
Screening and early detection of colorectal cancer in primary care: a systematic review
Screening of colorectal cancer in primary care
Authors
Abstract
Aim To enhance patient knowledge of colorectal cancer (CRC) risks, the advantages of early diagnosis, and the current screening techniques through educational programs implemented in primary care environments.
Methods A comprehensive search of relevant databases was conducted to identify studies meeting the inclusion criteria. An in-depth search of Web of Science, Science Direct, SCOPUS, and PubMed was conducted to find pertinent material.
Results Our data includes seven trials with 1,010,660 participants, and 429,418 (42.5%) were males. Retrospectively, trends in numerous full blood count (FBC) values, such as platelets, hemoglobin (HB), white blood cell count (WBC), and red blood cell (RBC) count, were statistically significant within the four years of diagnosing CRC. When a patient with lower-risk symptoms is presented to primary care (PC), a Fecal immunochemical test (FIT) is an extremely sensitive method for identifying the higher-risk patient. The frequency of positive i-FOBT (immunological fecal occult blood test) positive patients in PC is quite high.
Conclusion The systematic study emphasizes how important primary care physicians (PCPs) are to the early screening and diagnosis of colorectal cancer. Notwithstanding the difficulties encountered, a variety of tactics and measures can raise screening rates and better patient outcomes.
Keywords
Introduction
Among the main causes of illness and mortality in the West is CRC. In Europe, the 5-year survival rates for patients with colon and rectal cancer are 57% and 56%, respectively.1
The 5-year survival rates for patients with localized cancers are 92% and 90%, respectively, but the 5-year survival rates of patients with metastatic tumors are 13% and 18%, respectively (available at: https://www.cancer.org/cancer/types/colon- rectal-cancer/detection-diagnosis-staging.html). Because colorectal cancer patients tend to survive longer when the disease is discovered early, treating colorectal cancer early on is thought to enhance the overall prognosis of the patient.
Organized CRC screening programs have been demonstrated to lower CRC mortality and are utilized to recognize patients who are asymptomatic when the illness is most likely to be in its earliest stages.2,3 In addition to preventing CRC, screening makes it easier to remove adenomas and other polyps before they turn malignant.4 The practice of population-based CRC screening is well-established in numerous nations globally, with variations in the screening tests employed, time intervals, and eligibility criteria (including the USA, UK, and Australia).5 Participants in a biennial screening program in England and Wales are recruited between the ages of 60 and 74; in Scotland, the age range is smaller (50–74).6
To identify occult blood in asymptomatic people, the guaiac FOBT(Fecal occult blood test) was recently replaced in the UK by the FIT (available at: https://www.nice.org.uk/ guidance/ dg30). Compared to FOBT, FIT offers several benefits, such as enhanced sensitivity and specificity, improved sensitivity for identifying advanced adenomas, and the need for only one stool sample.
The capacity of CRC screening to detect adenomatous polyps, which can be excised to stop the development of cancer, emphasizes the significance of this procedure. The benefits of CRC screening have been demonstrated, yet participation rates are still below ideal. The low screening adoption can be attributed to many barriers, including cultural attitudes, lack of understanding, and restricted access to healthcare services. As a result, primary care physicians are strategically positioned to inform, encourage, and assist patients as they go through the screening process, guaranteeing increased compliance rates and prompt follow-up with aberrant results. The current systematic review aims to explore the screening and early detection methods of CRC in primary healthcare (PHC) centers.
Study Objectives• To enhance patient knowledge of colorectal cancer risks, the advantages of early diagnosis, and the current screening techniques through educational programs implemented in primary care environments.
• To guarantee that all patients have fair access to the tests they require—whether via in-office testing, referrals, or collaborations with specialized centers—barriers to CRC screening must be identified and addressed.
• To continuously assess the effectiveness of CRC screening initiatives in primary care, using metrics such as screening rates, follow-up compliance, and patient outcomes to drive ongoing improvements.
Materials and Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) were followed in the conduct of this systematic review 7 standards. Using databases including Scopus, PubMed, Web of Science, and Science Direct, an automated search was undertaken to find research articles written in English. In these situations, the search process employed pertinent keywords. To determine how strong the included study is, two reviewers independently went through the search results, selected pertinent papers, gathered information, and applied the proper assessment processes.
Eligibility Criteria
Inclusion Criteria
• Studies Written in English
• Studies investigating the screening methods and early detection of CRC in primary healthcare centers.
• RCTs (randomized control trials), cross-sectional, and observational studies (case-control & cohort) were included.
Exclusion Criteria
• Studies do not report the screening methods and investigating tools used for detecting CRC.
• Studies with limited methodological quality (e.g., case reports, opinion pieces).
• Studies in languages other than English or Arabic.
Data ExtractionTo ensure the accuracy and trustworthiness of our findings, the search results for the systematic review were rigorously reviewed using the Rayyan platform (QCRI).8 The titles and abstracts received throughout the search process were evaluated for their relevancy and consistency with the defined inclusion and exclusion criteria. The research team carefully and meticulously reviewed all papers that satisfied the inclusion criteria to extract relevant data. In instances where discrepancies arise during the evaluation process, these were resolved through a consensus among the reviewers, ensuring that the assessment is both fair and comprehensive. Key information from each study, including titles, authors, publication year, study location, demographic details of participants, gender distribution, screening methods, interventional diagnostic tool, and the main outcomes, were systematically recorded using a predetermined data extraction form. Furthermore, to appraise the methodological rigor of the included papers, we created a separate evaluation tool that aims to measure the degree of bias and the overall caliber of the research.
Data Synthesis StrategyOnce data extraction was complete, a qualitative analysis was conducted. This involved summary tables: creating tables to systematically organize and present the extracted data from all included studies. This allowed for easy comparison across studies and identification of common themes. Determining the Optimal Approach: depending on the nature of the data extracted.
Risk of Bias AssessmentTo ensure the validity and dependability of the involved studies, a standardized tool was utilized to guarantee each study’s methodological quality. This study employed the critical appraisal criteria for prevalence studies established by the Joanna Briggs Institute (JBI).9 This checklist consists of nine key questions that evaluate various aspects of a study’s design and execution, such as participant selection, data collection methods, and handling of confounding factors. For each question, a score of 1 was assigned for a “Yes” answer, indicating good methodological practice. Scores of 0 were given for “No,” “Unclear,” or irrelevant responses. The total score for each study was used to categorize its quality as follows: low risk of bias (score eight or above), moderate risk of bias (score 5-7), and high risk of bias (score below 4). Researchers independently assessed the quality of each study using the JBI tool. Any disagreements in scoring were resolved through discussion to ensure consistency in the quality assessment process.
Ethical ApprovalNot applicable. This systematic review did not involve human participants or animals, and no new data were collected.
Statistical AnalysisNot applicable. No meta-analysis or additional statistical analyses were performed; findings were synthesized descriptively from the included studies.
Reporting GuidelinesThis systematic review was conducted and reported in accordance with the PRISMA 2020 statement.
Results
Results of Systematic SearchA comprehensive search produced 948 study papers after 411 duplicates were removed.
After examining the titles and abstracts of 537 investigations, 442 manuscripts were rejected. Only three articles were not identified out of 95. After going through the full-text screening process, 92 papers were approved; 57 were rejected because of incorrect findings, 23 because the population was unsuitable, 2 were editor’s letters, and 3 were abstracts. Our eligibility criteria were satisfied by seven research articles that were utilized in this systematic review, as in Figure 1.
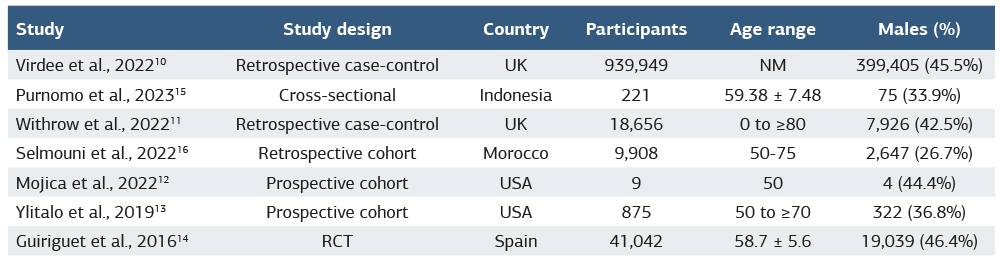
Sociodemographic Characteristics of the ParticipantsTable 1 illustrates the socio-demographic backgrounds of the research articles. Our data includes seven studies with 1,010,660 participants, and 429,418 (42.5%) were males. Two studies were retrospective case-control 10,11, two were prospective cohorts 12,13, one was an RCT14, and one was a cross-sectional study.15 Two studies were conducted in the UK,10,11 two in the USA,12,13 one in Indonesia,15 one in Morocco,16 and one in Spain.14 The initial study was carried out in 2016 14 and the most recent in 2023.15
Clinical OutcomesThe clinical data are shown in Table 2. Retrospective assessment of CRC screening using FBC results and FITs was discussed in three studies.10,11,16 Trends in numerous FBC values, such as RBC count, HB, WBC count, and platelets, were statistically significant within the four years of diagnosing CRC.10 When a patient with lower-risk symptoms presents to primary care, FIT is an extremely sensitive method for identifying the higher-risk patient.11,16
Four studies discussed prospective interventional screening methods using I-FOBT, colonoscopy, and FITs for the early detection of CRC.12,13,14,15 The frequency of I-FOBT-positive patients in primary care is quite high. CRC screening conducted as part of primary healthcare is increasing public involvement rates.12,13,14,15 Improving cancer screening rates in underserved patient communities may require an understanding of the obstacles and enablers of FITs/ FOBT.13
Discussion
Because most CRCs grow gradually, according to the Adenoma-Carcinoma sequence, screening can help lower the death rate from CRCs by identifying and eliminating precancerous lesions or early cancer diagnosis and removal.17,18 Stool-based imaging and endoscopic examinations are the three main types of CRC screening testing. Imaging and endoscopic tests can further lower the prevalence of colorectal cancer by identifying precancerous lesions, even as stool-based diagnostics can lower death rates by early detection of asymptomatic cancerous tumors.19
This review included retrospective assessments and prospective interventional screening to enhance the early detection of CRC. Retrospectively, we found that trends in numerous FBC values, such as WBC count, RBC count, HB, and platelets, were statistically significant within the four years of diagnosing CRC10 When a patient with lower-risk symptoms presents to primary care, FIT is an extremely sensitive method for identifying the higher-risk patient,.11,16 Virdee et al. included 53 papers evaluating the FBC blood test for colorectal cancer diagnosis found in a recent systematic review by.20 In comparison to patients who were not diagnosed, this research showed that within 6 months of diagnosis, diagnosed patients had considerably greater WBC cell count, platelets, RBC count, and HB. Less significant variations were found when compared to observations made more than six months before diagnosis, indicating that FBC changes with time. Patients with a diagnosis may be identified with the use of pertinent trends.20,21
Prospectively, we found that the frequency of I-FOBT-positive patients in primary care is quite high. This study demonstrates that CRC screening conducted as part of primary healthcare is increasing public involvement rates.12,13,14,15 Improving cancer screening rates in underserved communities may require an understanding of the obstacles and enablers of FITs/ FOBT.13 To identify occult blood in asymptomatic people, the FIT was just launched in the UK, taking the place of the guaiac FOBT (available at: https://www.nice.org.uk). FIT is superior to guaiac FOBT in several ways, such as enhanced sensitivity and specificity, improved sensitivity for identifying advanced adenomas, and the need for only one stool sample. Non-steroidal anti-inflammatory medications and anticoagulants do not affect the results of FIT, which is specific to human hemoglobin and does not need dietary restrictions.22,23 Screening participation is also increased when FIT is used in place of guaiac FOBT.24,25
Clinical ImplicationsThe results highlight the fact that participation rates are still below ideal even though screening has been demonstrated to be effective in lowering CRC mortality. This problem is caused by a number of things, including patient-related obstacles like ignorance, fear, and cultural preconceptions that restrict access to medical care. Implementation of screening is also hampered by provider-related issues such as lack of resources, inadequate training, and time constraints.
The analysis shows that two important tactics for raising screening uptake are patient education and tailored communication. Research has demonstrated that patient engagement in colorectal cancer screening programs is greatly increased by reminder systems, culturally sensitive communication, and customized educational interventions. Moreover, tracking screening status and sending automated reminders through the integration of electronic health records has been effective in raising screening rates.
Because primary care settings are easily accessible and PCPs maintain continuous relationships with their patients, they present a special opportunity to increase CRC screening rates. By making use of these connections, PCPs may be extremely helpful in encouraging patients to get screened, listening to their worries, and making sure that abnormal results are followed up on.
Future DirectionsSubsequent initiatives ought to concentrate on giving PCPs thorough training on risk assessment, communication techniques, and CRC screening procedures. They will be better equipped to inform and inspire their patients as a result. Innovative technologies, including machine learning (ML) and artificial intelligence (AI), are examples of cutting-edge technology that can be used to detect high-risk patients and forecast non-compliance, enabling focused interventions. Expanding access to CRC screening can also be facilitated by telemedicine, particularly in underprivileged areas.
Limitations
This review is limited by the small number of included studies, heterogeneity in study designs, and potential publication bias.
Conclusion
This systematic review emphasizes how important PCPs are to the early screening and diagnosis of colorectal cancer. Notwithstanding the difficulties encountered, a variety of tactics and measures can raise screening rates and better patient outcomes. Primary care facilities have the potential to make a substantial contribution to the early identification of colorectal cancer and, eventually, lower its incidence and fatality rate by concentrating on patient education, utilizing technology, and tackling systemic impediments. Further investigation into non-invasive and economical screening techniques, like blood- and stool-based biomarkers, can provide patients with more options and possibly boost screening rates.
Declarations
Ethics Declarations
Not applicable. No ethical approval or informed consent was required because this study synthesized findings from previously published literature only.
Animal and Human Rights Statement
Not applicable. No human or animal subjects were involved, and no interventions or procedures were performed. No new data were generated or analyzed in this systematic review; therefore, data sharing is not applicable
Informed Consent
Not applicable. This study did not involve human participants and used only data from published literature.
Data Availability
No new data were generated or analyzed in this systematic review; therefore, data sharing is not applicable.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: H.C.G.
Methodology: H.C.G., A.D.S.
Data curation: H.C.G.
Formal analysis: H.C.G.
Writing – original draft: H.C.G.
Writing – review & editing: H.C.G., A.D.S.
Supervision: A.D.S.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
CRC: Colorectal cancer
FBC: Full blood count
FIT: Fecal immunochemical test
FOBT: Fecal occult blood test
JBI: Joanna Briggs Institute
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
RCT: Randomized controlled trial
References
-
Holleczek B, Rossi S, Domenic A, et al. On-going improvement and persistent differences in the survival for patients with colon and rectum cancer across Europe 1999–2007–results from the EUROCARE-5 study. Eur J Cancer. 2015;51(15):2158-2168.
-
Zauber AG. The impact of screening on colorectal cancer mortality and incidence: Has it really made a difference? Dig Dis Sci. 2015;60(3):681-691.
-
Logan RF, Patnick J, Nickerson C, Coleman L, Rutter MD, von Wagner C. Outcomes of the Bowel Cancer Screening Programme (BCSP) in England after the first 1 million tests. Gut. 2012;61(10):1439-1446.
-
Geneve N, Kairys D, Bean B, Provost T, Mathew R, Taheri N. Colorectal Cancer Screening. Prim Care. 2019;46(1):135-148.
-
Young GP, Rabeneck L, Winawer SJ. The Global Paradigm Shift in Screening for Colorectal Cancer. Gastroenterology. 2019;156(4):843-51 e2.
-
Koo S, Neilson LJ, Von Wagner C, Rees CJ. The NHS Bowel Cancer Screening Program: current perspectives on strategies for improvement. Risk Manag Healthc Policy. 2017;10:177-187.
-
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
-
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210.
-
Munn Z, Aromataris E, Tufanaru C, et al. The development of software to support multiple systematic review types: The Joanna Briggs Institute System for the Unified Management, Assessment and Review of Information (JBI SUMARI). JBI evidence implementation. 2019;17(1):36-43.
-
Virdee PS, Patnick J, Watkinson P, Birks J, Holt TA. Trends in the full blood count blood test and colorectal cancer detection: A longitudinal, case-control study of UK primary care patient data. NIHR Open Res. 2022;2:32.
-
Withrow DR, Shine B, Oke J, et al. Combining faecal immunochemical testing with blood test results for colorectal cancer risk stratification: a consecutive cohort of 16,604 patients presenting to primary care. BMC Med. 2022;20(1):116.
-
Mojica CM, Gunn R, Pham R, et al. An observational study of workflows to support fecal testing for colorectal cancer screening in primary care practices serving Medicaid enrollees. BMC cancer. 2022;22(1):106.
-
Ylitalo KR, Camp BG, Umstattd Meyer MR, et al. Barriers and Facilitators of Colorectal Cancer Screening in a Federally Qualified Health Center (FQHC). J Am Board Fam Med. 2019;32(2):180-190.
-
Guiriguet C, Muñoz-Ortiz L, Burón A, et al. Alerts in electronic medical records to promote a colorectal cancer screening programme: a cluster randomised controlled trial in primary care. Br J Gen Pract. 2016;66(648):e483-e90.
-
Purnomo HD, Permatadewi CO, Prasetyo A, et al. Colorectal cancer screening in Semarang, Indonesia: A multicenter primary health care based study. PLoS One. 2023;18(1):e0279570.
-
Selmouni F, Amrani L, Sauvaget C, et al. Delivering colorectal cancer screening integrated with primary health care services in Morocco: Lessons learned from a demonstration project. Cancer. 2022;128(6):1219-1229.
-
De Leon MP, Percesepe A. Pathogenesis of colorectal cancer. Digestive and Liver Disease. 2000;32(9):807-821.
-
Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell. 1990;61(5):759-767.
-
Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med. 1993;329(27):1977-1981.
-
Virdee PS, Marian IR, Mansouri A, et al. The Full Blood Count Blood Test for Colorectal Cancer Detection: A Systematic Review, Meta-Analysis, and Critical Appraisal. Cancers (Basel). 2020;12(9):2348.
-
Virdee PS, Kirtley S, Elhussein L, Watkinson PJ, Holt TA, Birks J. Components of the full blood count as risk factors for colorectal cancer detection: a systematic review protocol. BMJ Open. 2019;9(12):e032759.
-
Nieuwenburg SAV, Vuik FER, Kruip M, Kuipers EJ, Spaander MCW. Effect of anticoagulants and NSAIDs on accuracy of faecal immunochemical tests (FITs) in colorectal cancer screening: A systematic review and meta-analysis. Gut. 2019;68(5):866-872.
-
Steele RJC. Overview of colorectal cancer screening. Colorectal Dis. 2019;21 Suppl 1(S1):14-15.
-
Vart G, Banzi R, Minozzi S. Comparing participation rates between immunochemical and guaiac faecal occult blood tests: a systematic review and meta-analysis. Prev Med. 2012;55(2):87-92.
-
Clark G, Strachan JA, Carey FA, et al. Transition to quantitative faecal immunochemical testing from guaiac faecal occult blood testing in a fully rolled- out population-based national bowel screening programme. Gut. 2021;70(1):106- 113.
Figures
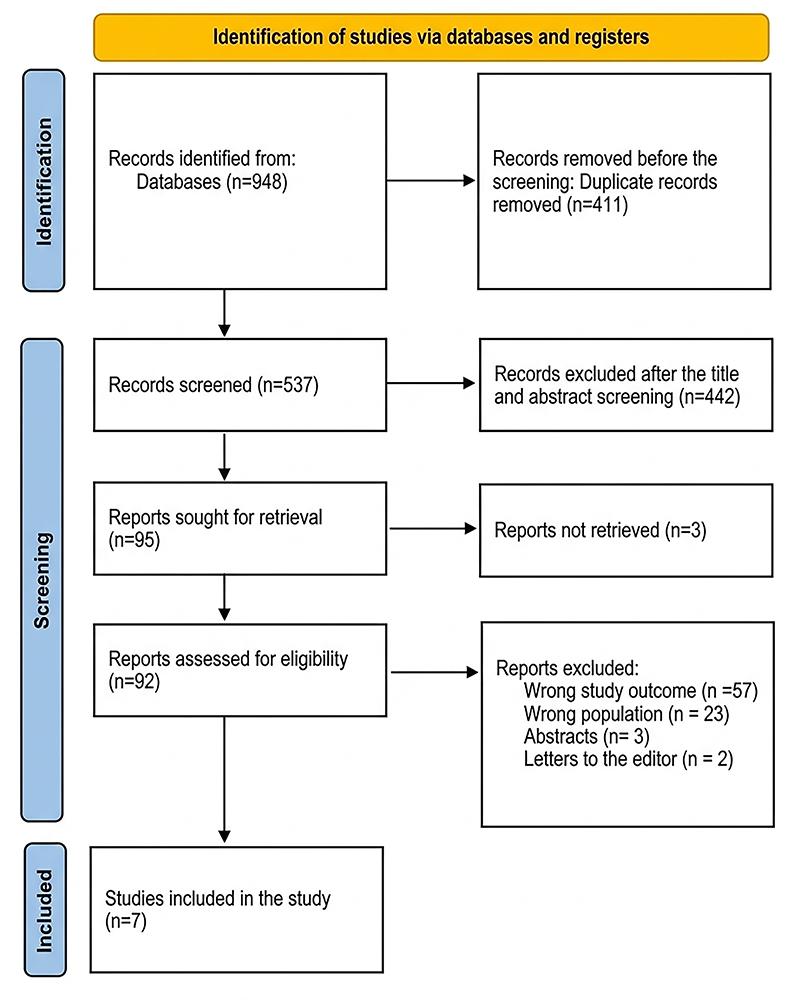
Figure 1. A PRISMA chart used to summarize the choices made during the study
Tables
Table 1. Sociodemographic backgrounds of the included participants
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mohamed M. Abd El-Mawgod, Faisal Saud m. Alenezi, Abdulmohsen Moharab Brik Alrawili, Basil Muteb Obaid Alanzi, Yasser Abdurrahman O Alhadhari, Rasil Naif M Alanazi, Abdullah Janab Alruwaili. Screening and early detection of colorectal cancer in primary care: a systematic review. Ann Clin Anal Med 2026;17(Suppl 2):S200-205. doi: 10.4328/ACAM.22486
- Received:
- November 15, 2024
- Accepted:
- December 16, 2024
- Published Online:
- December 29, 2024
- Printed:
- March 20, 2026