
The predictive role of amniotic fluid and serum tenascin X foradverse perinatal outcomes
Tenascin X and adverse perinatal outcomes
Authors
Abstract
AimThere is limited data about the association between tenascin X deficiency and obstetric outcomes. Here, we aimed to search the predictive role of amniotic fluid and serum tenascin X for adverse pregnancy outcomes.
MethodsThis is a prospective study conducted at a university-affiliated hospital between May 2021 and December 2021. A total of 70 patients who underwent amniocentesis for any reason were included. Patients were divided into two groups: adverse pregnancy outcome group (n = 35) and controls (n = 35). Demographic, laboratory and obstetrics features were recorded. Amniotic fluid and serum tenascin X levels were measured using the ELISA method.
ResultsAmniotic fluid tenascin X were 19.1(8.2–39.13)ng/ml in the adverse perinatal outcome group and 22.34(2.91–61.99)ng/ml in control group which was significantly lower in adverse outcome group (p=0.020). Similarly, serum tenascin X levels were lower in adverse perinatal outcome group compared to control group (1.97[1.07–5.85] ng/ml vs 3.03[1.31–8.15] ng/ml, p=0.030). Amniotic fluid tenascin X<20.7ng/ml predicted adverse perinatal outcomes, with a sensitivity of 74.29% and specificity of 65.7% (p=0.016, AUC=0.662). Serum tenascin X≤1.97ng/ml predicted adverse perinatal outcomes with a sensitivity of 54.29% and specificity of 80% (p=0.024, AUC=0.651). The analysis revealed no significant difference between serum and amniotic fluid (p=0.91). Amniotic fluid tenascin X levels were significantly lower in patients who developed gestational diabetes, preterm birth, premature rupture of membranes and an Apgar score ≤7.
ConclusionAmniotic fluid and serum tenascin X could be a valuable marker for predicting adverse perinatal outcomes. Large scaled, prospective randomized studies are needed to clarify this association.
Keywords
Introduction
Tenascins are extracellular matrix glycoproteins that play role in the modulation of cell signaling, collagen deposition and resistance to proteolysis.1 The family is composed of four members: Tenascin C, R, W and X.2 Tenascin C expresses in embrional period, modulates wound healing and neovascularization while tenascin R expresses in central nerve system. Tenascin W expression is limited to developing skeletal tissue and neural crest cells in zebrafish.3
Tenascin X (TNX) regulates connective tissues such as muscles, joints and skin. It provides elasticity and flexibility to connective tissues via stabilizing elastic fibers and producing some types of collagen.4,5 Ehler Danlos Syndrome, a heritable connective tissue disorder, has been shown to be related to TNX deficiency.6 In a study, pregnant women with Ehler Danlos Syndrome were found to be more prone to postpartum hemorrhage, preterm birth and premature rupture of membranes.7,8,9 This situation raises the suspicion that TNX deficiency may be associated with adverse pregnancy outcomes such as preterm birth and premature rupture of membranes. Unfortunately, there is limited data about the association between TNX deficiency and obstetric outcomes.
To the best of our knowledge, this is the first study searching the predictive role of TNX for adverse pregnancy outcomes. Additionally, we aimed to evaluate both second trimester amniotic fluid and serum TNX levels and to determine cut-off levels for adverse perinatal outcomes.
Materials and Methods
This is a single center, prospective study performed at a university affiliated research and training hospital between May 2021 and December 2021. For power analysis, NCSS statistical package program was used and it was determined that a minimum of 66 patients should be included in the study by accepting 80% power and α=0.01. A total of 70 patients who were admitted to the University of Health Sciences, Bursa Yuksek Ihtisas Research and Training Hospital, Department of Obstetrics and Gynecology, Perinatology Outpatients Clinic and underwent amniocentesis for any reason were included in the study. Then, patients were followed for their antenatal visits and adverse pregnancy outcomes were recorded. Adverse perinatal outcomes were defined as having hypertensive disorders of pregnancy, gestational diabetes, preterm birth, preterm premature rupture of membranes, intrauterine growth restriction and Apgar score ≤7. Finally, patients were grouped as adverse pregnancy outcome group (n = 35) and a control group (n = 35).
Inclusion criteria of the study were having single pregnancy, being between 16-35 years old, undergoing amniocentesis between 16-20 weeks of gestation, having regular antenatal visits and birth in our clinic. Pregnant women with any inflammatory or autoimmune disease, hepatic and renal dysfunction, thyroid disorders, smoking or alcohol use, history of stroke and anti-inflammatory drug use were excluded. Age, gravida, parity, height, weight, date of last menstrual period, gestational week confirmed by ultrasound, amniocentesis week, the time between pregnancies, adverse pregnancy outcomes, birth week, birth weight, delivery type, Apgar score, maternal hemoglobin at birth, hematocrit, white blood cell (WBC), platelet, fasting blood glucose, creatinine, aspartate aminotransferase (AST), alanine aminotransferase (ALT), C-reactive protein parameters were recorded.
In our clinic, amniocentesis was performed between 16-20 weeks of gestation by the transabdominal route and 22 gauge needle using the free hand technique, accompanied by ultrasonography. All procedures were performed by the same perinatologist. The first 5 cc fluids taken during amniocentesis and maternal serum samples of all patients were stored in the biochemistry laboratory at -80 degrees. Tenascin X levels were measured by ELISA method.
Ethical ApprovalThis study was approved by the Ethics Committee of Health Science University Bursa Yüksek İhtisas Training and Research Hospital (Date: 12.04.2021, Decision No: 2011-KAEK-25).
Statistical AnalysisNormality assumption was evaluated with Shapiro Wilk test. Variables were expressed as mean ± standard deviation or median (minimum-maximum) values as descriptive statistics. Categorical variables were presented with frequency and related percentage values. Student’s t-test was used to compare normally distributed quantitative data between two groups, and Mann Whitney-U test was used to compare non-normally distributed quantitative data between two groups. Chi-square or Fisher’s Exact test was used to compare categorical data. Receiver operating curve analysis was used to determine the predictive role of amniotic fluid and serum TNX levels for adverse perinatal outcomes. The sensitivity, specificity, Youden index and cut-off values were analyzed. Also, the predictive role of amnion fluid and serum TNX were compared with receiver operating curve analysis. The statistical analysis were performed with SPSS 21.0 program and the level of significance was accepted as α=0.05.
Reporting GuidelinesThis study was reported in accordance with the STROBE guidelines.
Results
A total of 70 patients who underwent amniocentesis were included and grouped as adverse outcome group (n = 35) and control group (n = 35). Hypertensive disorders of pregnancy were detected in 8 (11.4%) patients, gestational diabetes was detected in 7 (10%) patients, preterm birth was detected in 10 (14.3%) patients, preterm premature rupture of the membrane was detected in 9 (12.9%) patients, intrauterine growth restriction was detected in 18 (25.7%) patients and Apgar score ≤7 was detected in 10 (14.3%) patients. The sociodemographic features of adverse perinatal outcomes and control groups were demonstrated in Table 1. No significant difference was detected in terms of age, gravida, parity, abortion, BMI and interval between pregnancies.
The obstetric characteristics of adverse perinatal outcomes and control groups are shown in Table 1. There was no significant difference between two groups in terms of the week of amniocentesis while birth week and weight, Apgar scores of first and fifth minutes were lower in the adverse perinatal outcome group. The Cesarean section rate was significantly higher in the adverse perinatal outcome group.
The laboratory features of adverse perinatal outcome and control groups were presented in Table 2. There was no significant difference between the two groups regarding WBC, hemoglobin, hematocrit, platelet, fasting glucose, creatinine, AST, ALT and C reactive protein levels. Median amniotic fluid TNX levels were 19.1 (8.2- 39.13)ng/ml in adverse perinatal outcome group and 22.34 (2.91- 61.99)ng/ml in control group which was statistically significantly lower (p=0.020). Similarly, median serum TNX levels were significantly lower in adverse perinatal outcome group as compared to control group (1.97 (1.07- 5.85) ng/ml vs 3.03 (1.31- 8.15)ng/ml , p=0.030).
The ROC curve evaluating the role of amniotic fluid TNX in predicting adverse perinatal outcomes is shown in Figure 1.
According to this analysis, amniotic fluid TNX cut-off value of 20.7 was found to be statistically significant in predicting adverse perinatal outcomes with 74.29% sensitivity and 65.7% specificity (p=0.016, AUC=0.662).
The ROC curve evaluating the role of serum TNX in predicting adverse perinatal outcomes is demonstrated in Figure 2. According to this analysis, serum TNX cut-off value of 1.97 was found to be statistically significant in predicting adverse perinatal outcomes with 54.29% sensitivity and 80% specificity (p=0.024, AUC=0.651).
The ROC curve comparing the role of amniotic fluid and serum TNX in predicting adverse perinatal outcomes is presented in Figure 3. The analysis revealed no statistically significant difference between serum and amniotic fluid TNX levels (p=0.91).
Amniotic fluid and serum TNX levels for each adverse perinatal outcome are shown in Table 3. No significant difference was detected between patients with and without hypertensive disorders of pregnancy in terms of amniotic fluid and serum TNX levels. Likewise, there was no significant difference according to amniotic fluid and serum TNX levels in patients with and without intrauterine growth restriction. Serum TNX levels were similar between other subgroups like hypertensive disorders of pregnancy and intrauterine growth restriction whereas amniotic fluid TNX levels were statistically significantly lower in patients who develop gestational diabetes, preterm birth, premature rupture of membrane and Apgar score ≤7.
Discussion
Tenascin X, the largest member of the tenascin family with a weight of 450 kDa, interacts with extracellular matrix components such as fibrils, collagens type I, III, and V and proteoglycans such as decorin.10 Extracellular matrix, composed of fibrous proteins along with various types of collagen, provides the architectural and structural framework of the fetal membranes. Disruption of the collagen-rich extracellular matrix that connects the amnion and chorion layers of the fetal membranes is one of the key events leading to membrane rupture.3,11,12,13 Recent studies have shown that Ehler Danlos syndrome is related to TNX deficiency and low TNX levels could cause an increased risk of preterm premature rupture of membranes in Ehler Danlos cases.8 This condition was explained with the reduced binding of TNX deficient fibroblasts to fibronectin, an important adhesion molecule for fetal membranes.14 Rood and colleagues showed that fetal membranes contained significantly higher levels of TNX compared to myometrium, cervix and placenta. Moreover, it was shown that TNX expression tended to increase in amniotic fluid and decrease in fetal membranes during intraamniotic infection, independent of preterm premature rupture of membranes.3 All these studies has supported the role of TNX deficiency in premature rupture of membranes. Consistently, we found lower TNX levels in preterm birth and premature rupture of membrane cases.
There are limited studies in the literature about the role of TNX on other perinatal outcomes. In a study, searching the effect of TNX levels in human and mouse uterine connective tissues on obstetric complications, TNX deficiency was not found to be related to major complications except one postpartum hemorrhage case. In another study, a shorter pregnancy period was reported in TNX deficient mouses.15 Another study found an increase in abnormal mRNA expression for the tenascin-X gene in euploid fetuses with ventricular septal defects between 19 and 24 weeks of gestation.16
In a study by Alcaraz et al, it was shown that the TNX plays a key role in the conversion of latent TGF-β to an active molecule.17 It is known that obesity, insulin resistance and endothelial dysfunction causing early atherosclerosis occur in women with gestational diabetes. TGF-β1 is a key cytokine in obesity and insulin resistance and also plays an important role in the development of atherosclerosis. Yener et al showed that serum TGF-β1 levels were increased in patients with gestational diabetes mellitus.18 Morisette et al showed that TNX levels in patients with congenital adrenal hyperplasia were associated with TGF-β pathway abnormalities.19 In our study, amniotic fluid TNX levels were lower as compared to non-diabetic patients. We suggest that this condition could be related to increased TGF-β activation due to TNX deficiency which can lead to insulin resistance. It is also known that TNX increases endothelial cell proliferation by binding to VEGF-1.20 There are studies in the literature showing the presence of endothelial dysfunction and decreased VEGF-1 levels in gestational diabetes.21,22 Based on these, another mechanism explaining the relationship between TNX and gestational diabetes may be the decreased VEGF-1 interaction due to TNX deficiency that results in endothelial dysfunction.
Although there is no study about TNX deficiency in hypertension, Liang et al demonstrated that TGF-β is critical for vascular smooth muscle cells differentiation playing a role in atherosclerosis, hypertension, and aortic aneurysm.23 Considering the role of TNX deficiency in increased TGF-β activation, we suggest that TNX deficiency could be associated with hypertensive disorders of pregnancy. Unfortunately, no significant difference was detected between patients with and without hypertensive disorders of pregnancy in terms of amniotic fluid and serum TNX levels. This could be related to the small number of hypertensive cases.
There is no study examining TNX levels in other pregnancy outcomes where inflammation, angiogenesis and fibrogenesis play a role in the etiopathogenesis. Our study primarily showed that serum and amniotic fluid TNX levels were lower in composite adverse perinatal outcomes. Moreover, amniotic fluid TNX <20.7 predicted adverse perinatal outcomes with 74.29% sensitivity and 65.7% specificity and serum TNX <1.97 predicted adverse perinatal outcomes with 54.29% sensitivity and 80% specificity. When we searched for the other outcomes separately, amniotic fluid and serum TNX levels were lower in intrauterine growth restriction while only amniotic fluid TNX levels were lower in patients with low Apgar scores.
Another interesting finding of our study is the comparison of the predictive roles of amniotic fluid and serum TNX levels. The analysis revealed no statistically significant difference between serum and amniotic fluid TNX levels. Although there was no difference between amniotic fluid and serum in composite adverse outcomes, amniotic fluid TNX was found to be more significant between the groups when adverse outcomes examined individually.
Limitations
This study has some limitations. The data arose from single center and it had a small sample size. The predictive role of TNX levels could not be assessed for each outcome due to the small sample size.
Conclusion
Consequently, we suggest that amniotic fluid and serum TNX could be valuable marker for predicting adverse perinatal outcomes. Large scaled, prospective randomized studies are needed to clarify this association.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants before enrollment in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
ALT: Alanine aminotransferase
AST: Aspartate aminotransferase
AUC: Area under the curve
BMI: Body mass index
CRP: C-reactive protein
ELISA: Enzyme-linked immunosorbent assay
ROC: Receiver operating characteristic
TNX: Tenascin X
WBC: White blood cell
References
-
Adams JC, Tucker RP. The evolution of tenascins. BMC Ecol Evol. 2024;24(1):121. doi:10.1186/s12862-024-02306-2
-
Matsumoto KI, Aoki H. The roles of tenascins in cardiovascular, inflammatory, and heritable connective tissue diseases. Front Immunol. 2020;11:609752. doi:10.3389/fimmu.2020.609752
-
Rood KM, Buhimschi CS, Zhao G, et al. Tenascin-X in amniotic fluid and reproductive tissues of pregnancies complicated by infection and preterm prelabor rupture of membranes. Biol Reprod. 2019;100(3):773-782. doi:10.1093/biolre/ioy216
-
Egging DF, van Vlijmen I, Starcher B, et al. Dermal connective tissue development in mice: an essential role for tenascin-X. Cell Tissue Res. 2006;323(3):465-474. doi:10.1007/s00441-005-0100-5
-
Petersen JW, Douglas JY. Tenascin-X, collagen, and Ehlers-Danlos syndrome: tenascin-X gene defects can protect against adverse cardiovascular events. Med Hypotheses. 2013;81(3):443-447. doi:10.1016/j.mehy.2013.06.005
-
Okuda-Ashitaka E, Matsumoto KI. Tenascin-X as a causal gene for classical-like Ehlers-Danlos syndrome. Front Genet. 2023;14:1107787. doi:10.3389/fgene.2023.1107787
-
Spiegel E, Nicholls-Dempsey L, Czuzoj-Shulman N, Abenhaim HA. Pregnancy outcomes in women with Ehlers-Danlos syndrome. J Matern Fetal Neonatal Med. 2022;35(9):1683-1689. doi:10.1080/14767058.2020.1767574
-
Kang J, Hanif M, Mirza E, Jaleel S. Ehlers-Danlos syndrome in pregnancy: a review. Eur J Obstet Gynecol Reprod Biol. 2020;255:118-123. doi:10.1016/j.ejogrb.2020.10.033
-
Syx D, Malfait F. Pathogenic mechanisms in genetically defined Ehlers-Danlos syndromes. Trends Mol Med. 2024;30(9):824-843. doi:10.1016/j.molmed.2024.06.001
-
Lethias C, Carisey A, Comte J, Cluzel C, Exposito JY. A model of tenascin-X integration within the collagenous network. FEBS Lett. 2006;580(26):6281-6285. doi:10.1016/j.febslet.2006.10.037
-
Menon R, Richardson LS. Preterm prelabor rupture of the membranes: a disease of the fetal membranes. Semin Perinatol. 2017;41(7):409-419. doi:10.1053/j.semperi.2017.07.012
-
Moreno SE, Enwerem-Lackland I, Dreaden K, Massee M, Koob TJ, Harper JR. Human amniotic membrane modulates collagen production and deposition in vitro. Sci Rep. 2024;14(1):15998. doi:10.1038/s41598-024-64364-2
-
Strauss JF III. Extracellular matrix dynamics and fetal membrane rupture. Reprod Sci. 2013;20(2):140-153. doi:10.1177/1933719111424454
-
Minamitani T, Ariga H, Matsumoto K. Deficiency of tenascin-X causes a decrease in the level of expression of type VI collagen. Exp Cell Res. 2004;297(1):49-60. doi:10.1016/j.yexcr.2004.03.002
-
Egging DF, Van Vlijmen-Willems I, Choi J, et al. Analysis of obstetric complications and uterine connective tissue in tenascin-X-deficient humans and mice. Cell Tissue Res. 2008;332(3):523-532. doi:10.1007/s00441-008-0591-y
-
Morano D, Berto S, Lapucci C, Walczer Baldinazzo L, Prandstraller D, Farina A. Levels of circulating mRNA for the tenascin-X gene in maternal plasma at the second trimester in pregnancies with isolated congenital ventricular septal defects. Mol Diagn Ther. 2018;22(2):235-240. doi:10.1007/s40291-018-0321-4
-
Alcaraz LB, Exposito JY, Chuvin N, et al. Tenascin-X promotes epithelial-to-mesenchymal transition by activating latent TGF-β. J Cell Biol. 2014;205(3):409-428. doi:10.1083/jcb.201308031
-
Yener S, Demir T, Akinci B, et al. Transforming growth factor-beta 1 levels in women with prior history of gestational diabetes mellitus. Diabetes Res Clin Pract. 2007;76(2):193-198. doi:10.1016/j.diabres.2006.08.014
-
Morissette R, Merke DP, McDonnell NB. Transforming growth factor-β pathway abnormalities in tenascin-X deficiency associated with CAH-X syndrome. Eur J Med Genet. 2014;57(2-3):95-102. doi:10.1016/j.ejmg.2013.12.004
-
Liang G, Wang S, Shao J, et al. Tenascin-X mediates flow-induced suppression of EndMT and atherosclerosis. Circ Res. 2022;130(11):1647-1659. doi:10.1161/circresaha.121.320694
-
Zhou J, Ni X, Huang X, et al. Potential role of hyperglycemia in fetoplacental endothelial dysfunction in gestational diabetes mellitus. Cell Physiol Biochem. 2016;39(4):1317-1328. doi:10.1159/000447836
-
Troncoso F, Acurio J, Herlitz K, et al. Gestational diabetes mellitus is associated with increased promigratory activation of vascular endothelial growth factor receptor 2 and reduced expression of vascular endothelial growth factor receptor 1. PLoS One. 2017;12(8). doi:10.1371/journal.pone.0182509
-
Liang G, Lv XF, Huang W, et al. Loss of smooth muscle tenascin-X inhibits vascular remodeling through increased TGF-β signaling. Arterioscler Thromb Vasc Biol. 2024;44(8):1748-1763. doi:10.1161/atvbaha.123.321067
Figures

Figure 1. The ROC curve evaluating the role of amniotic fluid TNX in predicting adverse perinatal outcomes

Figure 2. The ROC curve evaluating the role of serum TNX in predicting adverse perinatal outcomes

Figure 3. The ROC curve comparing the role of amniotic fluid and serum TNX in predicting adverse perinatal outcomes
Tables
Table 1. The sociodemographic features and obstetric characteristics of adverse perinatal outcome and control groups
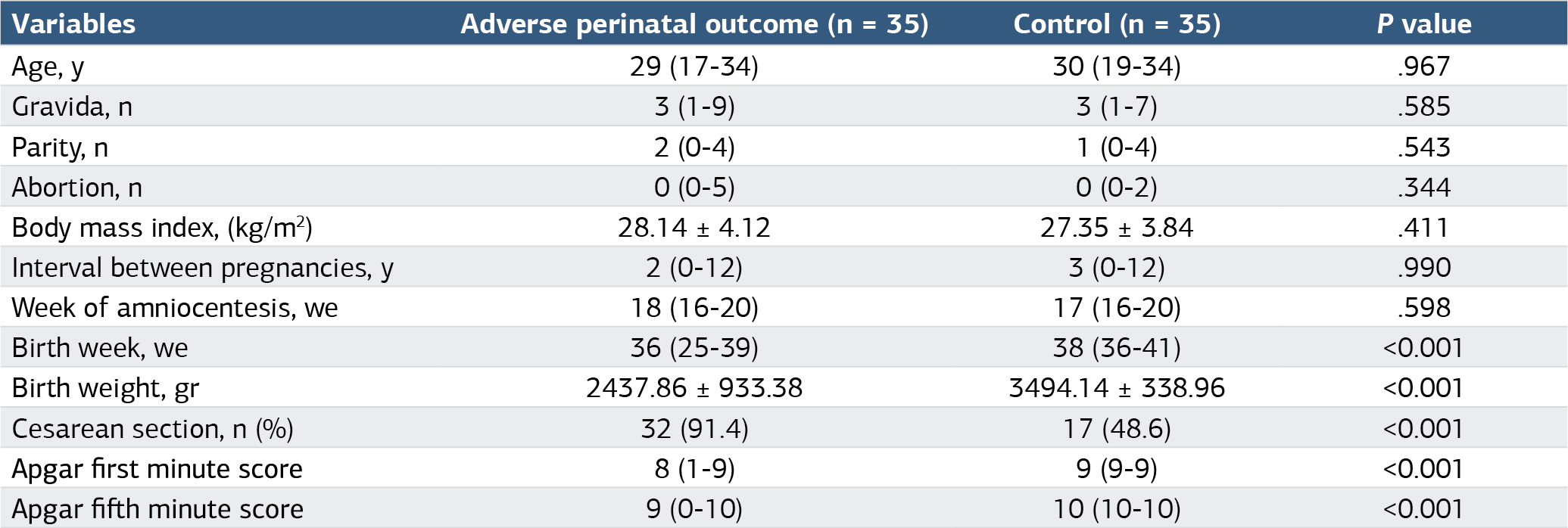
Table 2. The laboratory features of adverse perinatal outcome and control groups

ALT: alanine aminotransferase, AST: aspartate aminotransferase, aTNX: amniotic fluid tenascin X, sTNX: serum tenascin X, WBC: white blood cell
Table 3. Amniotic fluid and serum TNX levels for each adverse perinatal outcomes

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Begüm Uzsezer Güler, Burcu Dinçgez, Nefise Nazlı Yenigül, Gülten Özgen. The predictive role of amniotic fluid and serum tenascin X foradverse perinatal outcomes. Ann Clin Anal Med 2025;16(5):378-383. doi:10.4328/ACAM.22473
- Received:
- October 31, 2024
- Accepted:
- December 2, 2024
- Published Online:
- December 10, 2024
- Printed:
- May 1, 2025