
The prognostic significance of ast/alt (De Ritis) ratio on survival in patients underwent pancreaticoduodenectomy
De Ritis ratio and prognosis in pancreaticoduodenectomy
Authors
Abstract
AimPancreatic ductal adenocarcinoma (PDAC) has a poor prognosis. This study aimed to evaluate the AST/ALT (De Ritis) ratio as a prognostic biomarker in patients undergoing pancreaticoduodenectomy for PDAC.
MethodsClinical and pathological data of 222 PDAC patients who underwent pancreaticoduodenectomy between November 2010 and December 2018 were retrospectively analyzed. The prognostic value of the De Ritis ratio was assessed using ROC curve analysis. Kaplan–Meier and Cox regression models were used to evaluate their impact on disease-free survival (DFS) and overall survival (OS).
Results123 patients were analyzed (mean age: 63.48 ± 10.28 years; 43.1% female). The optimal AST/ALT threshold for survival prediction was 0.66. Patients with a higher De Ritis ratio had significantly shorter median DFS and OS (p=0.025 and p=0.048, respectively). Multivariate analysis identified advanced age (p<0.001), absence of chemotherapy (p<0.001), recurrence (p=0.003), prolonged hospital stay (p=0.016), positive surgical margins (p=0.012), and high metastatic lymph node count (p=0.006) as independent risk factors for lower OS. Similar factors also predicted shorter DFS.
ConclusionThe De Ritis ratio may serve as a prognostic factor in operable PDAC patients. If validated, it could be a simple, cost-effective tool for guiding surgical and neoadjuvant therapy decisions.
Keywords
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is the cause of the fourth-highest cancer-related deaths worldwide, and the number of newly diagnosed patients is gradually increasing.1 Because the disease becomes symptomatic in the advanced stages and therefore delays the diagnosis, only 15–20% of patients have the opportunity to undergo surgery at the time of diagnosis. Most patients have local or distant metastases at the time of diagnosis. Accordingly, the 5-year survival rate is less than 8%.2,3 Surgical resection followed by systemic chemotherapy remains the gold standard treatment. Despite advanced surgical and medical treatment methods, overall survival (OS) is quite low due to rapid local recurrence and systemic spread.4,5 Detailed preoperative risk assessment may improve treatment outcomes by optimizing patient selection for radical surgery.6 Therefore, there is a need for prognostic markers before surgery.
Despite recent advances in the identification of genetic, epigenetic, and molecular changes developed for use in preoperative risk assessment, the lack of standardization and expensive and/or time-consuming tests limit their routine use in daily clinical practice. Regularly used blood tests are relatively easy to evaluate without additional effort, making them attractive parameters for risk assessment.7
The ratio of aspartate aminotransferase (AST) and alanine aminotransferase (ALT) serum activities was first defined by Fernando De Ritis in 1957, and since then, the ratio between AST and ALT activities (AST/ALT) has been known as the De Ritis ratio.8 Aminotransferases, such as AST and ALT, are expressed by non-cancerous and cancerous cells in different cellular subdivisions and are strongly involved in cellular metabolism and cancer cell turnover.9 Alanine aminotransferase is involved in the “glucose-alanine cycle,” replacing alanine with pyruvate and strongly contributing to the replenishment of muscle-depleted glucose. Aspartate aminotransferase is required for aerobic glycolysis due to the displacement of nicotinamide adenine dinucleotide (NADH) within mitochondria. These transaminase reactions are especially important in muscle and liver cells but also in other cells with high metabolic activity.10 Both AST and ALT are easily measurable blood-based biomarkers that are routinely analyzed during preoperative preparation. Many studies conducted with solid tumors have reported that the AST/ ALT ratio is a biomarker associated with cancer prognosis. Tan et al. (2013) defined the De Ritis ratio as a suitable prognostic marker for cholangiocarcinoma, and it was associated with poor prognosis.11 Wu et al. (2019) reported in a metaanalysis involving 9400 patients that a high pretreatment De Ritis ratio is a prognostic factor for overall survival, cancerrelated survival, and disease-free survival in solid tumors, such as renal cell cancer, urinary tract urethral carcinoma, bladder cancer, and liver cancer.12 In a retrospective study by Nishikawa et al. involving 109 patients, the De Ritis ratio in urinary tract urothelial carcinoma was found to be a predictive factor independent of tumour-node-metastasis (TNM) staging.13 Katzke et al. (2020) conducted a prospective randomized cohort study and showed that a high ratio of De Ritis before treatment increases mortality in all lung, prostate, breast, and colon-rectal cancers14 In addition, De Ritis has been proven to be a biomarker with a prognostic role in non-malignant diseases, including cardiovascular-related deaths in diabetic patients.15
Although there are studies in the literature examining the relationship between AST/ALT ratio, disease-free survival (DFS) time in advanced pancreatic cancer, and chemotherapy response 1,16 , no study examining its possible relationship with the survival time in operable PDAC was found. This study aimed to examine the AST/ALT ratio, which can be a potential biomarker in determining survival time in pancreatic adenocarcinoma, which is one of the most important causes of death and morbidity worldwide.
Materials and Methods
After obtaining permission from the Gazi University Clinical Research Ethics Committee, the records of 222 patients who underwent pancreaticoduodenectomy and lymph node dissections for pancreatic adenocarcinoma at the Gazi University Faculty of Medicine General Surgery Clinic between November 2010 and December 2018 were analyzed retrospectively. Patients with metastatic disease at the time of diagnosis, patients who received pre-operative chemotherapy (CT) or radiotherapy (RT), patients who had chronic liver disease or inflammatory disease, and patients whose data could not be accessed were not included in the study.
In addition to demographic characteristics, such as age and gender, comorbidity, tumor diameter, tumor differentiation, TNM stage, T stage, N stage, albumin, carbohydrate antigen 19-9 (CA19-9) value, AST and ALT values, postoperative chemotherapy and/or radiotherapy, surgical margin (R0/ R1) status, presence of postoperative complications, and clinicopathological features, such as disease-free and overall survival (OS) times, were recorded. The tumor stage was determined according to the eighth edition of the International Union for Cancer Control (UICC).17 Follow-up examinations were performed every 3 months until 2 years after surgery and every 6 months after 2 years. Contrast-enhanced computed tomography sections (CT), biochemistry tests, carcinoembryonic antigen (CEA), and CA 19-9 tumor markers were evaluated in the follow-up examinations. The time between the day of surgery and the date of death was considered the survival time. The serum values of albumin, AST, ALT, and CA-19-9 were measured with a biochemical analyzer (Siemens 5600, Germany) according to the manufacturer’s instructions. The cut-off value was also calculated according to the ROC curve. The patients were divided into two groups according to high and low rates, according to a De Ritis ratio of 0.66 as the cutoff value.
Ethical Approval
This study was obtained from the Ethics Committee of Gazi University (Date: 09.06.2021, Decision No: 593).
Statistical AnalysisThe research data were evaluated using the SPSS 22.0 statistical package program. Descriptive statistical methods (mean, standard deviation, median, frequency, percentage, minimum, and maximum) were used to evaluate the study data. The conformity of the variables to the normal distribution was examined by visual (histogram) and analytical methods (Kolmogorov-Smirnov/Shapiro-Wilk). The DFS time and OS time of the patients were compared with the AST/ALT ratio. The Kaplan-Meier test was used for survival analysis. The Cox regression model was used for univariate and multivariate analyses. The statistical significance value was accepted as p<0.05.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
Detailed clinicopathological features of the 123 patients included in the study are shown in Table 1. The mean age of the patients was 63.48 ± 10.28 years; 83 (67.3%) were under the age of 70, and 53 (43.1%) were women. While 50.4% of the patients had concomitant chronic diseases, 23.6% had more than one additional disease. While complications were observed in 39.8% of the patients, the most common complications were intraabdominal abscess, hemorrhage, pancreatic fistula, biliary fistula, and gastric delayed emptying. Eighty-three point seven percent of the patients received adjuvant chemotherapy, and 47.2% received adjuvant radiotherapy. The median value of hospital stay was 17.3 ± 12.5. The mean tumor diameter was 3.1 ± 1.54 cm. While surgical margins were negative in 65% of the patients, the median value of the number of dissected metastatic lymph nodes was 3.2 ± 10.8. While recurrence was observed in 50 patients (40.7%), the median DFS time was 18.4 ± 17.3 months. It was confirmed at the last follow-up that 60.9% of the patients died. The median OS time was 22.2 ± 18.1 months. The mean values of AST, ALT, and AST/ALT ratio before surgery were 75.6 ± 64.9, 93.3 ± 87.4, and 1.0 ± 0.4 U/L, respectively.
The optimal threshold value for the AST/ALT ratio for survival prediction by ROC analysis was 0.66 (Table 2). The patients were divided into two groups according to the AST/ALT ratio: Group 1 < 0.66 (n = 36) and Group 2 ≥ 0.66 (n = 86). The clinicopathological variables of the patients according to the AST/ALT ratio are shown in Table 1. A high AST/ALT ratio was found to be statistically significantly associated with advanced age (p=0.003), high albumin level (p=0.007), and prolonged hospital stay (p=0.010).
ROC analysis was performed to measure the effectiveness of AST/ALT value in predicting mortality. According to this analysis, the area under the curve (AUC) was found to be 0.633 [AUCROC (95% CI): 0.633(0.520–0.747), p=0.019]. The sensitivity and specificity for the cut-off value of AST/ALT value ≥ 0.66 were 80.2% and 48.6%, respectively (Figure 1).
The median DFS and OS times were found to be lower in the patient group with a higher De Ritis rate (p<0.025 and p<0.048, respectively) (Figure 2 and Figure 3). The median OS duration of patients with a high AST/ALT ratio was 6 months shorter than patients with a low AST/ALT ratio (19 vs. 25 months). Similarly, the median DFS duration of patients with a high AST/ALT ratio was 7 months shorter (13 vs. 20 months) than patients with a low AST/ALT ratio (Table 3).
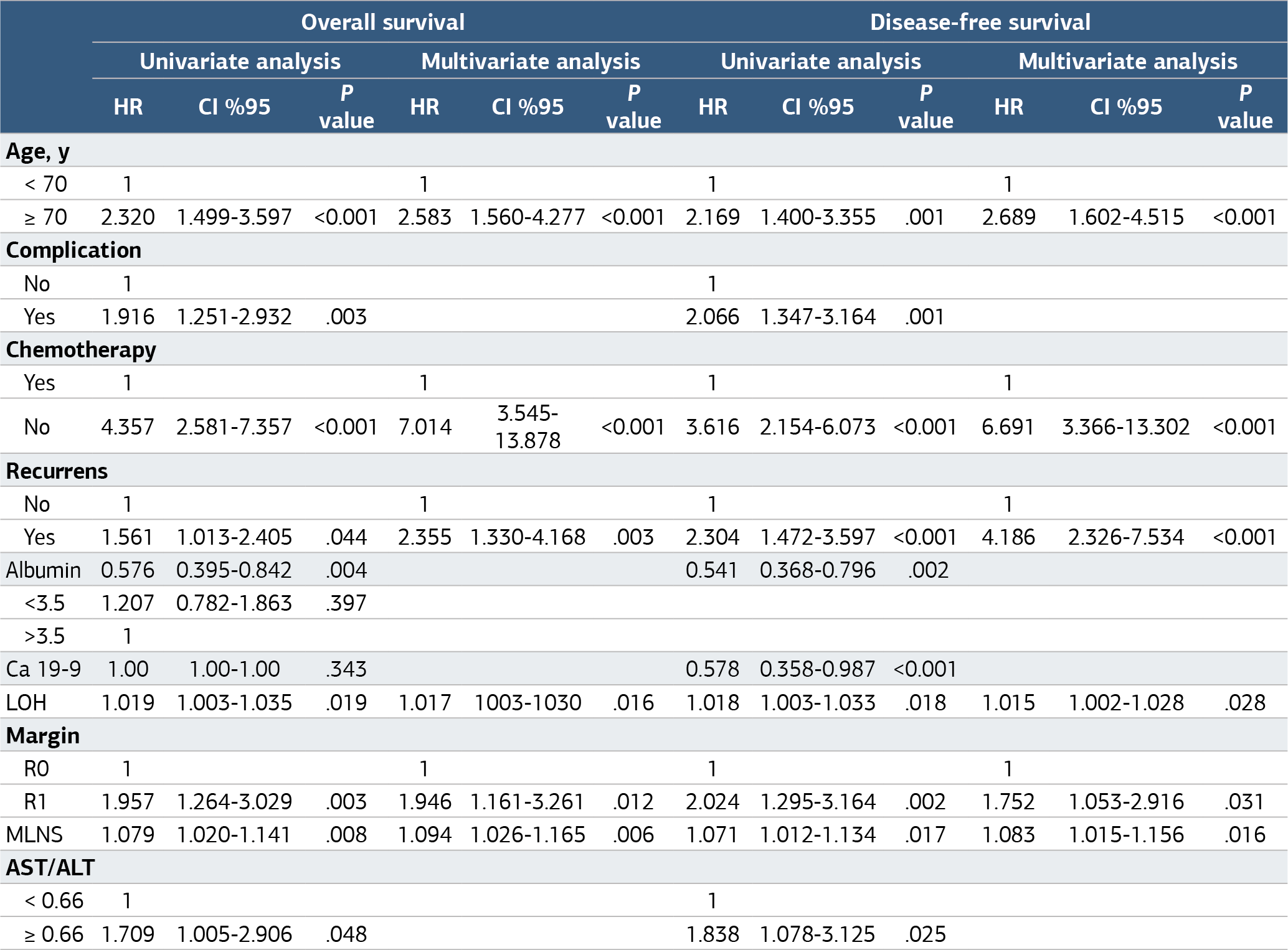
According to the univariate analysis results, a high AST/ ALT ratio (p=0.048), advanced age (p<0.001), presence of complications (p=0.003), no chemotherapy (p<0.001), low albumin value (p=0.004), prolonged hospital stay (p=0.019), a positive surgical margin (p=0.003), and a high number of metastatic lymph nodes (p=0.008) were associated with reduced overall survival times (Table 3). Similarly, a high AST/ ALT ratio (p=0.025), advanced age (p<0.001), presence of complications (p<0.001), failure to receive chemotherapy treatment (p<0.001), low albumin value (p=0.002), prolonged hospital stay duration (p=0.018), positive surgical margin (p=0.002), and high number of metastatic lymph nodes (p=0.017) were associated with DFS (Table 3).
According to the results of multivariate analysis, advanced age (p<0.001), not receiving chemotherapy (p<0.001), presence of recurrence (p=0.003), prolonged hospital stay (p=0.016), positive surgical margin (p=0.012), and high number of metastatic lymph nodes (p=0.006) were found to be independent risk factors for low OS time (Table 3). Similarly, advanced age (p<0.001), inability to receive chemotherapy (p<0.000), prolonged hospital stay (p=0.028), positive surgical margin (p=0.031), and high number of metastatic lymph nodes (p=0.016) were found to be independent prognostic factors for DFS (Table 3).
Discussion
In this study, the prognostic significance of the pretreatment AST/ALT (De Ritis) ratio was evaluated in patients who underwent pancreaticoduodenectomy for pancreatic adenocarcinoma. In our study, the cut-off value for the De Ritis ratio was 0.66. According to this cut-off value, it was shown that the DFS and OS times of the patients in the group with a high pre-treatment De Ritis ratio were lower than those of the patients in the group with a low De Ritis ratio.
Data on the prognostic role of the AST/ALT ratio in pancreatic adenocarcinoma are limited. To date, only a few studies have examined the prognostic role of the AST/ALT ratio in pancreatic adenocarcinoma. Riedl et al. (2020) showed that a high serum De Ritis ratio before gemcitabine/nab-paclitaxel therapy in 202 patients with advanced PDAC was significantly associated with reduced disease-free survival, overall survival, and time to progression-free survival (PFS). In addition, they showed that a high De Ritis ratio was a strong predictor of a poor response to combination chemotherapy with gemcitabine/nabpaclitaxel. In conclusion, they suggested that the ratio of De Ritis could be an easy and new mediator factor that can be used to predict prognoses for patients with advanced PDAC.16 Another study evaluating the results of 191 patients with locally advanced and metastatic pancreatic cancer showed that neutrophils, lymphocytes, platelets, CA19-9, total bilirubin, albumin, and alkaline phosphatase, together with the De Ritis ratio, were independent prognostic markers.1 The results of our study were similar to the results of studies suggesting that the De Ritis ratio is a prognostic factor in patients with PDAC. Contrary to these studies, our study investigated the prognostic significance of the De Ritis ratio in non-advanced patients who underwent pancreaticoduodenectomy, unlike studies investigating the prognostic effect of the De Ritis ratio in advanced pancreatic cancer. The recommendation of the De Ritis ratio as a prognostic marker in operable PDAC increases the clinical importance of our study.
ALT is involved in the “glucose-alanine cycle,” replaces alanine with pyruvate, and strongly contributes to the replenishment of muscle-depleted glucose.10 Aspartate aminotransferase plays an important role in aerobic glycolysis in mitochondria via the malate-aspartate shuttle and nicotinamide adenine dinucleotide hydrogen (NADH) produced in the cytoplasm.18 Warburg suggested that aerobic glycolysis, in which AST plays an active role, increases in cancer cells compared to normal cells and that biochemical markers based on this theory can be used to predict prognosis.19 In our study, the high De Ritis ratio due to increased AST levels in patients with PDAC can be explained by Warburg’s theory.
The mechanisms underlying the relationship between AST and ALT in cancer metabolism are not fully understood. Aspartate aminotransferase is widely expressed in different tissue types, while ALT is thought to be more specific to the liver.10 Pathological processes associated with higher proliferation, tissue damage, and tumor cell turnover may lead to a stronger increase in AST compared to ALT. In vitro experiments have revealed that ALT levels are decreased in more invasive cells compared to less invasive cancer cells. It is thought that this decrease in serum ALT levels may be due to the result of improved metabolism and increased consumption of ALT in aggressive cancer cells.20 The serum levels of AST and ALT can be affected by many factors, such as chronic hepatitis, coronary heart disease, impaired kidney function, and certain medications. Therefore, the use of numerical values alone to directly predict cancer prognosis has low sensitivity and specificity. Instead, we think that the combination of AST and ALT is more appropriate as a composite parameter. The highly invasive nature of PDAC can be explained by our results, the high De Ritis ratio, and the effect of ALT levels on cancer metabolism. Considering all these data, our results showed that the De Ritis ratio in patients with PDAC could be an attractive potential biomarker in clinical follow-up. In this study, age, inability of the patient to receive chemotherapy, relapse of the disease, prolonged hospital stay, positive surgical margin, and a high number of metastatic lymph nodes were found to be independent prognostic markers in operable pancreatic cancers. However, the small number of patients and the retrospective analysis of the data can be cited as limitations of our research. To reveal the usefulness of the De Ritis ratio as a biomarker, a longer-term study in a larger population should be conducted with a prospective design.
Limitations
This study has several important limitations. Due to its retrospective design, the collection of data retrospectively may introduce certain biases and missing information. Additionally, the limited sample size restricts the generalizability of the findings. Since our study was conducted at a single center, multicenter studies are needed to validate the results. Finally, comprehensive prospective studies that include other biochemical and genetic markers are necessary to better elucidate the prognostic role of the De Ritis ratio.
Conclusion
The De Ritis ratio can be used as a prognostic factor in patients with PDAC who are considered operable. To reveal the usefulness of the De Ritis ratio as a biomarker, longer-term studies in a larger population should be conducted with a prospective design. If confirmed by additional studies, the De Ritis ratio can be used as a simple and inexpensive marker for prognosis in the decision of surgery or neoadjuvant chemoradiotherapy.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
ALT: Alanine aminotransferase
AST: Aspartate aminotransferase
CA19-9: Carbohydrate antigen 19-9
CEA: Carcinoembryonic antigen
CT: Chemotherapy
DFS: Disease-free survival
NADH: Nicotinamide adenine dinucleotide hydrogen
OS: Overall survival
PDAC: Pancreatic ductal adenocarcinoma
ROC: Receiver operating characteristic
RT: Radiotherapy
TNM: Tumor-node-metastasis
UICC: International Union for Cancer Control
References
-
Varol U, Kaya E, Oflazoglu U, et al. Prognostic role of De Ritis and basal neutrophil to lymphocyte ratio in patients with advanced stage pancreatic cancer. J BUON. 2020;25(2):1063-1069. doi:10.5455/annalsmedres.2020.01.057
-
Wu W, He X, Yang L, et al. Rising trends in pancreatic cancer incidence and mortality in 2000-2014. Clin Epidemiol. 2018;10:789-797. doi:10.2147/clep.s160018
-
Seoane-Mato D, Nuñez O, Fernández-de-Larrea N, et al. Long-term trends in pancreatic cancer mortality in Spain (1952-2012). BMC Cancer. 2018;18(1):625. doi:10.1186/s12885-018-4494-3
-
Hartwig W, Werner J, Jäger D, Debus J, Büchler MW. Improvement of surgical results for pancreatic cancer. Lancet Oncol. 2013;14(11):e476-e485. doi:10.1016/s1470-2045(13)70172-4
-
Xu J, Shi KQ, Chen BC, Huang ZP, Lu FY, Zhou MT. A nomogram based on preoperative inflammatory markers predicting the overall survival of pancreatic ductal adenocarcinoma. J Gastroenterol Hepatol. 2017;32(7):1394-1402. doi:10.1111/jgh.13676
-
Stevens L, Pathak S, Nunes QM, et al. Prognostic significance of preoperative C-reactive protein and the neutrophil-lymphocyte ratio in resectable pancreatic cancer: a systematic review. HPB (Oxford). 2015;17(4):285-291. doi:10.1111/hpb.12355
-
Knittelfelder O, Delago D, Jakse G, et al. The AST/ALT ratio predicts survival in patients with oral and oropharyngeal cancer. Diagnostics (Basel). 2020;10(11):1-11. doi:10.3390/diagnostics10110973
-
De Ritis F, Coltorti M, Giusti G. An enzymic test for the diagnosis of viral hepatitis: the transaminase serum activities. Clin Chim Acta. 1957;2(1):70-74. doi:10.1016/0009-8981(57)90027-x
-
Koppenol WH, Bounds PL, Dang CV. Otto Warburg’s contributions to current concepts of cancer metabolism. Nat Rev Cancer. 2011;11(5):325-337. doi:10.1038/nrc3038
-
Botros M, Sikaris KA. The De Ritis ratio: the test of time. Clin Biochem Rev. 2013;34(3):117-130.
-
Tan X, Xiao K, Liu W, Chang S, Zhang T, Tang H. Prognostic factors of distal cholangiocarcinoma after curative surgery: a series of 84 cases. Hepatogastroenterology. 2013;60(128):1892-1895.
-
Wu J, Chen L, Wang Y, Tan W, Huang Z. Prognostic value of aspartate transaminase to alanine transaminase ratio in solid tumors: a pooled analysis of 9400 patients. Onco Targets Ther. 2019;12:5201-5213. doi:10.2147/ott.s204403
-
Nishikawa M, Miyake H, Fujisawa M. De Ritis ratio as a significant predictor of recurrence-free survival in patients with upper urinary tract urothelial carcinoma following nephroureterectomy. Urol Oncol. 2016;34(9):417.e9-417.e15. doi:10.1016/j.urolonc.2016.04.001
-
Katzke V, Johnson T, Sookthai D, Hüsing A, Kühn T, Kaaks R. Circulating liver enzymes and risks of chronic diseases and mortality in the prospective EPIC-Heidelberg case-cohort study. BMJ Open. 2020;10(3):e033532. doi:10.1136/bmjopen-2019-033532
-
Zoppini G, Cacciatori V, Negri C, et al. The aspartate aminotransferase-to-alanine aminotransferase ratio predicts all-cause and cardiovascular mortality in patients with type 2 diabetes. Medicine (Baltimore). 2016;95(43):e4821. doi:10.1097/md.0000000000004821
-
Riedl JM, Posch F, Prager G, et al. The AST/ALT ratio predicts clinical outcome in patients with pancreatic cancer treated with first-line nab-paclitaxel and gemcitabine: post hoc analysis of an Austrian multicenter, noninterventional study. Ther Adv Med Oncol. 2020;12:1758835919900872. doi:10.1177/1758835919900872
-
Cong L, Liu Q, Zhang R, et al. The tumor size classification of the 8th edition of the TNM staging system is superior to that of the 7th edition in predicting the survival outcome of pancreatic cancer patients after radical resection and adjuvant chemotherapy. Sci Rep. 2018;8(1):10383. doi:10.1038/s41598-018-28193-4
-
Sookoian S, Pirola CJ. Liver enzymes, metabolomics, and genome-wide association studies: from systems biology to the personalized medicine. World J Gastroenterol. 2015;21(3):711-725. doi:10.3748/wjg.v21.i3.711
-
Warburg O. On respiratory impairment in cancer cells. Science. 1956;124(3215):269-270. doi:10.1126/science.124.3215.269
-
Conde VR, Oliveira PF, Nunes AR, et al. The progression from a lower to a higher invasive stage of bladder cancer is associated with severe alterations in glucose and pyruvate metabolism. Exp Cell Res. 2015;335(1):91-98. doi:10.1016/j.yexcr.2015.04.007
Figures

Figure 1. ROC curve graph of AST/ALT value of research participants
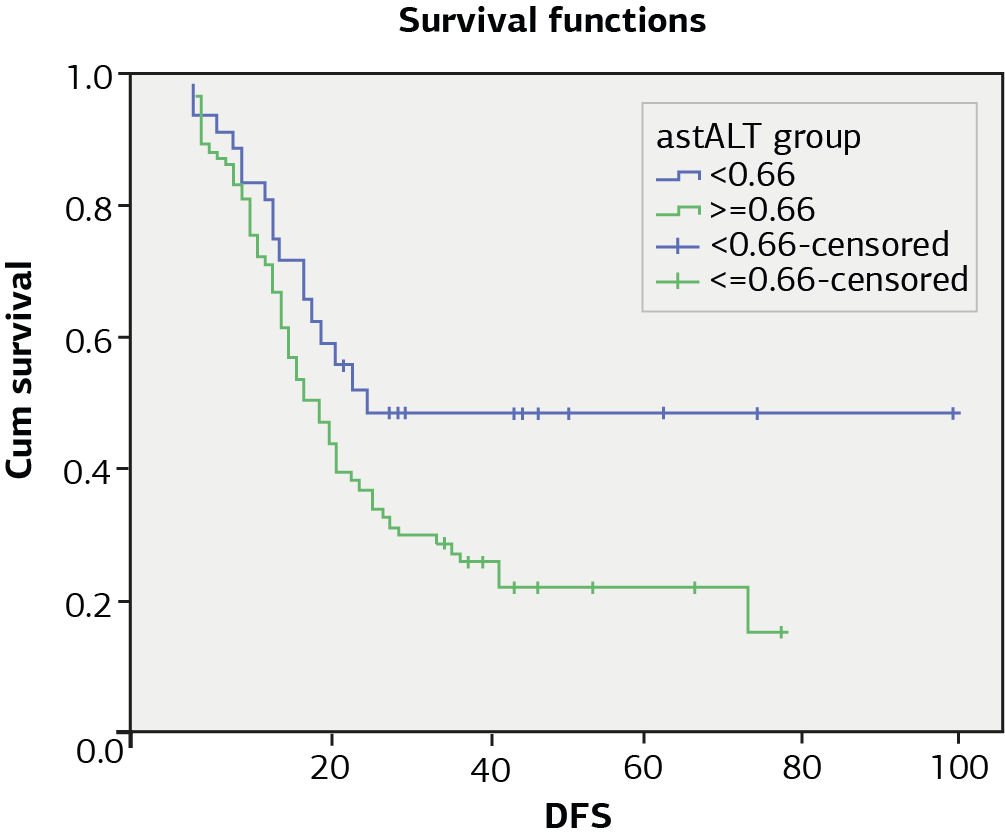
Figure 2. The effect of de ritis on disease free survival
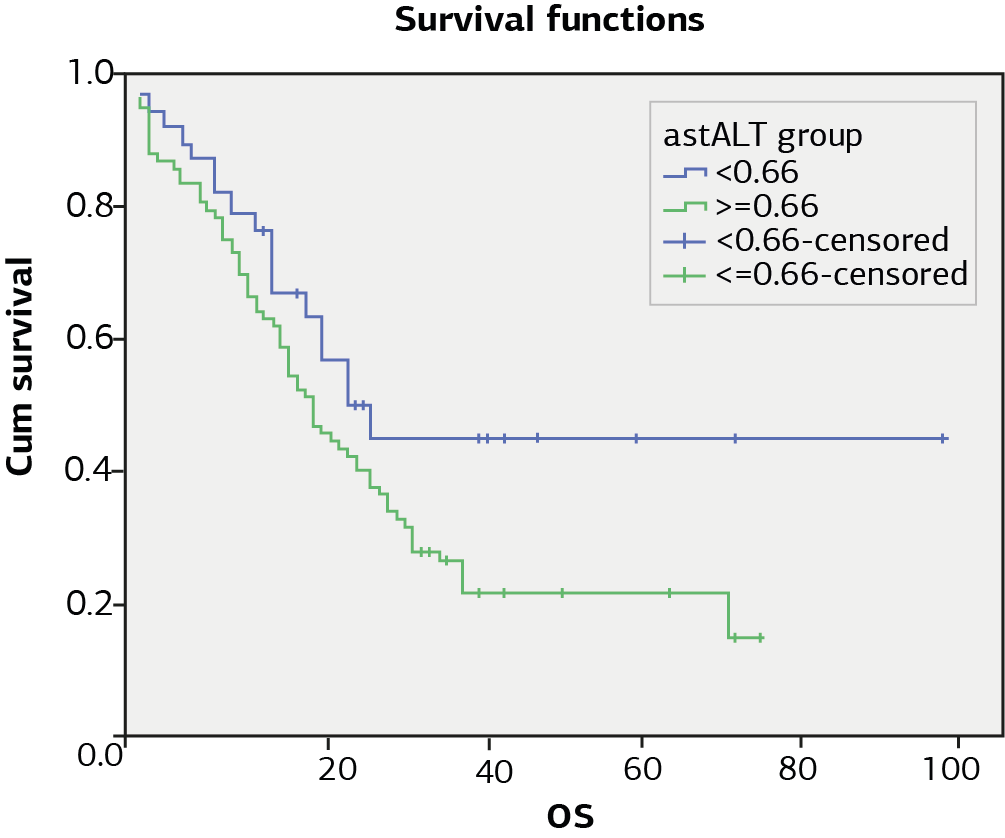
Figure 3. The effect of de ritis on overall survival
Tables
Table 1. The relationship between the descriptive characteristics of the individuals participating in the research and the AST/ ALT group

Table 2. Survival rates of patients according to De Ritis

Table 3. Univariate and multivariate Cox regression analyses of prognostic factors for overall and disease-free survival
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Saygin Altiner, Aydin Yavuz, Huseyin Gobut, Cagri Buyukkasap, Kursat Dikmen, Hasan Bostanci, Emre Gülçek, İsmail Emre Gokce, Mustafa Kerem. The prognostic significance of ast/alt (De Ritis) ratio on survival in patients underwent pancreaticoduodenectomy. Ann Clin Anal Med 2025;16(2):139-145. doi:10.4328/ACAM.22497
- Received:
- November 22, 2024
- Accepted:
- December 24, 2024
- Published Online:
- January 25, 2025
- Printed:
- February 1, 2025