
Clinicopathological features of patients with human epidermal growth factor receptor 2 (HER2) immunohistochemistry 2+ early-stage breast cancer
HER2 2+ early breast cancer
Authors
Abstract
AimHuman epidermal growth factor receptor 2 (HER2) 2+ with immunohistochemistry early breast cancer was evaluated with in situ hybridization (ISH) as a further assessment. Positive and negative groups may have different characteristics. This study aimed to investigate the clinicopathological characteristics of these groups.
MethodsPatients with HER2 2+ early breast cancer were evaluated. ISH-positive and negative groups were compared according to patient and disease characteristics, tumor markers, and inflammatory parameters.
ResultsAbout a quarter of the patients were ISH-positive. Many patient and disease characteristics were similar between the two groups. CEA levels were higher in the positive group. There was a negative correlation between HER2/CEP17 ratio and PR and a positive correlation between HER2/CEP17 ratio and CEA.
ConclusionHER2 2+ early breast cancer is a very heterogeneous disease, and patients can be assessed individually. Also, larger trials are needed to determine the benefit of new treatments.
Keywords
Introduction
Breast cancer is regarded as a heterogeneous tumor group, exhibiting variability in terms of underlying biology, pathological features such as hormone status and surface receptor expression, response to treatment, and clinical outcome.1
Human epidermal growth factor 2 (HER2)-positive breast cancer represents between 10 and 34% of all breast carcinomas and is characterized by the amplification of the ERBB2/HER2 gene and/or overexpression of the associated kinase receptor protein. This results in more aggressive tumor behavior and a reduction in survival rates.2,3 The introduction of the humanized anti-HER2 monoclonal antibody trastuzumab into clinical practice, followed by the development of several other anti-HER2 targeted agents, has resulted in enhanced outcomes in both early-stage and metastatic disease.4,5
By the ASCO/CAP guidelines, a clinically diagnosed HER2(+) breast cancer is defined as a tumor exhibiting complete and intense peripheral membrane staining for HER2 protein (3+ score) by immunohistochemistry (IHC) and/or HER2 gene (ERBB2) amplification by in situ hybridization (ISH). Additionally, the HER2/CEP17 ratio must be 2.0, and the mean HER2 gene copy number must exceed 4.0 signals/cell. This definition is based on that used in HER2+ clinical trials evaluating trastuzumab and other targeted therapies. However, the clinical presentation of HER2+ disease is, in fact, a more complex and heterogeneous entity, which requires further study to facilitate the development and validation of new and more effective diagnostic and therapeutic approaches.6,7,8,9
There is a paucity of knowledge and a lack of consensus regarding the characteristics of IHC 2+ HER2-positive early breast cancer. The objective of the present study was to evaluate the relationship between the disease, patient features, and HER2 status.
Materials and Methods
The medical records of 81 women diagnosed with HER2 IHC 2+ breast cancer and admitted to Ankara Bilkent City Hospital between 2020 and 2023 were subjected to case-control analysis.
The study population comprised patients aged 18 and over who had been diagnosed with early-stage breast cancer with an IHC score of 2 in biopsy samples. Patients with advanced breast cancer were excluded from the study.
The following variables were evaluated: age at diagnosis, Eastern Cooperative Oncology Group (ECOG) performance status, biochemical laboratory values at diagnosis, estrogen receptor status, stage at diagnosis, and tumor marker levels. The study also assessed inflammatory parameters, including the neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR). The patients were divided into two groups according to the results of fluorescein in situ hybridization (FISH) testing. A comparison was made between the patient and disease characteristics and laboratory values of the two groups. The correlation between the numerical values was subjected to analysis.
Ethical ApprovalThis study was approved by the Ethics Committee of Ankara Bilkent City Hospital (Date: 07.02.2024, Decision No: E2-24-6181).
Statistical AnalysisIBM SPSS version 25 was used for all statistical analyses. Shapiro-Wilk test and histograms were used to test normal distribution. Normally distributed numerical values were expressed as mean and standard deviation, and non-normally distributed values were expressed as median (min-max). Chi-square and Fisher-exact tests were used for the comparison of categorical variables between the two groups. Mann Whitney U test was used for comparison of numerical values. Spearman test was used for correlation analysis. p<0.05 was considered significant.
Reporting GuidelinesThis study was reported in accordance with the STROBE guidelines.
Results
All 81 patients were women, and 26.7% of patients were FISH-positive. Between FISH-positive and negative groups, age, medical history, family history, performance status, T stage, N stage, and histological grades were similar. Most patients were hormone receptor-positive in both groups (Table 1). For FISH-positive and negative groups, hormone receptor expressions, Ki67 index, and CA15-3 levels were similar. CEA levels were higher in the positive group. As inflammatory markers, NLR and PLR were not significantly different (Table 2).
HER2/CEP17 ratio had a weak significant correlation between progesterone receptor expression and CEA levels (p=0.024 r = -0.27, p=0.003 r = 0.358 respectively) (Figure 1, Figure 2). There was no correlation between the HER2/CEP17 ratio and estrogen receptor or CA15-3 levels (p=0.12 and p=0.24, respectively).
Discussion
The findings of this study indicate that FISH-positive and FISH-negative diseases present with numerous similarities, with only a few notable differences, such as serum tumor marker levels. Additionally, gene amplifications were found to be associated with progesterone receptor and CEA levels.
Bahremani et al.10 evaluated HER2 2+ breast cancer patients in the Iranian population using resection and fine needle biopsy materials. They divided the patients into two groups based on the results of chromogenic in situ hybridization (CISH) testing: CISH-positive and CISH-negative. In contrast with the findings of our study, the researchers observed that the CISH-negative group had a significantly higher prevalence of hormone receptor-positive cases. The CISH-positive group exhibited a higher Ki-67 index. These discrepancies may be attributed to differences in the characteristics of the studied populations. The median ages of the two groups were similar to those observed in our study.
The study of Zaidoon et al.11 concluded that there was a higher prevalence of hormone receptor expression in the gene-amplified group and a negative correlation between both estrogen and progesterone receptors and HER2 amplification. Thus, a negative correlation was identified between PR and the HER2/CEP17 ratio. However, no such correlation was observed for ER. Ji et al.12 demonstrated that the HER2 FISH-amplified group exhibited a reduced frequency of ER and PR. Additionally, a positive correlation was observed between Ki67 and gene amplification, as evidenced by several other studies.13,14 These findings contradict our own, potentially due to limitations in our sample size and features. Conversely, Alsafi et al.15 corroborated our findings. Their study did not identify a correlation between gene amplification and the Ki67 index.
The latest data indicates that inflammatory markers may influence the prognosis of HER2-positive disease. The HELENA study investigated the prognosis of early-stage breast cancer and demonstrated that HER2 2+ cases exhibited superior outcomes compared to HER2+ cases. Additionally, the study indicated that the neutrophil-to-lymphocyte ratio (NLR) did not exert a notable influence on prognosis.16 Furthermore, the evaluation of inflammatory markers, specifically NLR and PLR, did not reveal any notable differences. The results of several studies have been inconclusive about these markers. In a study of early-stage breast cancer, it was concluded that NLR and PLR were not significant markers for disease-free survival.17 Two distinct studies have reached the same conclusion: that patients with HER2-positive metastatic breast cancer who have a high level of NLR tend to have better outcomes.18,19 Another study revealed that PLR was an independent risk factor for survival.20 In their investigation of the characteristics of equivocal HER2 early breast cancer, Al-Zadjali et al.21 found no significant differences in hormonal status or neutrophil-to-lymphocyte ratio (NLR) between groups based on FISH results.
Limitations
It should be noted that the present study is subject to several limitations. The quality of the analysis was constrained by the retrospective nature of the study and the presence of missing data. Additionally, the limited sample size and the exclusive reliance on data from a single center posed challenges for a comprehensive evaluation. Nevertheless, to the best of our knowledge, this is the inaugural investigation into the clinicopathological features of HER2 IHC2+ disease within our population.
Conclusion
HER2 IHC2+ breast cancer is a heterogeneous disease, and as such, each patient should be assessed individually. In particular, a tailored approach that incorporates targeted therapies is recommended. Further investigation of different biomarkers and predictive factors may elucidate the optimal management pathway.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
The requirement for informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
CEA: Carcinoembryonic antigen
CEP17: Chromosome enumeration probe 17
ECOG: Eastern Cooperative Oncology Group
ER: Estrogen receptor
FISH: Fluorescence in situ hybridization
HER2: Human epidermal growth factor receptor 2
IHC: Immunohistochemistry
ISH: In situ hybridization
NLR: Neutrophil-to-lymphocyte ratio
PLR: Platelet-to-lymphocyte ratio
PR: Progesterone receptor
References
-
Ali AM, Provenzano E, Bartlett JMS, et al. Prognosis of early breast cancer by immunohistochemistry-defined intrinsic subtypes in patients treated with adjuvant chemotherapy in the NEAT/BR9601 trial: prognosis of early breast cancer. Int J Cancer. 2013;133(6):1470-1478. doi:10.1002/ijc.28150
-
Zhao J, Wu R, Au A, Marquez A, Yu Y, Shi Z. Determination of HER2 gene amplification by chromogenic in situ hybridization in archival breast carcinoma. Mod Pathol. 2002;15(6):657-665. doi:10.1038/modpathol.3880582
-
López-Guerrero JA, Llombart-Cussac A, Noguera R, et al. HER2 amplification in recurrent breast cancer following breast-conserving therapy correlates with distant metastasis and poor survival. Int J Cancer. 2006;118(7):1743-1749.
-
Shah S, Chen B. Testing for HER2 in breast cancer: a continuing evolution. Pathol Res Int. 2010;2011:903202. doi:10.4061/2011/903202
-
Murphy CG, Modi S. HER2 breast cancer therapies: a review. Biologics. 2009;3:289-301. doi:10.2147/btt.s3479
-
Wolff AC, Hammond MEH, Schwartz JN, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol. 2007;25(1):118-145. doi:10.1200/jco.2006.09.2775
-
Tchrakian N, Flanagan L, Harford J, Gannon JM, Quinn CM. New ASCO/CAP guideline recommendations for HER2 testing increase the proportion of reflex in situ hybridization tests and of HER2-positive breast cancers. Virchows Arch. 2016;468(2):207-211. doi:10.1007/s00428-015-1871-z
-
Oh DY, Bang YJ. HER2-targeted therapies: a role beyond breast cancer. Nat Rev Clin Oncol. 2020;17(1):33-48. doi:10.1038/s41571-019-0268-3
-
Atkinson R, Mollerup J, Laenkholm AV, et al. Effects of the change in cutoff values for human epidermal growth factor receptor 2 status by immunohistochemistry and fluorescence in situ hybridization: a study comparing conventional brightfield microscopy, image analysis-assisted microscopy, and interobserver variation. Arch Pathol Lab Med. 2011;135(8):1010-1016. doi:10.5858/2010-0462-oar
-
Hashemi Bahremani M, Ebrahimi A, Fallahi M. Predicting effects of clinicopathological variables on HER2 gene amplification by chromogenic in situ hybridization in IHC HER2 2+ breast cancer patients: a study from Iran. Iran J Pathol. 2020;15(3):217-224.
-
Musa ZA, Qasim BJ, Al Shaikhly AWA. Evaluation of immunohistochemistry-equivocal 2+ HER2 gene status in invasive breast cancer by silver DNA in situ hybridization and its association with clinicopathological variables. Iran J Pathol. 2017;12(1):9-19.
-
Ji Y, Sheng L, Du X, Qiu G, Chen B, Wang X. Clinicopathological variables predicting HER2 gene status in immunohistochemistry-equivocal 2+ invasive breast cancer. J Thorac Dis. 2014;6(7):896-904.
-
Dieci MV, Barbieri E, Bettelli S, et al. Predictors of human epidermal growth factor receptor 2 fluorescence in situ hybridisation amplification in immunohistochemistry score 2+ infiltrating breast cancer: a single-institution analysis. J Clin Pathol. 2012;65(6):503-506. doi:10.1136/jclinpath-2011-200643
-
Shokouh TZ, Ezatollah A, Barand P. Interrelationships between Ki67, HER2/neu, p53, ER, and PR status and their associations with tumor grade and lymph node involvement in breast carcinoma subtypes: retrospective-observational analytical study. Medicine (Baltimore). 2015;94(32). doi:10.1097/md.0000000000001359
-
Abdul Raouf ALSafi R, A Ali S, Hausin Al-Khafaj A, Adnan Habib M. Assessment of HER2/neu gene amplification status by chromogenic in situ hybridization in breast cancer patients with equivocal 2+ HER2/neu immunostaining and its relation to the clinicopathological parameters. Karbala J Med. 2016;9(2):2483-2490.
-
Cherifi F, Da Silva A, Johnson A, et al. HELENA: HER2-low as a predictive factor of response to neoadjuvant chemotherapy in early breast cancer. BMC Cancer. 2022;22(1):1081. doi:10.1186/s12885-022-10163-9
-
Ulas A, Avci N, Kos T, et al. Are neutrophil/lymphocyte ratio and platelet/lymphocyte ratio associated with prognosis in patients with HER2-positive early breast cancer receiving adjuvant trastuzumab? Lung Cancer. 2015;20(3):714-722. doi:10.7314/apjcp.2015.16.4.1643
-
Ding N, Pang J, Liu X, et al. Prognostic value of baseline neutrophil/lymphocyte ratio in HER2-positive metastatic breast cancer: exploratory analysis of data from the CLEOPATRA trial. Breast Cancer Res. 2024;26(1):9. doi:10.1186/s13058-023-01761-x
-
Shao B, Liu X, Li H, et al. Prognostic value of pretreatment neutrophil-to-lymphocyte ratio in HER2-positive metastatic breast cancer. Curr Oncol. 2022;29(9):6154-6166. doi:10.3390/curroncol29090483
-
Song D, Li X, Zhang X. Expression and prognostic value of ratios of platelet lymphocyte, neutrophil lymphocyte, and lymphocyte monocyte in breast cancer patients. Am J Transl Res. 2022;14(5):3233.
-
Yaqeen AZ, Afrah AR, Samya AH, Suaad AB, Hajer AB, Arafa M. Clinicopathological study of breast carcinoma patients with equivocal HER2 immunohistochemical status: 5-year experience from a tertiary care center. Maedica (Bucur). 2023;18(1):27.
Figures
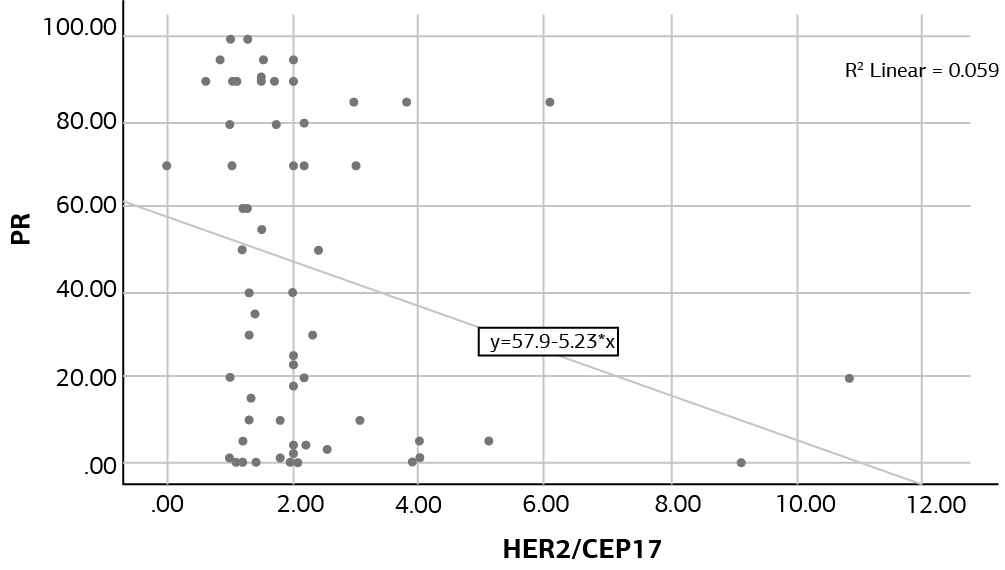
Figure 1. HER2/CEP17 and progesterone receptor expression levels

Figure 2. HER2/CEP17 and CEA levels
Tables
Table 1. Patients and disease characteristics between groups
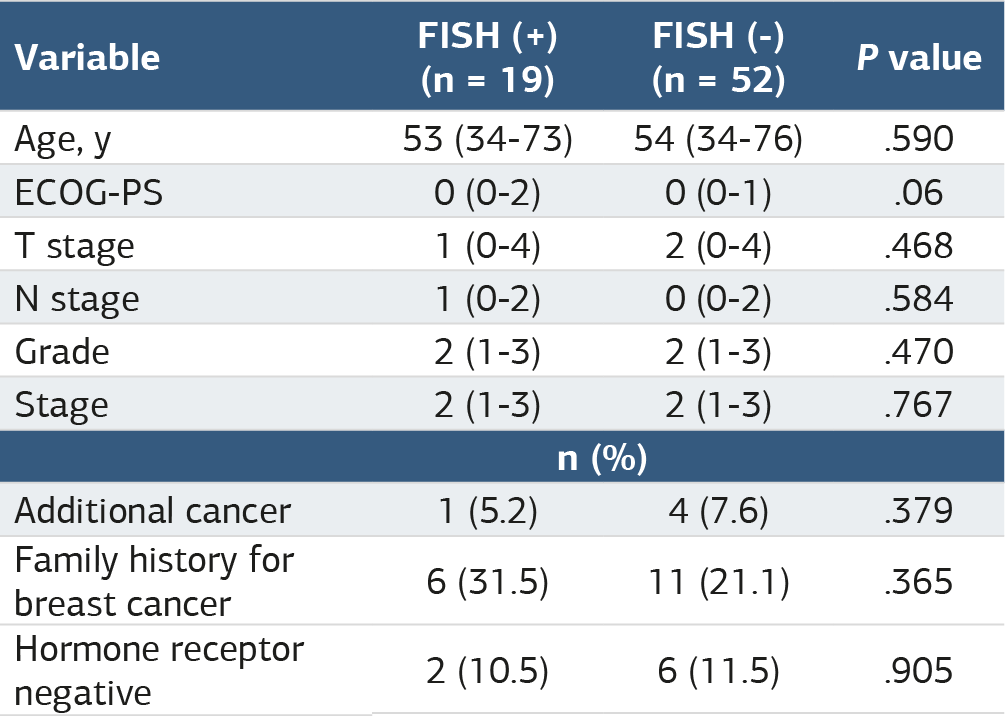
Table 2. Pathological features and laboratory values of groups

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
İsmet Seven, İrfan Karahan, Fahriye Tuğba Köş, Serhat Sekmek, Doğan Bayram, Gökhan Uçar, Doğan Uncu. Clinicopathological features of patients with human epidermal growth factor receptor 2 (HER2) immunohistochemistry 2+ early-stage breast cancer. Ann Clin Anal Med 2025;16(5):369-372. doi:10.4328/ACAM.22464
- Received:
- October 17, 2024
- Accepted:
- November 25, 2024
- Published Online:
- December 4, 2024
- Printed:
- May 1, 2025