
Ventilator associated tracheobronchitis; prospective investigation ofetiology, laboratory, treatment and prognosis
Ventilator associated tracheobronchitis
Authors
Abstract
AimVentilator-associated tracheobronchitis (VAT) is an intermediate process between lower respiratory tract colonization and ventilator-associated pneumonia (VAP). This study aimed to provide data on etiologic, laboratory, treatment, and prognostic factors to prevent VAT.
MethodsThe study was conducted in tertiary general intensive care units (ICUs) in two different hospitals. The data were prospectively recorded on the forms prepared by visiting the ICUs daily.
ResultsThree hundred and seventeen patients were included in the study. VAT developed in 54 (14.1%) patients, and VAP developed in 108 (28.3%) patients. VAT developed in an average of 10 ± 7 days (3-35 days) during mechanical ventilatory support. Twenty-eight (51.9%) of the patients developed VAP during VAT. Inappropriate antibiotic use and prolonged stay in the ICU (>21 days) were the independent risk factors for the development of VAP following VAT. The most common microorganisms in patients who developed VAT were A.baumannii (38.9%) and K.pneumoniae (29.6%). Multidrug resistance was detected in 76% of the microorganisms. When the risk factors for the development of VAT were evaluated, prolonged stay in the ICU (>14 days), diabetes mellitus, and application of a nasogastric tube were independent risk factors. Mortality developed in 11 (20.4%) in patients with VAT.
ConclusionInappropriate antibiotic use and prolonged stay in the ICU were the independent risk factors for the development of VAP following VAT. Prolonged stay in the ICU, male gender, diabetes mellitus, and application of a nasogastric tube were identified as independent risk factors for the development of VAT.
Keywords
Introduction
Nosocomial lower respiratory tract infections are the most common type of nosocomial infections observed in the intensive care unit (ICU).1 While mechanical ventilation is a lifesaving intervention in the ICU, it may cause important risks and complications, such as ventilator-associated lower respiratory tract infections, including ventilator-associated pneumonia (VAP) and ventilator-associated tracheobronchitis (VAT).2 Invasive mechanical ventilation via an endotracheal tube is an important risk factor for nosocomial lower respiratory tract infections. The major routes for acquiring nosocomial lower respiratory tract infections are oropharyngeal colonization by the endogenous flora of the host or by pathogens acquired exogenously from the ICU environment, particularly the hands or apparel of health-care workers or contaminated respiratory equipment, hospital water, or air.3 The stomach is a potential site of secondary colonization and also a reservoir of nosocomial Gram-negative bacilli. The occurrence of endotracheal-tube biofilm formation plays an important contributory role in sustaining tracheal colonization, and additionally, it also has an important effect in late-onset nosocomial lower respiratory tract infections caused by resistant organisms. Contaminated oropharyngeal, gastric, or tracheal secretions around the cuffed endotracheal tube cause nosocomial infections in the normally sterile lower respiratory tract.4,5
Although there are numerous studies related to VAP, there are a small number of studies related to nosocomial VAT. As far as the literature can be evaluated, there are only three studies evaluating risk factors in VAT. There is no study on VAT in our country. In this study, it was aimed to obtain data for the prevention of VAT by determining the risk factors, etiological agents, and therapeutic information.
Materials and Methods
The study was performed prospectively in the third-level general ICUs of X Hospital (Centre A) and Y Hospital (Centre B) between 1 April 2018 and 1 April 2019. Two ICUs with ten beds each were investigated in each hospital.
Inclusion and Exclusion CriteriaPatients over 18 years of age who were admitted to the ICU for longer than 48 hours and received mechanical ventilator support were included in the study. VAT was defined according to the following criteria: fever (>38 °C) with no other recognizable cause, increased volume and purulence of tracheal secretions and positive culture of tracheal aspirate (≥105 cfu/mL), and the absence of new infiltration on chest radiograph.6 All infections were accompanied by microbiological documentation. The diagnosis of VAP was made according to the Centers for Disease Control and Prevention criteria. VAP was defined by the presence of at least one of the following: new or progressive and persistent infiltrate, consolidation or cavitation on chest radiograph; at least one of the following: body temperature of more than 38.5 °C or less than 36.5 °C or leucocyte count greater than 12,000 cells per μL or less than 4,000 cells per μL or altered mental status (for adults >70-year old); and at least two of the following: new onset of purulent or changes in sputum, new onset or worsening tachypnea, rales/bronchial breath sounds, worsening gas exchange with increased vent requirements; and at least one of the following: positive blood culture not related to another infection, positive pleural fluid culture, positive quantitative culture (BAL or PSB), BAL fluid with >5% cells with intracellular bacteria on microscopy or positive histopathology.7 The first episode of VAT was included in the study. Patients with a previous episode of VAP and immunocompromised patients were excluded from the study. The demographic characteristics, underlying diseases, possible risk factors, clinical and laboratory findings of developed nosocomial infections, treatment, treatment response, and mortality data of the patients were prospectively recorded on the forms prepared by visiting the ICU daily.
Ethical ApprovalThe study was approved by the Ethics Committee of Kocaeli University (Date: 01.03.2018, Decision No: GÜ-GOKAEK-2018/99).
Statistical AnalysisThe study data were analyzed by using SPSS 17.0 (Statistical Package for Social Sciences Inc.) software. The Chi-square test was used for the evaluation of dependent variables, and logistic regression analysis was used for the evaluation of risk factors for independent variables in the statistical analysis. A p-value of <0.05 was considered to be statistically significant.
Reporting GuidelinesThis study was reported in accordance with the STROBE guideline.
Results
Three hundred and seventeen patients (250 in Centre A, 132 in Centre B) who were admitted to the ICU, received mechanical ventilatory support, and met the eligibility criteria were included in the study. VAT developed in 54 (14.1%) patients, and VAP developed in 108 (28.3%) patients. Thirty-six (66.7%) patients were male in patients with VAT, and the mean age of the patients was 75 ± 11 years (28-93 years). The mean ICU stay length was 45 ± 43 days (9-265 days). VAT developed in an average of 10 ± 7 days (3-35 days) during mechanical ventilatory support.
When the risk factors for the development of VAT were investigated in the patient group receiving mechanical ventilation support, prolonged stay in the ICU (>14 days) (p=0.000), diabetes mellitus (p=0.011), cerebrovascular event (p=0.034) and application of a nasogastric tube (p=0.000) were statistically significantly higher in patients developing VAT compared to patients not developing VAT (Table 1).
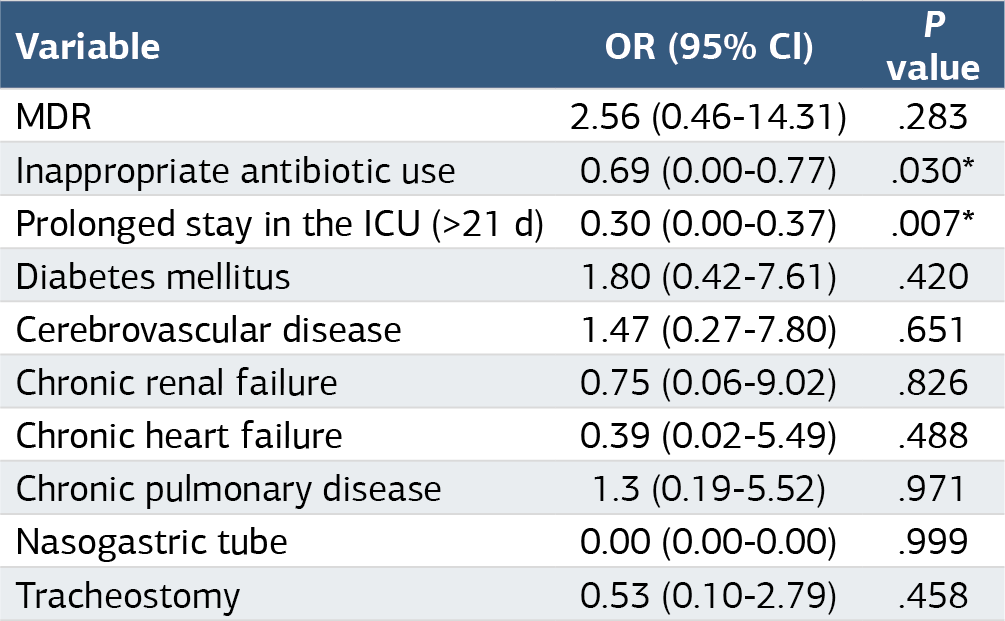
The most frequently determined microorganisms in patients developing VAT were A.baumannii 21 (38.9%), K.pneumoniae 16 (29.6%) and P.aeruginosa 12 (22.2%). Forty-one causative agents (76%) were multidrug-resistant (MDR) organisms in patients with VAT. VAP developed following VAT in 28 (51.9%) of VAT patients. When VAT and VAP developed following VAT were compared, prolonged stay in the ICU (>21 days) (p=0.007) and inappropriate antibiotic use (p=0.030) was higher in patients whose VAP developed following VAT. The independent risk factors for the development of VAP developed following VAT (Table 2).
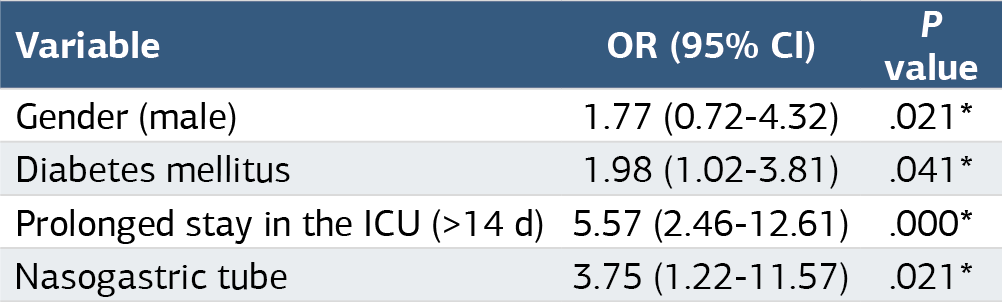
When the risk factors for the development of VAT were investigated in the patient group receiving mechanical ventilation support, prolonged stay in the ICU (>14 days) (p=0.000), malignancy (p=0.016), diabetes mellitus (p=0.011), cerebrovascular event (p=0.034) and application of a nasogastric tube (p=0.000) were statistically significantly higher in patients developing VAT compared to patients not developing VAT (Table 2). Both groups included patients who developed VAP. Prolonged stay in the ICU (>14 days) [OR = 5.57 (2.46-12.61)], male gender [OR = 1.77 (0.72-4.32) ], diabetes mellitus [OR = 1.98 (1.02-3.81)] and application of a nasogastric tube [OR = 3.75 (1.22-11.57)] were independent risk factors for the development of VAT (Table 3).
All of the patients developing VAT received antibiotic treatment.
The mortality developed in 11 (20.4%) of patients developing VAT.
Discussion
VAT is a major health problem in ICU patients receiving mechanical ventilatory support worldwide, and it causes high resource consumption in all countries.8 Pathogen microorganisms cause tracheal colonization by bypassing pulmonary host defenses in patients receiving long-term mechanical ventilation in the ICU.9 This condition may result in VAP during VAT and afterward. VAT is an intermediate process between lower respiratory tract colonization and VAP. Post-mortem studies have demonstrated that there is a continuity between bronchitis and pneumonia in mechanically ventilated ICU patients.10,11 The frequency of VAT is reported estimated to be approximately 11.5%.12 The frequency of VAT (14.1%) was determined to be higher in this study. The VAT ratio obtained in this study is the highest detected in studies to date. Additionally, the development of VAP after VAT in this study’s patients was determined to be as high as 51.9%. The development of VAP after VAT is reported to be between 9% and 34% in various studies.6,11,13,14 In a prospective observational study performed on VAT patients, Nseir et al.15,16,17,18 reported an appropriate antibiotic treatment is independently associated with reduced risk for transition from VAT to VAP. In this study, prolonged stay in the ICU (>21 days) (p=0.007) and inappropriate antibiotic use (p=0.030) were the independent risk factors for the development of VAP following VAT. The use of antibiotics in patients with VAT is not clear as a recommendation. The potential undesirable consequences of antibiotic therapy include high costs and side effects such as rash, C.difficile colitis, and antibiotic resistance. Therefore, antibiotic treatment of patients with VAT has not been supported by existing guidelines. On the other hand, studies are showing that VAP development decreases after VAT with appropriate antibiotic use.8
In this study, A.baumannii, K.pneumoniae, and P.aeruginosa were the most frequently determined microorganisms. In various studies investigating the causative agents in VAP and VAT, similar microbiological data were observed.19,20,21 MDR organisms were determined to be present at a rate of 32% and 63% in patients developing VAT.2,19,21 In this study, a high rate of MDR organisms, 76%, was determined. Appropriate antibiotic use, hand hygiene, care bundles, and training are necessary to prevent the development of MDR microorganisms in ventilator-associated lower respiratory tract infections. Being over 60 years old, the presence of chronic obstructive pulmonary disease, and the use of antibiotics within the last two weeks have been previously determined to be risk factors in patients with VAT.6 In another study, mechanical ventilation day, tracheostomy, and length of stay in the ICU and hospital were determined to be significantly higher in the group developing VAT compared to the control group.14 In this study, prolonged stay in the ICU (>14 days), diabetes mellitus, male gender, and nasogastric tube application were independent risk factors for the development of VAT. Dysfunction develops in the immune system with advanced age and diabetes mellitus. Nasogastric tube application in patients may lead to the colonization of oropharyngeal and gastric microorganisms and subsequent microaspiration. Long stays in ICUs, increasingly invasive interventions, and the use of drugs lead to the colonization of microorganisms. Therefore, hospitalization indications in ICUs should be questioned regularly for each patient. Although risk factors have been investigated in many studies about VAP, risk factor data about VAT are insufficient. It is important to know the risk factors related to the development of VAT in terms of determining the precautions to be taken. Therefore, determining the risk factors for VAT development in this study will contribute to the literature.
The mortality rate has been reported to be between 29% and 42% in various studies.6,21 There was a mortality rate of 11 (20.4%) in patients developing VAT in this study. VAT is a common nosocomial lower respiratory tract infection in ICUs. The VAT ratio obtained in this study is the highest detected in studies to date. The development of VAP after VAT in these patients was determined to be the highest compared to previous studies. Inappropriate antibiotic use and prolonged stay in the ICU were the independent risk factors for the development of VAP following VAT. The rate of MDR among causative microorganisms in VAT in ICUs in this study is the highest detected in studies to date. Long-term hospitalization, diabetes mellitus, and application of nasogastric tubes were identified as independent risk factors for the development of VAT in this study.
Limitations
The limitation of our study is that it was performed with a limited number of patients. Studies performed in more centers and with more patients are needed.
Conclusion
Appropriate antibiotic use, hand hygiene, care bundles, and training are necessary to prevent the development of MDR microorganisms in ventilator-associated lower respiratory tract infections. The presence of foreign bodies and indications for hospitalization in ICUs should be regularly questioned for each patient, especially in patients with advanced age and diabetes mellitus.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants or their legally authorized representatives before enrollment in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
BAL: Bronchoalveolar lavage
CRP: C-reactive protein
ICU: Intensive care unit
MDR: Multidrug-resistant
VAT: Ventilator-associated tracheobronchitis
References
-
Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):2323-2329. doi:10.1001/jama.2009.1754
-
Kollef MH. Prevention of ventilator-associated pneumonia or ventilator-associated complications: a worthy, yet challenging, goal. Crit Care Med. 2012;40(1):271-277. doi:10.1097/ccm.0b013e318232e41d
-
Craven DE, Chroneou A, Zias N, Hjalmarson KI. Ventilator-associated tracheobronchitis: the impact of targeted antibiotic therapy on patient outcomes. Chest. 2009;135(2):521-528. doi:10.1378/chest.08-1617
-
Nseir S, Ader F, Marquette CH. Nosocomial tracheobronchitis. Curr Opin Infect Dis. 2009;22(2):148-153. doi:10.1097/qco.0b013e3283229fdb
-
Metheny NA, Clouse RE, Chang YH, Stewart JB, Oliver DA, Kollef MH. Tracheobronchial aspiration of gastric contents in critically ill tube-fed patients: frequency, outcomes, and risk factors. Crit Care Med. 2006;34(4):1007-1015. doi:10.1097/01.ccm.0000206106.65220.59
-
Nseir S, Di Pompeo C, Pronnier P, et al. Nosocomial tracheobronchitis in mechanically ventilated patients: incidence, aetiology, and outcome. Eur Respir J. 2002;20(6):1483-1489. doi:10.1183/09031936.02.00012902
-
Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309-332. doi:10.1016/j.ajic.2008.03.002
-
Martin-Loeches I, Povoa P, Rodríguez A, et al. Incidence and prognosis of ventilator-associated tracheobronchitis: TAVeM; a multicentre, prospective, observational study. Lancet Respir Med. 2015;3(11):859-868. doi:10.1016/s2213-2600(15)00326-4
-
Craven DE, Hudcova J, Craven KA, Scopa C, Lei Y. Antibiotic treatment of ventilator-associated tracheobronchitis: to treat or not to treat? Curr Opin Crit Care. 2014;20(5):532-541. doi:10.1097/mcc.0000000000000130
-
Kalil AC, Metersky ML, Klompas M, et al. Executive summary: management of adults with hospital-acquired and ventilator-associated pneumonia; 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):575-582. doi:10.1093/cid/ciw504
-
Nseir S, Favory R, Jozefowicz E, et al. Antimicrobial treatment for ventilator-associated tracheobronchitis: a randomized, controlled, multicenter study. Crit Care. 2008;12(3). doi:10.1186/cc6890
-
Dallas J, Skrupky L, Abebe N, Boyle WA, Kollef MH. Ventilator-associated tracheobronchitis in a mixed surgical and medical ICU population. Chest. 2011;139(3):513-518. doi:10.1378/chest.10-1336
-
Karvouniaris M, Makris D, Manoulakas E, et al. Ventilator-associated tracheobronchitis increases the length of intensive care unit stay. Infect Control Hosp Epidemiol. 2013;34(8):800-808. doi:10.1086/671274
-
Agrafiotis M, Siempos II, Falagas ME. Frequency, prevention, outcome, and treatment of ventilator-associated tracheobronchitis: systematic review and meta-analysis. Respir Med. 2010;104(3):325-336. doi:10.1016/j.rmed.2009.09.001
-
Nseir S, Martin-Loeches I, Makris D, et al. Impact of appropriate antimicrobial treatment on transition from ventilator-associated tracheobronchitis to ventilator-associated pneumonia. Crit Care. 2014;18(3). doi:10.1186/cc13940
-
Pontes LG, Menezes FG, Gonçalves P, et al. Risk factors for mortality in ventilator-associated tracheobronchitis: a case-control study. Einstein (Sao Paulo). 2017;15(1):61-64. doi:10.1590/s1679-45082017ao3865
-
Inchai J, Pothirat C, Liwsrisakun C, Deesomchok A, Kositsakulchai W, Chalermpanchai NB. Ventilator-associated pneumonia: epidemiology and prognostic indicators of 30-day mortality. Jpn J Infect Dis. 2015;68(3):181-186. doi:10.7883/yoken.jjid.2014.282
-
Phu VD, Nadjm B, Duy NHA, et al. Ventilator-associated respiratory infection in a resource-restricted setting: impact and etiology. J Intensive Care. 2017;5:69. doi:10.1186/s40560-017-0266-4
-
Craven DE, Lei Y, Ruthazer R, Sarwar A, Hudcova J. Incidence and outcomes of ventilator-associated tracheobronchitis and pneumonia. Am J Med. 2013;126(6):542-549. doi:10.1016/j.amjmed.2012.12.012
-
Hashemi SH, Hashemi N, Esna-Ashari F, Taher A, Dehghan A. Clinical features and antimicrobial resistance of bacterial agents of ventilator-associated tracheobronchitis in Hamedan, Iran. Oman Med J. 2017;32(5):403-408. doi:10.5001/omj.2017.76
-
Nseir S, Di Pompeo C, Soubrier S, et al. Effect of ventilator-associated tracheobronchitis on outcome in patients without chronic respiratory failure: a case-control study. Crit Care. 2005;9(3). doi:10.1186/cc3508
Tables
Table 1. Comparison of baseline characteristics of patients with or without VAT

*Significant
Table 2. The independent risk factors for the development of VAP following VAT
*Significant
Table 3. The independent risk factors for the development of VAT
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Hasan Naz, Duru Mıstanoğlu Ozatag, Esra Arslanalp, Pınar Korkmaz, Hande Gürbüz. Ventilator associated tracheobronchitis; prospective investigation ofetiology, laboratory, treatment and prognosis. Ann Clin Anal Med 2025;16(5):360-363. doi:10.4328/ACAM.22459
- Received:
- October 16, 2024
- Accepted:
- November 25, 2024
- Published Online:
- December 2, 2024
- Printed:
- May 1, 2025