brucellar, and pyogenic spontaneous spondylodiscitis patients. J Infect. 2007;55(2):158-163. doi:10.1016/j.jinf.2007.04.002
-
Grammatico L, Baron S, Rusch E, et al. Epidemiology of vertebral osteomyelitis in France: analysis of hospital-discharge data 2002-2003. Epidemiol Infect. 2008;136(5):653-660. doi:10.1017/s0950268807008850
-
Weissman S, Parker RD, Siddiqui W, Dykema S, Horvath J. Vertebral osteomyelitis: retrospective review of 11 years of experience. Scand J Infect Dis. 2014;46(3):193-199. doi:10.3109/00365548.2013.868600
-
Berbari EF, Kanj SS, Kowalski TJ, et al. Infectious Diseases Society of America. 2015 Infectious Diseases Society of America clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin Infect Dis. 2015;61(6). doi:10.1093/cid/civ482
-
Cornett CA, Vincent SA, Crow J, Hewlett A. Bacterial spine infections in adults: evaluation and management. J Am Acad Orthop Surg. 2016;24(1):11-18. doi:10.5435/jaaos-d-13-00102
-
Kwon JW, Hyun SJ, Han SH, Kim KJ, Jahng TA. Pyogenic vertebral osteomyelitis: clinical features, diagnosis, and treatment. Korean J Spine. 2017;14(2):27-34. doi:10.14245/kjs.2017.14.2.27
-
Rosahl SK, Gharabaghi A, Zink PM, Samii M. Monitoring of blood parameters following anterior cervical fusion. J Neurosurg. 2000;92(2 suppl):169-174. doi:10.3171/spi.2000.92.2.0169
-
Jean M, Irisson JO, Gras G, et al. Diagnostic delay of pyogenic vertebral osteomyelitis and its associated factors. Scand J Rheumatol. 2017;46(1):64-68. doi:10.3109/03009742.2016.1158314
-
Yoon SH, Chung SK, Kim KJ, et al. Pyogenic vertebral osteomyelitis: identification of microorganism and laboratory markers used to predict clinical outcome. Eur Spine J. 2010;19(4):575-582. doi:10.1007/s00586-009-1216-1
-
Herren C, Jung N, Pishnamaz M, et al. Spondylodiscitis: diagnosis and treatment options. Dtsch Arztebl Int. 2017;114(51-52):875-882. doi:10.3238/arztebl.2017.0875
-
Zarghooni K, Röllinghoff M, Sobottke R, Eysel P. Treatment of spondylodiscitis. Int Orthop. 2012;36(2):405-411. doi:10.1007/s00264-011-1425-1
-
Lacasse M, Derolez S, Bonnet E, et al. 2022 SPILF clinical practice guidelines for the diagnosis and treatment of disco-vertebral infection in adults. Infect Dis Now. 2023;53(3):104647. doi:10.1016/j.idnow.2023.01.007
Tables
Table 1. Demographic and clinical characteristics of patients with vertebral osteomyelitis

n: number, %: percentage.
Table 2. Risk factors in the development of vertebral osteomyelitis
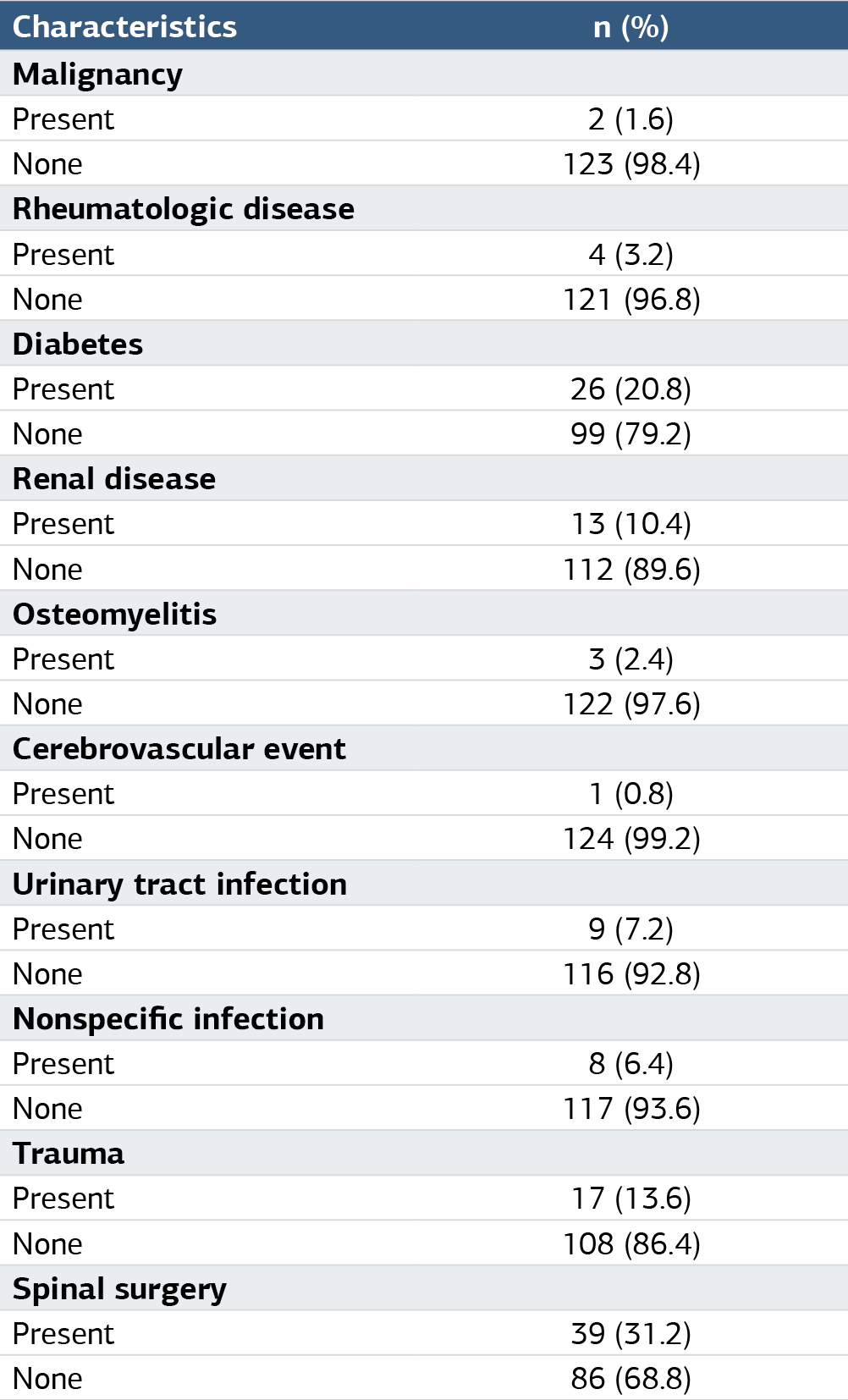
n:number, %:percentage.
Table 3. Laboratory results of patients with vertebral osteomyelitis
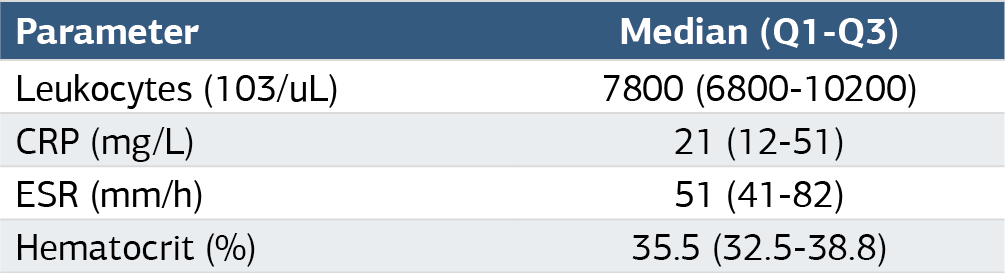
CRP: C-reactive protein, ESR: Erythrocyte sedimentation rate, ul: Microliter, l: Liter, mm/h: Millimeter/hour, %: Percent.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Nurbanu Sezak, Burcu Açıkalın Arıkan, Gülçin Oltulu, Özge Eren Korkmaz. Evaluation of patients with vertebral osteomyelitis diagnosis: ten years of experience. Ann Clin Anal Med 2025;16(5):355-359. doi:10.4328/ACAM.22458
- Received:
- October 16, 2024
- Accepted:
- November 25, 2024
- Published Online:
- December 24, 2024
- Printed:
- May 1, 2025