
How does the mental health of caregivers affect diabetes management inadolescents with type 1 diabetes?
Diabetes caregiver mental health
Authors
Abstract
AimThe current study examined the impact of mental health status and socioeconomic conditions on diabetes management in adolescents with diabetes and their caregivers.
MethodsIn this cross-sectional study, the Patient Health Questionnaire (PHQ-9) and the Hospital Anxiety and Depression Scale (HADS) were administered to adolescents over the age of ten who have had type 1 diabetes (T1D) for at least two years, along with their caregivers. The questionnaire results were assessed alongside the most recent HbA1c levels and the annual average HbA1c levels.
ResultsA statistically significant and positive association was found between the average child’s HbA1C and the parent’s PHQ-9 score (Spearman’s rho = 0.332, p=0.007), parent’s HADS anxiety (Spearman’s rho = 0.328, p=0.008), and HADS depression (Spearman’s rho = 0.322, p=0.010) scores. There was also a positive and statistically significant association between the parent’s PHQ-9 score (Spearman’s rho = 0.291, p=0.020) and depression (Spearman’s rho = 0.280, p=0.025) scores. However, no statistically significant association was found between the adolescents’ average and last HbA1C levels and the PHQ-9, anxiety, and depression scores.
ConclusionParental mental health is as essential in the management of diabetes during adolescence as it is during childhood and should be evaluated regularly.
Keywords
Introduction
With its limitations and daily demands, type 1 diabetes mellitus (T1D) requires some parental adaptations. Parental adaptation has been identified as having a detrimental or protective effect on children’s ability to cope with this condition.1 With the recent interest in this aspect of the disease, many authors have focused on the mental health status of caregivers, who play an essential role in disease management.2,3 Due to the complexity of T1D management, multidisciplinary support is needed, with particular attention to patient and family psychology and emotions. Indeed, healthcare providers should be involved with parents, as T1D involves daily responsibilities such as blood sugar level assessments, insulin administration, and food intake regulation.4 Therefore, with this “extra work,” difficulties in parent-child/adolescent interactions and increases in parental stress are reported by parents.5
Adolescence is when children seek independence while relying on their families for financial, emotional, and psychological support. Navigating this complex balance can be particularly challenging for adolescents with chronic illnesses, such as T1D, when it comes to managing their health. Many studies indicate that both younger and older adolescents with T1D often experience poor glycemic control and worse overall health outcomes.6,7 Previous research has shown that past and present family interactions and relationships impact the development of adolescents’ self-care behaviors. Furthermore, parenting style and the alignment of family communication may influence glycemic control.8,9
In this study, we assessed the influence of adolescent mental health and that of their primary caregivers on managing type 1 diabetes.
Materials and Methods
The study included 64 children aged 10 years and older who had been diagnosed with Type 1 diabetes for at least 2 years and their caregivers.
Height, weight, and BMI variables were standardized using standard deviation scores (SDS) based on Turkish norms.10 Pubertal development and breast and pubic hair growth were assessed using Tanner criteria.11 After the examination, blood samples were collected from the patients to evaluate their HbA1c levels. The average HbA1c value was calculated by summing the four values examined over the last year and then dividing by four.
Before administering the questionnaire, we collected and recorded the sociodemographic characteristics of patients and their caregivers. This included information about the primary caregiver, marital status, employment status, educational background, the number of people living in the household, and the average monthly income, among other factors. Two pediatric endocrinologists in two different centers administered the Patient Health Questionnaire (PHQ-9) and the Hospital Anxiety and Depression Scale (HADS) questionnaires separately to the patient and caregiver.
The relationship between questionnaire results, sociodemographic data, the last glycated hemoglobin (HbA1c), and HbA1c averages in the previous year was evaluated.
Hospital Anxiety and Depression Scale (HADS)HADS was designed to screen for the presence of anxiety and depression in patients with physical illness.12 The Turkish validity and reliability study was conducted by Özdemir et al.13 The self-report scale consists of 14 items, 7 of which investigate depression and 7 of which investigate anxiety symptoms. Responses are evaluated on a four-point Likert scale and scored between 0 and 3. The scale is designed to screen for anxiety and depression quickly to identify risk groups, not to make a diagnosis.
In preparing the score, 0-1 was accepted as “no risk,” 2 score as “borderline disease risk,” and 3-4 as “marked disease risk.” The HAD scale has proven to be a helpful assessment tool, and score ranges minimize false positive or negative results (12). It has been shown that the score obtained from the scale is not affected by physical illness.14
Patient Health Questionnaire (PHQ-9)The Patient Health Questionnaire-9 (PHQ-9) is a diagnostic tool designed to identify common mental disorders, such as depression, in primary care settings. Kroenke et al. validated it, measuring nine symptoms based on the PHQ-9 and diagnosing depression according to DSM-IV criteria.15 The short and straightforward nature of the questions is a significant advantage, making them easy to apply. Sari et al.16 carried out the Turkish reliability study of the questionnaire.
The questionnaire consists of 9 questions, each scored from 0 (never) to 3 (almost every day). The scores are added up for each question. According to the original questionnaire scoring system, scores between 1 and 4 are graded as minimal, 5-9 as mild, 10-14 as moderate, 15-19 as moderately severe, and 20-27 as severe depression. In addition to the nine diagnostic questions, the test includes one such question: “If you checked any problems, how difficult did they make it for you to do your job, take care of household chores, or get along with others?”. However, this question does not affect the scoring.15
Ethical ApprovalThis study was approved by the Ethics Committee of Selçuk University (Date: 03.07.2024, Decision No: 341).
Statistical AnalysisAll statistical analysis was performed using R version 4.2.1 (www.r-project.org) statistical software. Numerical data were presented as mean ± standard deviation (ranges: min – max), and categorical data were described as count (n) and percentage (%). Spearman’s rho correlation coefficient was used to examine the relationship between HbA1C levels and PHQ-9 scores in children and parents. A two-tailed p-value less than 0.05 was considered statistically significant.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
The mean age of the 64 study participants was 169.33 ± 27.97 months. Thirty-eight of the participants (59.4%) were male. The mean body weight of the participants was 54.52 ± 14.26 kg (SD= 0.08 ± 1.21). Fifty-seven participants had completed puberty. The mean duration of diabetes in the patients was 5.63 ± 3.36 years. The participants’ mean HbA1c values for the last year were 8.92 ± 1.83, and the HbA1c at the previous visit was 8.85 ± 1.77. The caregivers of 58 (90.6%) participants were their mothers. Only six children (9.4%) reported experiencing peer bullying due to their illness, while twelve children (18.8%) felt stigmatized. The general characteristics of the participants and the questionnaire results are shown in Table 1.
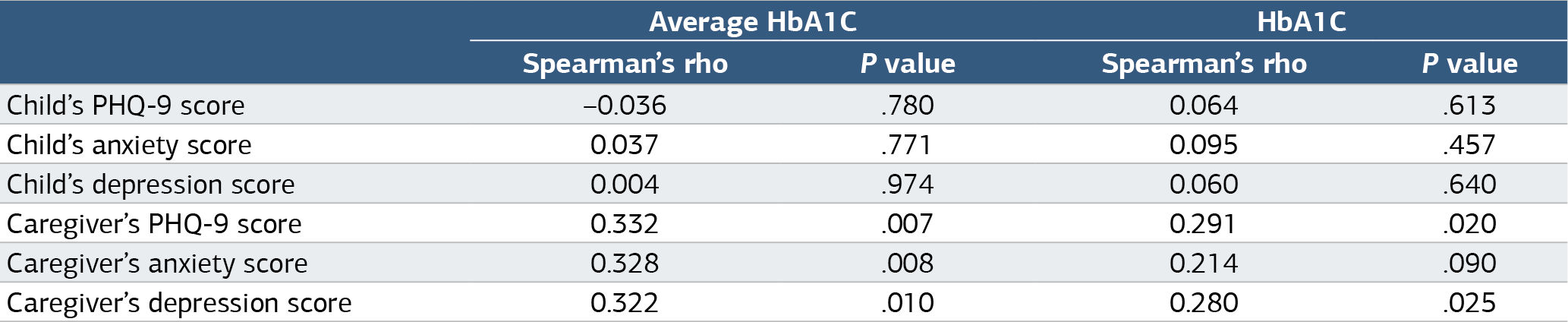
A statistically significant positive association was found between the average child’s HbA1C and the parent’s PHQ-9 score (Spearman’s rho = 0.332, p=0.007). Similar associations were observed with the parent’s HADS anxiety (Spearman’s rho = 0.328, p=0.008) and HADS depression (Spearman’s rho = 0.322, p=0.010) scores. There was also a positive and statistically significant association between the parent’s PHQ9 score (Spearman’s rho = 0.291, p=0.020) and depression (Spearman’s rho = 0.280, p=0.025) scores (Figure 1). However, no statistically significant association was found between the adolescents’ average and last HbA1C levels and the PHQ9, anxiety, and depression scores (Table 2). No considerable relationship was identified between HbA1c levels and the other sociocultural factors assessed.
Discussion
The results of this study identified a relationship between caregiver anxiety and depression and glycated hemoglobin (HbA1c) levels, thus contributing to the existing literature by highlighting the importance of caregiver mental health in adolescent diabetes management.
A substantial body of literature shows cross-sectional and longitudinal associations between family and adolescent-level variables and glycemic control in younger and older adolescents.17 Family conflict related to diabetes, the perceived burden on parents, and a critical parenting style have been consistently linked to poor glycemic control.18 However, to resolve this complexity sensibly, there is no doubt that the mental health of the caregiver is also essential, and it will negatively affect diabetes management. In this study, a more substantial relationship was identified between caregiver mental health and HbA1c than between the adolescents’ mental health.
Studies have shown that individuals with lower socioeconomic status experienced more conflict with their children, less acceptance of diabetes, and increased parental stress; however, this status did not influence the level of parental monitoring of diabetes care.19 Participants in this study were generally of low economic status with similar socioeconomic levels. In other words, since the patients were a uniform group in terms of socioeconomic level, we believed that this factor did not act as an independent variable affecting HbA1c among them. Similar to the study by Silina et al., the data analysis failed to establish a statistically reliable relation between the child’s environment and HbA1c or between socioeconomic factors in that circumference.20
Many young people with diabetes face challenges related to self-esteem, body image, social roles, and relationships with peers. During adolescence, acceptance by friends and maintaining peer relationships are crucial. To avoid being seen as different by their peers, adolescents may use passive coping strategies, such as withdrawing, avoiding activities, and not adhering to their treatment plans.21 The stigma associated with chronic diseases is defined as negative social judgment based on the condition or its management. This stigma can lead to perceived or experienced exclusion, rejection, blame, stereotyping, and loss of status. Adolescents and young adults may be especially vulnerable to stigma and its harmful effects during these life stages.22 Although studies are showing that stigma harms diabetes control by causing high HbA1c levels and more hypoglycemia, the number of patients who felt stigmatized and experienced peer bullying was very low among our patients.23 There was no significant difference in HbA1c levels between patients who reported experiencing peer bullying or feeling stigmatized compared to others.
Studies have reported that fear of hypoglycemia, chronic sadness, and uncertainty are some common psychological responses for parents of children with diabetes, especially among mothers, and this may increase parental depression and anxiety, leading to higher HbA1c.24 In our study, 90.6% of the caregivers were mothers. Thirty-one mothers had a HADS anxiety score above seven. As the anxiety and depression scores of caregivers increased, HbA1c levels also rose. Including fathers in the diabetes management process may reduce the stress burden on caregivers.
Limitations
The study has several limitations. Because it was a crosssectional study, causality could not be established, but the direction of the observed relationships remained unclear. Furthermore, the research relied on self-reported assessments of anxiety and depression, which may have introduced bias. Additionally, the study specifically targeted adolescents with T1D and their caregivers, meaning that the results may not be relevant to other age groups or types of diabetes. The limited sample size may impact how broadly the results can be applied. Despite these limitations, our study offers essential practical and clinical inferences. Improving caregiver mental health should be an important goal for families with an adolescent diagnosed with T1D, as this may lead to improved diabetes management.
Conclusion
In conclusion, the study suggests that caregiver mental health is essential to children’s diabetes management outcomes. This highlights the importance of addressing mental health concerns in both children and their parents as part of diabetes care strategies. Diabetes is not solely an endocrine disorder; it also affects psychological and psychiatric health, the socioeconomic environment, and overall family functioning.
Diabetes care should be multidisciplinary, involving endocrinologists, primary care physicians, psychologists, psychiatrists, social workers, and other specialists. Fathers should also be involved in diabetes management, sharing the often overwhelming caregiver stress on mothers. It is important to note that working with parents is a critical component of interdisciplinary diabetes care, including preventive measures to improve mental health.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants and their caregivers prior to inclusion in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
BMI: Body Mass Index
DSM-IV: Diagnostic And Statistical Manual Of Mental Disorders, Fourth Edition
HADS: Hospital Anxiety And Depression Scale
HbA1c: Glycated Hemoglobin
PHQ-9: Patient Health Questionnaire-9
SDS: Standard Deviation Score
STROBE: Strengthening The Reporting Of Observational Studies In Epidemiology
T1D: Type 1 Diabetes Mellitus
References
-
Körner A, Würz J, Brosseau DC, Brähler E, Kapellen T, Kiess W. Parental dyadic coping in families of children and adolescents with type 1 diabetes. J Pediatr Endocrinol Metab. 2013;26(9-10):867-875. doi:10.1515/jpem-2012-0410
-
Yaqoob U, Ali Khan M, Khemani L, Ul-Haq F, Rafiq J, Iftikhar AS. Diabetes mellitus in children and its effect on caregivers’ mental health. Cureus. 2018;10. doi:10.7759/cureus.2409
-
Jönsson L, Lundqvist P, Tiberg I, Hallström I. Type 1 diabetes: impact on children and parents at diagnosis and one year after the child’s diagnosis. Scand J Caring Sci. 2014;29(1):126-135.
-
Sherifali D, Ciliska D, O’Mara L. Parenting children with diabetes: exploring parenting styles on children living with type 1 diabetes mellitus. Diabetes Educ. 2009;35(3):476-483. doi:10.1177/0145721709333268
-
Whittemore R, Jaser S, Chao A, Jang M, Grey M. Psychological experience of parents of children with type 1 diabetes: a systematic mixed-studies review. Diabetes Educ. 2012;38:562-579. doi:10.1177/0145721712445216
-
Petitti DB, Klingensmith GJ, Bell RA, et al. Glycemic control in youth with diabetes: the SEARCH for Diabetes in Youth study. J Pediatr. 2009;155(5):668-672. doi:10.1016/j.jpeds.2009.05.025
-
Bryden KS, Dunger DB, Mayou RA, Peveler RC, Neil HAW. Poor prognosis of young adults with type 1 diabetes: a longitudinal study. Diabetes Care. 2003;26(4):1052-1057. doi:10.2337/diacare.26.4.1052
-
Miller DC, Byrnes JP. To achieve or not to achieve: a self-regulation perspective on adolescents’ academic decision making. J Educ Psychol. 2001;93:677-685. doi:10.1037/0022-0663.93.4.677
-
Katz ML, Volkening LK, Butler DA, Anderson BJ, Laffel LM. Family-based psychoeducation and care ambassador intervention to improve glycemic control in youth with type 1 diabetes: a randomized trial. Pediatr Diabetes. 2014;15(2):142-150. doi:10.1111/pedi.12065
-
Neyzi O, Gunoz H, Furman A. Reference values for body weight, height, head circumference, and body mass index in Turkish children. Turk Pediatri Ars. 2008;51:1-14.
-
Marshall WA, Tanner JM. Variations in pattern of pubertal changes in girls. Arch Dis Child. 1969;44(235):291-303. doi:10.1136/adc.44.235.291
-
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361-370. doi:10.1111/j.1600-0447.1983.tb09716.x
-
Aydemir Ö. Hastane Anksiyete ve Depresyon Ölçeği Türkçe formunun geçerlilik ve güvenilirliği. Turk Psikiyatri Derg. 1997;8(4):280-287.
-
Clark DA, Steer RA. Use of nonsomatic symptoms to differentiate clinically depressed and nondepressed hospitalized patients with chronic medical illnesses. Psychol Rep. 1994;75(3 pt 1):1089-1090. doi:10.2466/pr0.1994.75.3.1089
-
Kroenke K, Spitzer RL, Williams JBW. Validity of a brief depression severity inventory. J Gen Intern Med. 2001;16(9):606-613.
-
Sarı YE, Kökoğlu B, Balcıoğlu H, et al. Turkish reliability of the Patient Health Questionnaire-9. Biomed Res. 2016;27:460-462.
-
Nagy BE, Munkácsi B, Kovács KE. Factors influencing adherence among youth with type 1 diabetes mellitus: the Hungarian case. Curr Diabetes Rev. 2021;17(2):222-232. doi:10.2174/1573399816666200120123719
-
Lewin AB, Heidgerken AD, Geffken GR, et al. The relation between family factors and metabolic control: the role of diabetes adherence. J Pediatr Psychol. 2006;31(2):174-183. doi:10.1093/jpepsy/jsj004
-
Caccavale LJ, Weaver P, Chen R, Streisand R, Holmes CS. Family density and SES related to diabetes management and glycemic control in adolescents with type 1 diabetes. J Pediatr Psychol. 2015;40(5):500-508. doi:10.1093/jpepsy/jsu113
-
Silina E, Taube M, Zolovs M. Exploring the mediating role of parental anxiety in the link between children’s mental health and glycemic control in type 1 diabetes. Int J Environ Res Public Health. 2023;20(19):6849. doi:10.3390/ijerph20196849
-
Berntsson L, Berg M, Brydolf M, Hellström A. Adolescents’ experiences of well-being when living with a long-term illness or disability. Scand J Caring Sci. 2007;21(4):419-425. doi:10.1111/j.1471-6712.2006.00490.x
-
Browne JL, Ventura A, Mosely K, Speight J. I’m not a druggie, I’m just a diabetic: a qualitative study of stigma from the perspective of adults with type 1 diabetes. BMJ Open. 2014;4(7). doi:10.1136/bmjopen-2014-005625
-
Brazeau AS, Nakhla M, Wright M, et al. Stigma and its impact on glucose control among youth with diabetes: protocol for a Canada-wide study. JMIR Res Protoc. 2016;5(4). doi:10.2196/resprot.6629
-
Barnard K, Thomas S, Royle P, Noyes K, Waugh N. Fear of hypoglycemia in parents of young children with type 1 diabetes: a systematic review. BMC Pediatr. 2010;10:50. doi:10.1186/1471-2431-10-50
Figures

Figure 1. The relationship between average and last HbA1C and Caregiver’s PHQ-9, anxiety, and depression scores
Tables
Table 1. General Characteristics of children and caregivers and questionnaire results
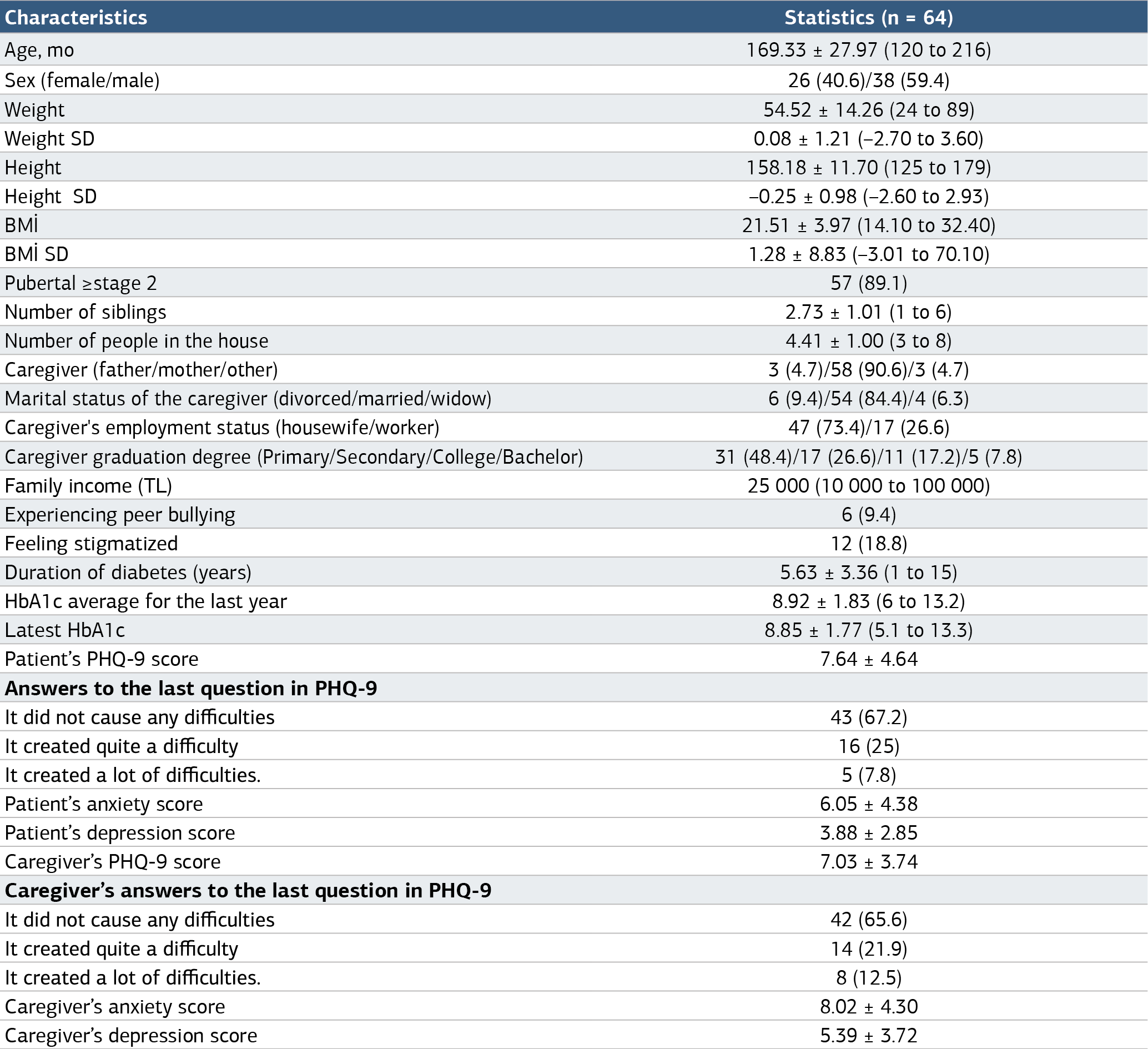
Table 2. The relationship between HbA1c and Questionnaire Scores
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Fatma Özgüç Çömlek, Saime Ergen Dibeklioğlu, Muslu Kazım Körez. How does the mental health of caregivers affect diabetes management inadolescents with type 1 diabetes? Ann Clin Anal Med 2025;16(3):166-170. doi:10.4328/ACAM.22502
- Received:
- November 25, 2024
- Accepted:
- January 13, 2025
- Published Online:
- January 24, 2025
- Printed:
- March 1, 2025