
Oxidative stress in pediatric patients: mechanisms, implications and therapeutic approaches
Oksidative stress in pediatric patients
Authors
Abstract
Oxidative stress (OS), defined as an imbalance between reactive oxygen species (ROS) and the body’s antioxidant defense systems, plays a significant role in the pathophysiology of various pediatric diseases. Reactive oxygen species are generated both endogenously through cellular metabolism and exogenously from environmental factors such as pollutants and radiation. While OS is essential for physiological processes, its dysregulation can contribute to tissue damage, cellular aging, and disease development. In children, OS is implicated in a wide range of conditions, including metabolic disorders like cystic fibrosis and type 1 diabetes, neurodevelopmental disorders such as autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD), respiratory diseases like asthma and cardiovascular conditions including congenital heart disease.
This review examines the mechanisms of OS in pediatric populations and highlights its role in disease progression. In particular, we discuss how ROS con- tributes to the pathogenesis of respiratory, neurodevelopmental, metabolic, gastrointestinal, and inflammatory diseases. For example, children with asthma experience increased OS, exacerbating airway inflammation, while those with cystic fibrosis suffer from chronic ROS-mediated lung damage. In neurodevel-opmental conditions like ASD and ADHD, OS disrupts normal neuronal function, potentially contributing to cognitive and behavioral impairments. Additionally, OS is a major factor in pediatric gastrointestinal disorders such as necrotizing enterocolitis and food allergies, where imbalances in antioxidant defenses are commonly observed. The paper also explores the potential for antioxidant therapies to mitigate OS-related damage in pediatric diseases.
Keywords
Introduction
The term oxidative stress (OS) was first introduced by Sies in 1985 1. OS occurs when there is an imbalance between reactive oxygen species (ROS) and antioxidants, with the balance tipping in favor of ROS production 2. Reactive oxygen species have both endogenous and exogenous sources. Endogenous ROS are produced from molecular oxygen during cellular metabolism, enzymatic oxidation, or inflammatory processes. Exogenous sources include radiation, certain drugs (such as chemotherapeutic agents), metal ions, asbestos, quartz, silica, exhaust gases, and cigarette smoke 3. Antioxidants are divided into enzymatic and non-enzymatic types; examples of non- enzymatic antioxidants include vitamins A, C, and E, flavonoids, procyanidins, β-carotene, and glutathione (GSH), while enzymatic antioxidants include superoxide dismutase (SOD), catalase (CAT), heme oxygenase-1, peroxiredoxins, thioredoxins, and glutaredoxins 4. Reactive oxygen species play roles in regulating intracellular calcium levels, protein phosphorylation and dephosphorylation, and pathogen destruction 5.
In children, OS has been linked to metabolic disorders such as cystic fibrosis, type 1 diabetes mellitus, obesity, and chronic renal failure, as well as psychiatric conditions like autism, psychosis, and schizophrenia. Cardiovascular diseases, including congenital heart failure and Kawasaki disease, which have inflammatory components, are also associated with OS. Numerous studies have been conducted on the role of OS in various pediatric conditions, including nutrition, the comparative effects of antiepileptic drugs on cellular damage in childhood epilepsy, enuresis, asthma, rickets, immunodeficiencies, neonatal disorders like necrotizing enterocolitis, retinopathy of prematurity, and the impact of sports activities. Results suggest that OS significantly affects children’s metabolism 6,7,8,9,10,11,12.
In this study, we aimed to explore the role of OS in the pathogenesis of childhood diseases by reviewing research that examines OS biomarkers in pediatric conditions.
Materials and Methods
The studies obtained as a result of the current literature review consist of intervention studies such as case-control, case series, and revisions. We applied the Preferred Reporting Items for Screening Meta-Analyses in our study 13. English publications made in the last 15 years using the keywords ‘’oxidative stress, pediatric patients, children’’ were examined via the PUBMED, Scopus, and Elsvier scientific databases. Approximately 30 studies conducted with patients under the age of 18, which were suitable for the disease groups in our article, were included.
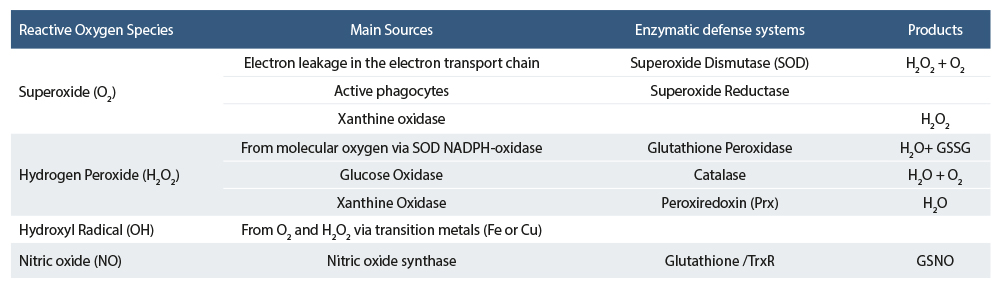
MechanismMitochondria are the primary endogenous source of ROS. Molecular oxygen is reduced to water in the electron transport chain, but 2-3% of oxygen is converted to ROS instead of water. When oxygen gains one electron, a superoxide radical is formed; with two electrons, hydrogen peroxide is produced, and with three electrons, a reactive hydroxyl radical is created. To mitigate the toxicity of these ROS, antioxidant enzymes like SOD, glutathione peroxidase (GPx), glutathione reductase, glutathione S-transferase (GST), CAT, thioredoxin reductase, peroxiredoxins (Prx), and NAD(P)H: ubiquinone oxidoreductase (NQO1) become active (Table 1). When the capacity of the antioxidant system is overwhelmed, ROS levels rise 14. The imbalance between ROS and antioxidant systems leads to cellular stress, resulting in lipid peroxidation, protein and carbohydrate degradation, oxygen inactivation, and DNA damage, causing cellular aging, disease, and cancer 15.
OS is understood as the disruption of the balance between ROS and antioxidants, tipping in favor of ROS. In adults, OS often results from weakened antioxidant systems and increased ROS, leading to cellular aging and disease. In children, OS tends to arise due to the genetic and metabolic foundations of childhood diseases, which make their cellular environments prone to inflammation and increased ROS production. For example, studies have shown excessive ROS production in diabetes mellitus associated with cystic fibrosis, leading to damage in pancreatic beta cells 16. In sickle cell anemia, the sickle- shaped red blood cells produce more ROS than healthy red cells 17. Autism spectrum disorder is linked to mitochondrial abnormalities that reduce ATP synthesis and increase ROS production, accompanied by an increased antioxidant response, leading to OS 18. Furthermore, infants born to mothers who consumed alcohol during pregnancy exhibit elevated ROS levels in the neonatal period, leading to metabolic and neurocognitive disorders in childhood 19.
Although numerous mechanisms explaining OS have been proposed, no specific mechanism has been conclusively identified in children. Since OS frequently occurs in the context of genetic and metabolic diseases in children, the mechanisms involved are complex and multifaceted. To better understand OS in children, individualized studies for each disease are necessary.
Results
The Role of Oxidative Stress in Pediatric DiseasesRespiratory DiseasesA study comparing children with allergic rhinitis to healthy controls found that OS index levels were higher and absolute eosinophil counts were significantly elevated in children with allergic rhinitis 20. Asthma, a common reason for pediatric emergency visits and school absences, is influenced by OS, which regulates the inflammatory response. Dietary intake of antioxidants such as zinc can enhance treatment efficacy, while an increase in oxidative substances or a reduction in antioxidant intake can worsen asthma severity 21. Low temperatures have been shown to increase OS in pediatric asthma patients, both in the nasal cavity and in the circulatory system, inducing asthma symptoms 22. Poorly controlled asthma in children exposed to exhaust fumes exacerbates OS and reduces lung capacity 23. Premature neonates, due to their increased ROS load and underdeveloped antioxidant mechanisms, are prone to oxidative damage, which can progress to chronic conditions such as bronchopulmonary dysplasia 24. Cystic fibrosis, an autosomal recessive genetic disorder, is characterized by mutations in the cystic fibrosis transmembrane regulator (CFTR) gene, which impairs chloride ion transport and affects organs such as the lungs and pancreas 25. In cystic fibrosis, chronic airway inflammation leads to excessive ROS production by neutrophils and macrophages, causing cell damage 26. Additionally, CFTR mutations disrupt ion balance, increase intracellular calcium, reduce GSH levels, and impair antioxidant defenses 25. Iron accumulation also contributes to OS in cystic fibrosis patients 27.
When Mycobacterium tuberculosis is inhaled, it is phagocytized by antigen-presenting cells in the lungs, leading to inflammation. Reactive oxygen species and reactive nitrogen products are released to eliminate the bacillus. Although the increase in free radicals is part of the defense mechanism, it can harm the host. A study in 2014 compared OS and paraoxonase-1 (PON-1) levels in 40 children with tuberculosis and 40 healthy children. In pulmonary tuberculosis patients, total oxidative status (TOS) and OSI levels were higher, while total antioxidant status (TAS) and PON-1 levels were lower than in the control group, indicating greater OS in pulmonary tuberculosis patients 28. In children with adenoid hypertrophy or obesity, the narrowing of the upper airway increases resistance, causing pharyngeal collapse and reduced airflow, leading to hypoxemia, hypercapnia, and short arousals from sleep. The hypoxia and reoxygenation cycles that occur during airway blockage and breathing resumption trigger systemic OS and inflammation. In pediatric obstructive sleep apnea syndrome, increased leukotriene activity, an inflammatory and OS biomarker, has been observed in both the airway and pharyngeal lymphoid tissue 29.
Neurodevelopmental DisordersAtaxia-telangiectasia, an autosomal recessive neurodevelopmental disorder characterized by cerebellar degeneration, oculocutaneous telangiectasias, immune deficiency, and susceptibility to malignancies, is associated with OS. Inflammatory markers such as IL-6 and IL-8, elevated in these patients, suggest OS may contribute to disease progression 30. Autism spectrum disorder, a neurodevelopmental condition influenced by both genetic and environmental factors, is also associated with increased OS due to impaired antioxidant systems, particularly in the temporal cortex and cerebellum 31,32. Autism spectrum disorder is a neuropsychiatric disorder characterized by repetitive behaviors, impaired social communication skills, and restricted interests. Although genetic and environmental factors cause ASD, its pathophysiology is still unclear. Since there is no reliable marker for diagnosis, it is quite difficult to diagnose in patients under 2 years of age. Although OS is not diagnostic, it has an important place in the pathophysiology of ASD. Since brain tissue uses almost 20% of the oxygen in the body, the amount of ROS production is higher than other tissues, and therefore it is more sensitive to OS. In a postmortem study conducted in 2012 with ASD patients, it was shown that reduced GSH, oxidized glutathione (GSSG), and glutathione redox/antioxidant capacity (GSH/GSSG), which are peripheral markers of ASD, were significantly reduced in the cerebellum and temporal cortex of the brain, and it was concluded that there was a serious relationship between ASD and OS 33. Attention-deficit/hyperactivity disorder (ADHD) is another neurodevelopmental disorder linked to OS, with increased ROS production and reduced antioxidant defenses contributing to the pathophysiology of 34.
Oxidative stress is an important factor, alongside genetic, neurobiological, psychological, and neurochemical factors, in the etiology of anxiety disorders in children and adolescents. The imbalance between oxidants and antioxidants leads to a biological condition where accumulated oxidants impact central nervous system-related pathologies, contributing to neuropsychiatric disorders. A 2014 study on children with and without anxiety disorders found that those with anxiety had higher OS indices and total oxidative levels than the control group, indicating a role for OS in anxiety disorder etiology 35. Simple febrile seizures are generally benign, but due to high glutamate levels and increased metabolic brain activity during a seizure, increased oxygen use can result in OS. Oxidative stress damages functional cells and can lead to cell death due to the oxidation of biomolecules such as proteins, lipids, and nucleotides. Changes in antioxidant levels and increased lipid peroxidation may contribute to neuronal damage during seizures. Increased ROS levels are both a cause and result of seizures. Thiol/disulfide homeostasis, a safe, cost-effective biomarker indicating excessive ROS production, plays a significant role in antioxidant defense, detoxification, signal transduction, enzyme activity, apoptosis, and central nervous system physiology. In febrile seizure patients, thiol/disulfide homeostasis is disrupted, contributing to seizure progression and recurrence, which can lead to neuronal damage 36.
Although the pathophysiological mechanism of epilepsy is not fully known, it is thought that Os plays a role in etiopathogenesis. Brain tissue is very sensitive to OS because it uses most of the oxygen entering the body. The resulting ROS affects signal transmission. In a study conducted to examine the effect of antiepileptic treatments on OS, it was shown that antiepileptic treatment increased OS 37.
Cardiac and Metabolic DiseasesChildren with congenital heart disease are more vulnerable to OS due to inadequate oxygen delivery to tissues 38. Acute rheumatic fever (ARF), a disease triggered by a Group B streptococcal infection, has been linked to OS. Studies show elevated levels of C-reactive protein (CRP), malondialdehyde (MDA), protein carbonyl (PCO), and cytokines in ARF patients, along with reduced TAS 39. Kawasaki disease, a vasculitis that affects coronary arteries in children under 5 years of age, is characterized by increased OS during its early phase due to the accumulation of ROS-producing neutrophils and macrophages in the coronary arteries 40. In a study conducted in 2019, oxidized low-density lipoprotein (ox-LDL)/lectin-like-oxLDL receptor-1 (LOX-1) levels were examined, and LOX-1 mRNA expression was significantly increased in Kawasaki patients, especially those with coronary artery lesions. LOX-1 level may be a biomarker indicating the risk of developing coronary artery lesions in Kawasaki patients 41.
OS has an important role in the pathophysiology of many cardiovascular diseases. The development and progression of heart failure in patients with congenital heart disease (CHD) is the most important cause of morbidity and mortality. Since oxygenation is lower in congenital heart diseases, especially in patients with cyanotic CHD, hypoxia causes an increase in ROS production in these patients. Therefore, these patients are more susceptible to OS. In a study conducted in Turkey in 2011, MDA, PCO, hs-CRP, fibrinogen, IL-6, and TNF-a levels were significantly higher in children with CHD compared to healthy children. The results showed that patients with CHD were more susceptible to OS and that PCO could be used as a biomarker 42.
Tetralogy of Fallot (TOF) is the most common form of cyanotic CHD. It is seen in 0.5 people per 1000 live births. TOF clinically causes frequent hypoxia attacks. These attacks produce large amounts of ROS. These attacks contribute to the formation of OS. To prove this contribution, in a study conducted with 47 CHD patients (24 TOF, 23 ventricular septal defect (VSD)) and 47 healthy children, thiol and NO levels of the participants were examined, and a significant decrease in the native thiol/ total thiol ratio was detected in TOF patients. No significant change was observed in this ratio in VSD patients. NO levels were significantly increased in VSD and TOF patients 43.
Gastrointestinal DisordersNecrotizing enterocolitis, a severe gastrointestinal disease in premature infants, is associated with rapid ROS production due to premature metabolic processes, exposure to 100% oxygen, and the presence of free iron 44. Studies on food allergies in children have shown reduced antioxidant levels, such as selenium and zinc, and decreased activity of antioxidant enzymes like GPx and SOD. Antioxidant levels improved after elimination diets, indicating a weakened antioxidant defense system in food allergies 45.
Celiac disease is an autoimmune disorder triggered by gluten sensitivity in the small intestine. The DNA sequence of gliadin, one of the proteins in gluten, exerts cytotoxic and immunomodulatory effects and triggers OS, causing pro- inflammatory cytokine release and mucosal damage. Both enzymatic and non-enzymatic antioxidants protect the body against ROS damage, but most non-enzymatic antioxidants are essential dietary components in celiac patients. Adherence to a strict gluten-free diet is crucial for maintaining oxidant- antioxidant balance in celiac disease 46.
Rheumatologic DisordersIn IgA vasculitis, when gastrointestinal involvement is the first clinical symptom, studies have shown increased DNA oxidation. During the active phase of the disease, IL-17 levels and TAS were found to be higher compared to remission, indicating that OS plays a significant role during disease exacerbation 47.
Systemic lupus erythematosus (SLE) is an autoimmune disease that involves multiple organs and systems. In SLE patients, immune cells are dysfunctional due to autoantigen production and autoantibody reactivity. In these patients, the evaluation of DNA, lipid, and protein markers damaged by OS helps determine the course of the disease, treatment response, severity, and prognosis. In a study conducted in Egypt in 2019 with 100 children diagnosed with SLE and 100 healthy controls, the participants’ MDA GST SOD TAS CAT levels were examined. It was determined that there was a significant increase in MDA and CAT levels and a significant decrease in SLE and GST levels in SLE patients. It was concluded that OS plays an important role in the pathogenesis of SLE 48.
Endocrine DisordersType 1 diabetes mellitus (T1DM) is an autoimmune disease caused by the destruction of pancreatic islet β-cells, resulting in insufficient insulin secretion. The primary treatment involves individually adjusted insulin doses to regulate glucose levels. Proper glycemic control affects the antioxidant system and prevents complications. Dietary intake of antioxidant nutrients is as important as metabolic and glycemic control in minimizing OS-related damage 49. To detect and prevent diabetic inflammation and complications early, many recent studies have focused on hemogram parameters. In a study investigating the relationship between hemogram parameters and OS in type 1 diabetes patients, findings revealed that inflammation and OS markers contributed to abnormalities in hemogram parameters. This suggests that certain hemogram parameters could serve as early indicators for diabetic complications 50.
Childhood obesity, affecting millions of children worldwide, is associated with metabolic syndrome and OS due to cytokine release, lipid hemostasis disruption, and reduced antioxidant defenses 38.
Urinary DiseasesNephron formation is generally completed between the 34th and 36th weeks of gestation. Preterm births often occur while nephrogenesis is still ongoing. Oxidative stress can damage the proximal tubules. The exposure of preterm newborns to high concentrations of oxygen at birth and afterward contributes to hypertension, a reduction in nephron numbers, and structural impairment in adulthood. Reactive oxygen species also increase extracellular matrix accumulation in tubular epithelial cells, mesangial cells, and the tubular interstitium and activate a profibrogenic cytokine, TGF-β, leading to fibrosis in kidney tissue 51.
Oxidative stress arises from the imbalance between ROS and antioxidants. In chronic renal failure, this stress is multifactorial, stemming from uremic toxins, incompatible dialyzers with mononuclear cells, contaminated dialysates, and infections, and is compounded by reduced antioxidant enzyme activities. Hemodialysis reduces hypoxia but increases antioxidant loss. The resulting OS can lead to long-term complications in uremic patients. As a compensatory mechanism, VEGF is produced to increase oxygen delivery to hypoxic tissue 52.
Hematologic DiseasesOxidative stress and alterations in thiol-disulfide balance are thought to play a role in the pathogenesis of idiopathic thrombocytopenic purpura (ITP). A 2021 study divided participants into three groups: acute ITP, chronic ITP, and a control group. The study analyzed TAS, TOS, oxidative stress index (OSI), and thiol-disulfide levels. Results showed increased OS in children with acute and chronic ITP, a thiol-disulfide imbalance favoring disulfide in acute ITP, and no imbalance in children with ITP who had normal platelet counts and did not require treatment 53.
Leukemias and lymphomas are among the most diagnosed and deadliest malignancies in children worldwide. Cellular OS in these patients is mainly related to cancer treatment and diet. Normally, OS promotes disease progression and DNA damage. However, in pediatric leukemia and lymphoma patients, OS increases the effectiveness of chemotherapeutic treatment. These drugs increase ROS levels, causing irreversible damage to cancer cells. Since cellular antioxidant balance can be regulated by diet, studies have been conducted to enhance treatment efficacy by monitoring the nutritional status of pediatric leukemia and lymphoma patients 54.
Iron deficiency anemia has also been associated with OS in patients experiencing breath-holding spells. Studies have shown that the oxidant/antioxidant balance is shifted toward oxidants in these patients 55.
NewbornNeonatal hyperbilirubinemia, affecting 8 to 11% of newborns during their first week of life, is a common condition that arises from the oxidative breakdown of red blood cells. A study on preterm neonates demonstrated that vitamin E supplementation, an antioxidant, significantly reduced serum bilirubin levels and increased total antioxidant capacity. This suggests that vitamin E supplementation can shorten the duration of phototherapy required for treating neonatal hyperbilirubinemia 56.
Since the antioxidant system in newborns is not yet developed, they are quite sensitive to OS. In a study conducted in 2023 with 28 newborns who received phototherapy with the diagnosis of neonatal hyperbilirubinemia, bilirubin, total and native thiol, TAS, TOS, and OSI levels of the patients were measured before and after phototherapy. It was found that native and total thiol levels, TAS, and TOS levels were significantly lower in infants after phototherapy. It was concluded that phototherapy reduces OS due to hyperbilirubinemia in newborns and that Thiol- disulfide homeostasis can be used as a marker of OS due to hyperbilirubinemia in the early period 7.
Fetal alveolar fluid fills the alveoli during the antenatal period and must be removed for gas exchange to occur at birth. Tachypnea is observed in newborns to tolerate late removal or inadequate absorption of this fluid. This condition is defined as transient tachypnea of the newborn (TTN). Increased respiratory workload triggers OS. Continuing Positive Airway Pressure (CPAP) treatment helps remove this fluid from the alveoli. In a study conducted in 2023, Thiol (natural and total) and disulfide levels, TAS, TOS, and OSI levels were measured before and after CPAP treatment in patients admitted to the neonatal intensive care unit with TTN. A significant decrease in disulfide levels was detected after CPAP treatment in the late preterm group. It was concluded that CPAP treatment reduced OS associated with TTN in newborns 8.
Bronchopulmonary dysplasia (BPD) is a chronic lung disease seen in premature newborns due to the negative effects on alveolar and pulmonary vascular development as a result of premature birth and subsequent processes. In premature infants, exposure to high oxygen pressure and volume as a result of respiratory support given to ventilate immature lung tissue damages lung tissue. Inflammation is triggered. Inflammation and the ROS that occur together trigger OS formation. In a study conducted to evaluate the level of OS and dynamic thiol-disulfide balance in patients with BPD, TAS, TOS, OSI, natural thiol (NT), and total thiol levels were measured in 2 groups of patients with and without BPD included in the study. Plasma TAS and NT levels measured in newborns with BPD were found to be significantly lower than in newborns without BPD. It was concluded that OS was high in newborns with BPD and affected them 9.
Parallel to the developments in newborn care, although the survival chance of low birth weight and premature babies has increased, the incidence of retinopathy of prematurity (ROP), which causes vision problems, is increasing. The retina is not fully vascularized in premature newborns; there are avascular areas. As a result of oxygen treatments after birth, abnormal vascularization occurs in avascular areas. ROP occurs as a result of bleeding in these abnormal vascularized areas. Since the risk of developing ROP increases in hyperoxia conditions, ROS production also increases in these patients. It is thought that these patients are quite sensitive to OS. In a study conducted with 129 premature newborns with a gestational age of <34 weeks, the Thiol (native and total), TAS, TOS, and OSI levels of the patients were examined. TAS levels were found to be lower in those with ROP compared to those without, while TOS and OSI levels were found to be significantly higher. It was concluded that ROP patients are quite sensitive to OS 10.
Other Related ConditionsHuman breast milk is the baby’s sole and primary source of nutrition in the first 6 months of life. Human breast milk plays a major role in the development of both the gastrointestinal system and the immune system. Human breast milk is rich in many antioxidant enzymes such as CAT, GPx, and SOD. These enzymes are not found in formula milk. It has previously been shown that there is a significant reduction in urinary markers of oxidative DNA damage in breastfed full-term and preterm infants compared to formula-fed infants 57.
Vitamin B12 has undertaken many important roles, such as neurotransmitter synthesis, DNA synthesis, and cognitive development. In vitamin B12 deficiency, permanent changes are likely to be seen in cognitive activities and neuronal and hematological systems. In vitamin B12 deficiency, GSH synthesis, which is an indicator of antioxidant capacity, decreases. Thus, ATP production decreases and ROS amount increases. In a case-control study conducted in 2023 with patients presenting with headache complaints, serum disulfide level was found to be higher in patients with vitamin B12 deficiency than in those without vitamin B12 deficiency, and it was concluded that OS plays an important role in vitamin B12 deficiency 6.
Vitamin D is a vitamin that affects calcium, phosphorus, and bone metabolism in the human body, as well as having antioxidant properties. In a study conducted in China in 2014 with 1488 pediatric patients, CRP, IL-6, MDA, and SOD levels were examined in 2 groups of patients with and without vitamin D deficiency, and SOD levels were found to be high in patients with vitamin D deficiency. It has been reported that high SOD levels are associated with OS 58.
Diagnostic Biomarkers of Oxidative Stress in Pediatric Patients
Oxidative stress plays a role in the pathophysiology of various diseases, from DNA oxidation to effects on lipids, free amino acids, and proteins. Many methods have been developed to study OS effects, with biomarkers of OS being among the most effective. However, due to its complex nature, finding and using a disease-specific biomarker is challenging. Main indicators of oxidative damage include MDA, a stable end-product of membrane lipid peroxidation, and 8-hydroxy-deoxyguanosine (8-OHdG). Antioxidant systems formed in response to oxidative damage are divided into enzymatic and non-enzymatic systems. Key enzymatic biomarkers include GPx, CAT, and SOD, while primary non-enzymatic biomarkers include uric acid and GSH 59. In our review, the biomarkers measured in the diseases mentioned are reported in Table 2.
Conclusion
Oxidative stress occurs as a result of the imbalance between the production of ROS and antioxidant mechanisms. In children who are in the growth and development period, due to the immaturity of antioxidant mechanisms, the excessive production of ROS and the immaturity of antioxidant mechanisms to balance this resulting in the imbalance in favor of the increase in ROS, resulting in OS. Although there are different mechanisms for each patient and disease, OS fundamentally plays an important role in childhood diseases. It has been concluded that the use of antioxidants in the treatment of these diseases contributes to the reduction of damage caused by OS.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
References
-
Sies H, Cadenas E. Oxidative stress: Damage to intact cells and organs. Philos Trans R Soc Lond B Biol Sci. 1985;311(1152):617-31. doi:10.1098/rstb.1985.0168.
-
Micangeli G, Menghi M, Profeta G, et al. The impact of oxidative stress on pediatrics syndromes. Antioxidants (Basel). 2022;11(10):1983. doi:10.3390/antiox11101983.
-
Jesenak M, Zelieskova M, Babusikova E. Oxidative stress and bronchial asthma in children-causes or consequences? Front Pediatr. 2017;5:162. doi:10.3389/fped.2017.00162.
-
Vincenzo SD, Ferrante G, Ferraro M, et al. Oxidative stress, environmental pollution, and lifestyle as determinants of asthma in children. Biology (Basel). 2023;12(1):133. doi:10.3390/biology12010133.
-
Sies H, Jones DP. Reactive oxygen species (ROS) as pleiotropic physiological signalling agents. Nat Rev Mol Cell Biol. 2020;21(7):363-83. doi:10.1038/s41580-020-0230-3.
-
Demirtas MS, Erdal H. Evaluation of thiol disulfide balance in adolescents with vitamin B12 deficiency. Ital J Pediatr. 2023;49(1):3. doi:10.1186/s13052-022-01396-2.
-
Demirtas MS, Erdal H. Evaluation of thiol-disulfide homeostasis and oxidative stress parameters in newborns receiving phototherapy. J Investig Med. 2023;71(3):183-90. doi:10.1177/10815589221140594.
-
Demirtas MS, Erdal H, Kilicbay F, Tunc G. Association between thiol-disulfide hemostasis and transient tachypnea of the newborn in late-preterm and term infants. BMC Pediatr. 2023;23(1):135. doi:10.1186/s12887-023-03936-z.
-
Demirtas MS, Kilicbay F, Erdal H, Tunc G. Oxidative stress levels and dynamic thiol-disulfide balance in preterm newborns with bronchopulmonary dysplasia. Lab Med. 2023;54(6):587-92. doi:10.1093/labmed/lmad010.
-
Erdal H, Demirtas MS, Kilicbay F, Tunc G. Evaluation of oxidative stress levels and dynamic thiol-disulfide balance in patients with retinopathy of prematurity. Curr Eye Res. 2023;48(11):1026-33. doi:10.1080/02713683.2023.2185569.
-
Genc SO, Erdal H. Effect of mode of delivery on neonatal oxidative stress and dynamic thiol-disulfide homeostasis. J Int Med Res. 2023;51(10):3000605231202145. doi:10.1177/03000605231202145.
-
Erdal H, Bekmezci M. Evaluation of dynamic thiol/disulfide homeostasis and ischemia-modified-albumin levels in cord blood of newborns to patients with oxytocin-induced labor. Aksaray University J of S and H Res. 3(2):193-202. doi:10.54152/asujshr.1203106.
-
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. doi:10.1371/journal.pmed.1000100.
-
Casteilla L, Rigoulet M, Penicaud L. Mitochondrial ROS metabolism: modulation by uncoupling proteins. IUBMB Life. 2001;52(3-5):181-8. doi:10.1080/15216540152845984.
-
Yoshikawa T, You F. Oxidative stress and bio-regulation. Int J Mol Sci. 2024;25(6):3360. doi:10.3390/ijms25063360.
-
Pinzaru AD, Mihai CM, Chisnoiu T, et al. Oxidative stress biomarkers in cystic fibrosis and cystic fibrosis-related diabetes in children: a literature review. Biomedicines. 2023;11(10):2671. doi:10.3390/biomedicines11102671.
-
Silva M, Faustino P. From Stress to sick(le) and back again-oxidative/ antioxidant mechanisms, genetic modulation, and cerebrovascular disease in children with sickle cell anemia. Antioxidants (Basel). 2023;12(11):1977. doi:10.3390/antiox12111977.
-
Zhuang H, Liang Z, Ma G, et al. Autism spectrum disorder: pathogenesis, biomarker, and intervention therapy. MedComm (2020). 2024;5(3):e497. doi:10.1002/mco2.497.
-
Derme M, Briante M, Ceccanti M, et al. Prenatal alcohol exposure and metabolic disorders in pediatrics: the role of the oxidative stress-a review of the literature. Children (Basel). 2024;11(3):269. doi:10.3390/children11030269.
-
Danevska IA, Jakjovska T, Zendelovska D, et al. Comparison of oxidative stress levels in healthy children and children with allergic rhinitis. Pril (Makedon Akad Nauk Umet Odd Med Nauki). 2023;44(1):17-26. doi:10.2478/prilozi-2023-0003
-
He L, Norris C, Palaguachi-Lopez K, et al. Nasal oxidative stress mediating the effects of colder temperature exposure on pediatric asthma symptoms. Pediatr Res. 2024;96(4):1045-51. doi:10.1038/s41390-024-03196-2.
-
He L, Norris C, Palaguachi-Lopez K, et al. Nasal oxidative stress mediating the effects of colder temperature exposure on pediatric asthma symptoms. Pediatr Res. 2024;96(4):1045-51. doi:10.1038/s41390-024-03196-2.
-
Fitzpatrick AM, Mohammad AF, Desher K, et al. Clinical and inflammatory features of traffic-related diesel exposure in children with asthma. Ann Allergy Asthma Immunol. 2024;133(4):393-402e4. doi:10.1016/j.anai.2024.07.019.
-
Cannavo L, Perrone S, Viola V, Marseglia L, Di Rosa G, Gitto E. Oxidative stress and respiratory diseases in preterm newborns. Int J Mol Sci. 2021;22(22):12504. doi:10.3390/ijms222212504.
-
Moliteo E, Sciacca M, Palmeri A, et al. Cystic fibrosis and oxidative stress: the role of CFTR. Molecules. 2022;27(16):5324. doi:10.3390/molecules27165324.
-
Quinn MT, Gauss KA. Structure and regulation of the neutrophil respiratory burst oxidase: comparison with nonphagocyte oxidases. J Leukoc Biol. 2004;76(4):760-81. doi:10.1189/jlb.0404216.
-
Abe C, Miyazawa T, Miyazawa T. Current use of fenton reaction in drugs and food. Molecules. 2022;27(17):5451. doi:10.3390/molecules27175451.
-
Torun E, Gedik AH, Cakir E, Umutoglu T, Gok O, Kilic U. Serum paraoxonase 1 activity and oxidative stress in pediatric patients with pulmonary tuberculosis. Med Princ Pract. 2014;23(5):426-31. doi:10.1159/000363700.
-
Malakasioti G, Alexopoulos E, Befani C, et al. Oxidative stress and inflammatory markers in the exhaled breath condensate of children with OSA. Sleep Breath. 2012;16(3):703-8. doi:10.1007/s11325-011-0560-7.
-
McGrath-Morrow SA, Ndeh R, Collaco JM, et al. Inflammation and transcriptional responses of peripheral blood mononuclear cells in classic ataxia telangiectasia. PLoS One. 2018;13(12):e0209496. doi:10.1371/journal.pone.0209496.
-
Usui N, Kobayashi H, Shimada S. Neuroinflammation and oxidative stress in the pathogenesis of autism spectrum disorder. Int J Mol Sci. 2023;24(6):5487. doi:10.3390/ijms24065487.
-
Pangrazzi L, Balasco L, Bozzi Y. Oxidative stress and immune system dysfunction in autism spectrum disorders. Int J Mol Sci. 2020;21(9):3293. doi:10.3390/ijms21093293.
-
Rose S, Melnyk S, Pavliv O, et al. Evidence of oxidative damage and inflammation associated with low glutathione redox status in the autism brain. Transl Psychiatry. 2012;2(7):e134. doi:10.1038/tp.2012.61.
-
Corona JC. Role of oxidative stress and neuroinflammation in attention- deficit/hyperactivity disorder. Antioxidants (Basel). 2020;9(11):1039. doi:10.3390/antiox9111039.
-
Guney E, Fatih Ceylan M, Tektas A, et al. Oxidative stress in children and adolescents with anxiety disorders. J Affect Disord. 2014;156:62-6. doi:10.1016/j.jad.2013.11.016.
-
Elmas B, Erel O, Ersavas D, Yurumez Y. Thiol/disulfide homeostasis as a novel indicator of oxidative stress in children with simple febrile seizures. Neurol Sci. 2017;38(11):1969-75. doi:10.1007/s10072-017-3087-2.
-
Kopan DT, Ozcelik AA, Kopan MA, Taysi S. Assessment of oxidative/ nitrosative stress and antioxidant capacity in children with epilepsy. Int J Neurosci. 2024;134(6):652-7. doi:10.1080/00207454.2022.2140426.
-
Gonzalez-Dominguez A, Belmonte T, Gonzalez-Dominguez R. Childhood obesity, metabolic syndrome, and oxidative stress: microRNAs go on stage. Rev Endocr Metab Disord. 2023;24(6):1147-64. doi:10.1007/s11154-023-09834-0.
-
Gozu Pirinccioglu A, Alyan O, Akin A, Kizil G, Isik FB. Oxidative stress parameters in children with acute rheumatic fever. Pediatr Int. 2019;61(10):962-6. doi:10.1111/ped.13983.
-
Tsuge M, Uda K, Eitoku T, Matsumoto N, Yorifuji T, Tsukahara H. Roles of oxidative injury and nitric oxide system derangements in Kawasaki disease pathogenesis: a systematic review. Int J Mol Sci. 2023;24(20):15450. doi:10.3390/ijms242015450.
-
He YE, Qiu HX, Wu RZ, et al. Oxidised low-density lipoprotein and its receptor- mediated endothelial dysfunction are associated with coronary artery lesions in Kawasaki disease. J Cardiovasc Transl Res. 2020;13(2):204-14. doi:10.1007/s12265-019-09908-y.
-
Pirinccioglu AG, Alyan O, Kizil G, Kangin M, Beyazit N. Evaluation of oxidative stress in children with congenital heart defects. Pediatr Int. 2012;54(1):94-8. doi:10.1111/j.1442-200X.2011.03478.x.
-
Temel MT, Demiryürek S, Saracaloglu A, et al. Determination of dynamic thiol/ disulphide homeostasis in children with tetralogy of Fallot and ventricular septal defect. Cardiol Young. 2019;29(4):499-504. doi:10.1017/S104795111900012X.
-
Gershner GH, Hunter CJ. Redox chemistry: implications for necrotizing enterocolitis. Int J Mol Sci. 2024;25(15):8416. doi:10.3390/ijms25158416.
-
Kamer B, Wasowicz W, Pyziak K, Kamer-Bartosinska A, Gromadzinska J, Pasowska R. Role of selenium and zinc in the pathogenesis of food allergy in infants and young children. Arch Med Sci. 2012;8(6):1083-8. doi:10.5114/aoms.2012.32420.
-
Rowicka G, Czaja-Bulsa G, Chełchowska M, et al. Oxidative and antioxidative status of children with celiac disease treated with a gluten free-diet. Oxid Med Cell Longev. 2018;2018:1324820. doi:10.1155/2018/1324820.
-
Kisaoglu H, Misir S, Aliyazicioglu Y, Kalyoncu M. Interleukin -17 and oxidative stress in children with immunoglobulin A vasculitis. Scand J Rheumatol. 2022;51(4):309-14. doi:10.1080/03009742.2021.1926319.
-
Fouad H, Yahia S, Elsaid A, et al. Oxidative stress and vitamin D receptor BsmI gene polymorphism in Egyptian children with systemic lupus erythematosus: a single center study. Lupus. 2019;28(6):771-7. doi:10.1177/0961203319846380.
-
Grabia M, Socha K, Soroczynska J, Bossowski A, Markiewicz-Zukowska R. Determinants related to oxidative stress parameters in pediatric patients with type 1 diabetes mellitus. Nutrients. 2023;15(9):2084. doi:10.3390/nu15092084.
-
Abdel-Moneim A, Zanaty MI, El-Sayed A, Khalil RG, Rahman HA. Relation between oxidative stress and hematologic abnormalities in children with type 1 diabetes. Can J Diabetes. 2020;44(3):222-8. doi:10.1016/j.jcjd.2019.07.153.
-
Wang HH. Oxidative stress and potential renal damage in neonates. Pediatr Neonatol. 2015;56(4):209-10. doi:10.1016/j.pedneo.2015.03.003.
-
Hamed EA, El-Abaseri TB, Mohamed AO, Ahmed AR, El-Metwally TH. Hypoxia and oxidative stress markers in pediatric patients undergoing hemodialysis: cross section study. BMC Nephrol. 2012;13:136. doi:10.1186/1471-2369-13-136.
-
Kar YD, Ozdemir ZC, Bor O. Thiol / disulfide balance and oxidative stress parameters in pediatric patients diagnosed with acute and chronic idiopathic thrombocytopenic purpura. Turk J Pediatr. 2021;63(6):962-9. doi:10.24953/turkjped.2021.06.003.
-
Raber M, Wu J, Donnella H, et al. Cellular oxidative stress in pediatric leukemia and lymphoma patients undergoing treatment is associated with protein consumption. Nutrients. 2019;12(1):75. doi:10.3390/nu12010075.
-
Dilber B, Akbulut UE, Serin HM, et al. Plasma and erytrocyte oxidative stress markers in children with frequent breath-holding spells. Klin Padiatr. 2021;233(4):173-80. doi:10.1055/a-1369-9426.
-
Ahmed MZH, Saad RHAH, Gadalla A, et al. The association of oxidative stress of neonatal hyperbilirubinemia and vitamin E supplementation. Clin Exp Hepatol. 2024;10(1):30-8. doi:10.5114/ceh.2024.136230.
-
Demirtas MS, Yalcin SS. The use of human milk for therapeutic purposes other than nutrition. Turk Arch Pediatr. 2022;57(3):255-66. doi:10.5152/TurkArchPediatr.2022.22075.
-
Zhang HQ, Teng JH, Li Y, et al. Vitamin D status and its association with adiposity and oxidative stress in schoolchildren. Nutrition. 2014;30(9):1040-4. doi:10.1016/j.nut.2014.02.024.
-
Frijhoff J, Winyard PG, Zarkovic N, et al. Clinical relevance of biomarkers of oxidative stress. Antioxid Redox Signal. 2015;23(14):1144-70. doi:10.1089/ars.2015.6317.
Tables
Table 1. Important ROS molecules and their metabolism
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Sebahattin Memiş, Mehmet Semih Demirtaş, Hüseyin Erdal, Gizem Sorkulu Memiş. Oxidative stress in pediatric patients: mechanisms, implications and therapeutic approaches. Ann Clin Anal Med 2026;17(2):179-185
- Received:
- November 19, 2024
- Accepted:
- December 24, 2024
- Published Online:
- January 3, 2025
- Printed:
- February 1, 2026