
Immunohistochemical markers affecting nodal metastasis in breast cancerand imaging methods for detection of axillary lymph node metastasis
Markers affecting nodal metastasis in breast cancer
Authors
Abstract
AimAxillary lymph node metastasis (ALNM) is a prognostic determinant of breast cancer (BC) and influences the treatment decision. Our study aimed to determine the factors associated with ALNM in BC and to accurately evaluate the ALN status with imaging methods while determining the treatment modality.
MethodsPatients (n=417) who underwent BC surgery in our clinic were included. Patient’s axillary ultrasound (AUS), magnetic resonance imaging (MRI), 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG-PET/CT) reports and immunohistochemical data were collected for analysis.
ResultsALNM was found in 59.7% (n = 249) of the patients. Invasive ductal carcinoma (IDC), invasive lobular carcinoma (ILC), lymphovascular invasion, and perineural invasion were found to be associated with ALNM (p<0.001). Tumor histological type was found to be the factor affecting true/false positivity or true/false negative of AUS, MRI, 18F-FDG-PET/CT (p<0.01, p=0.012, p=0.006).
ConclusionPremenopause, IDC, ILC, and the presence of LVI or PNI are factors that increase the risk of ALNM. MRI is the most reliable to accurately predict ALNM, followed by AUS and 18F-FDG-PET/CT. If the tumor type is IDC and ILC, AUS and MRI may be superior in predicting ALNM positivity. All three imaging modalities may be reliable in accurately predicting axilla negativity in other tumor types.
Keywords
Introduction
Breast cancer is among the most common cancers worldwide and the second most common cause of cancer-related death in women. Early diagnosis and use of aggressive multimodal treatment options have resulted in a reduction in mortality and morbidity in recent years.1,2 However, despite all developments, axillary lymph node (ALN) status remains the most important prognostic factor in staging, treatment, prognosis, recurrence, and survival in breast cancer.3
Until recently, axillary lymph node dissection was standard in patients with axillary lymph node metastases (ALNM), and then the sentinel lymph node biopsy (SLNB) method became standard in clinically node-negative patients. However, SLNB is also an operation and preoperative recognition of ALNM is essential in determining the treatment modality. Ultrasoundguided fine needle aspiration cytology (FNAC) or tru-cut biopsy (tru-cut Bx)is another option for suspected ALNs during diagnosis. However, it is an invasive procedure and sometimes leads the patient to the wrong treatment option due to false negatives or loss of time with repeat biopsies.3,4,5,6
Apart from nodal involvement, tumor size, hormone receptor (HR) status, and histological grade are other prognostic factors to predict the course of breast cancer, and numerous other clinicopathological factors and novel molecular markers have been investigated to improve treatment response and prognosis.7
Estrogen receptor (ER) is expressed in 50-80% of breast cancer tissues, and ER expression is the main indicator of potential response to endocrine hormone therapy (EHT). Progesterone receptor (PR) is an ER regulatory protein, and PR expression in breast cancers has been used to predict ER functionality.8 Human epidermal growth factor receptor 2 (HER2) is overexpressed or amplified in ~25% of breast cancer patients and is associated with poor clinical outcomes if not treated appropriately with HER2-targeted therapies.9
Molecular subtypes are based on ER/PR/HER2 oncogene expression and the Ki-67 index. Detecting the molecular subtype of breast cancer is important for determining the prognosis and treatment of the disease. HER2 overexpressed and triplenegative subtypes have poor prognosis, whereas luminal A and B subtypes have better prognosis.10
This study has two purposes. The primary aim is to evaluate histopathological and immunohistochemical markers that may affect ALNM. The second aim of the study is the diagnostic value of axillary ultrasonography (AUS), magnetic resonance imaging (MRI), and 18F-fluorodeoxyglucose-positron emission tomography/computed tomography (18F-FDG-PET/ CT) in determining the status of axillary lymph nodes. May immunohistopathological features of the tumor affect the diagnostic values of imaging methods?
Materials and Methods
Patients diagnosed with breast cancer treated at our hospital between January 2016 and June 2021 were evaluated retrospectively. After anamnesis and physical examination, patients who applied to our clinic with breast complaints were screened with breast and axillary ultrasonography under 40 years of age and mammography and breast and axillary ultrasonography over 40 years of age. In the daily practice of our clinic, AUS is routinely performed together with breast ultrasonography (USG) for the evaluation of axillary lymph nodes. Breast MRI was added to imaging modalities of highrisk patients. USG-guided tru-cut biopsy was performed from suspicious masses detected in the breast in imaging methods, and USG-guided FNAC or tru-cut biopsy was performed from suspicious lymph nodes. According to the pathology results, patients diagnosed with breast cancer underwent breast MRI to evaluate multicentric foci, contralateral breast and axillary lymph nodes, and 18F-FDG-PET/CT to search for distant metastases.
The imaging of breast cancer patients at the time of initial diagnosis was included in the study. AUS, breast MRI, and PETCT images of these patients at the initial diagnosis stage were examined. The patients were divided into two groups, those with and without axillary lymph node metastasis, based on the status of axillary metastases with Tru-cut Bx & FNAC or preoperative SLNB/axillary dissection. The effects of age, sex, menopausal status, tumor histology, tumor size, histological grade, multicentricity, lymphovascular invasion, perineural invasion, ER, PR, HER2, Ki67 status, and molecular subtype were evaluated in both groups.
The molecular type was performed as follows: luminal A (ER+ or PR+ and HER2-), luminal B (ER+ or PR+ and HER2+), and HER2 -amplified (ER- and PR- and HER2+). A tumor is defined as triple-negative when it is negative for all three of the ER, PR, and HER2.7
Patients with distant metastases at the time of diagnosis were not included in the study, and post-neoadjuvant imaging of patients who received neoadjuvant chemotherapy was not included.
We analyzed our patient series’ histopathological and immunohistochemical data that may affect the axillary lymph node metastasis. Secondly, to more accurately detect axillary lymph node status at the time of diagnosis, we tried to identify histopathological and immunohistochemical markers that affect the reliability and correct positivity/ negativity rates of AUS, MRI, 18F-FDG-PET/CT.
Ethical ApprovalThis study was approved by the Ethics Committee of Kanuni Sultan Süleyman Training and Research Hospital (Date: 12.08.2021, Decision No: KAEK/2021.08.237).
Statistical AnalysisSPSS (Statistical Package for Social Sciences) version 21.0 was used to analyze data. Categorical data are presented as frequency (percentage), and continuous data are presented as mean ± standard deviation. The Chi-square test or Fisher’s exact test was done for categorical data, and continuous variables were compared using an unpaired t-test. Logistic regression was used to identify the independent predictors of axillary lymph node metastasis. A Bonferroni correction and Tukey test were used to compare quantitative variables that did not show a normal distribution between more than two groups. The Pearson correlation coefficient method was used for correlations. Diagnostic screening tests, including sensitivity, specificity, positive predicted value (PPV), negative predicted value (NPV), and kappa compliance tests, were used to determine the compatibility between qualitative data. The statistical significance level was at 95% confidence intervals, and p<0.05 was considered significant. Patients with missing data were excluded from corresponding analyses.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
Patient and tumor characteristics classified by ALNM status are presented in Table 1. The study included 417 patients diagnosed and treated in our clinic. The mean age of the patients was 54.7±12.8 y. Of the patients, 413 (99%) were female, and 4 (1%) were male. Histopathologically, ALNM was negative in 168(40.3%) patients, and ALNM was positive in 249 (59.7%) patients. Based on the menopausal status, ALNM positivity was found to be higher in the premenopausal patient group, and it was statistically significant (p=0.012). When we examined for tumor histology, lymph node positivity was found to be 65.7% in invasive ductal carcinoma patients, 69% in invasive lobular carcinoma patients, and 42.3% in other histological types, which was statistically significant (p<0.001). Lymph node metastasis was found in 50.3% of the patients in the group with negative lymphovascular invasion and 74.4% of the patients in the group with positive lymphovascular invasion. It was statistically significant (p<0.001). When evaluated according to perineural invasion, ALNM positivity was detected in 64.2% of the patients in the group with negative perineural invasion and 72.1% of the patients in the group with positive perineural invasion, and it was statistically significant (p<0.001). In our study group, it was concluded that patient age, gender, tumor size, histological grade, and tumor multisencentricity did not affect lymph node metastasis, and statistically significant results could not be reached in these parameters. The relationship of immunohistochemical markers with axillary lymph node metastasis is given in Table 1. In our study, the effect of ER, PR, HER2, Ki67, and molecular type on axillary lymph node metastasis was not found to be statistically significant.
The diagnostic performance of imaging methods in detecting axillary lymph node metastases is given in Table 2.
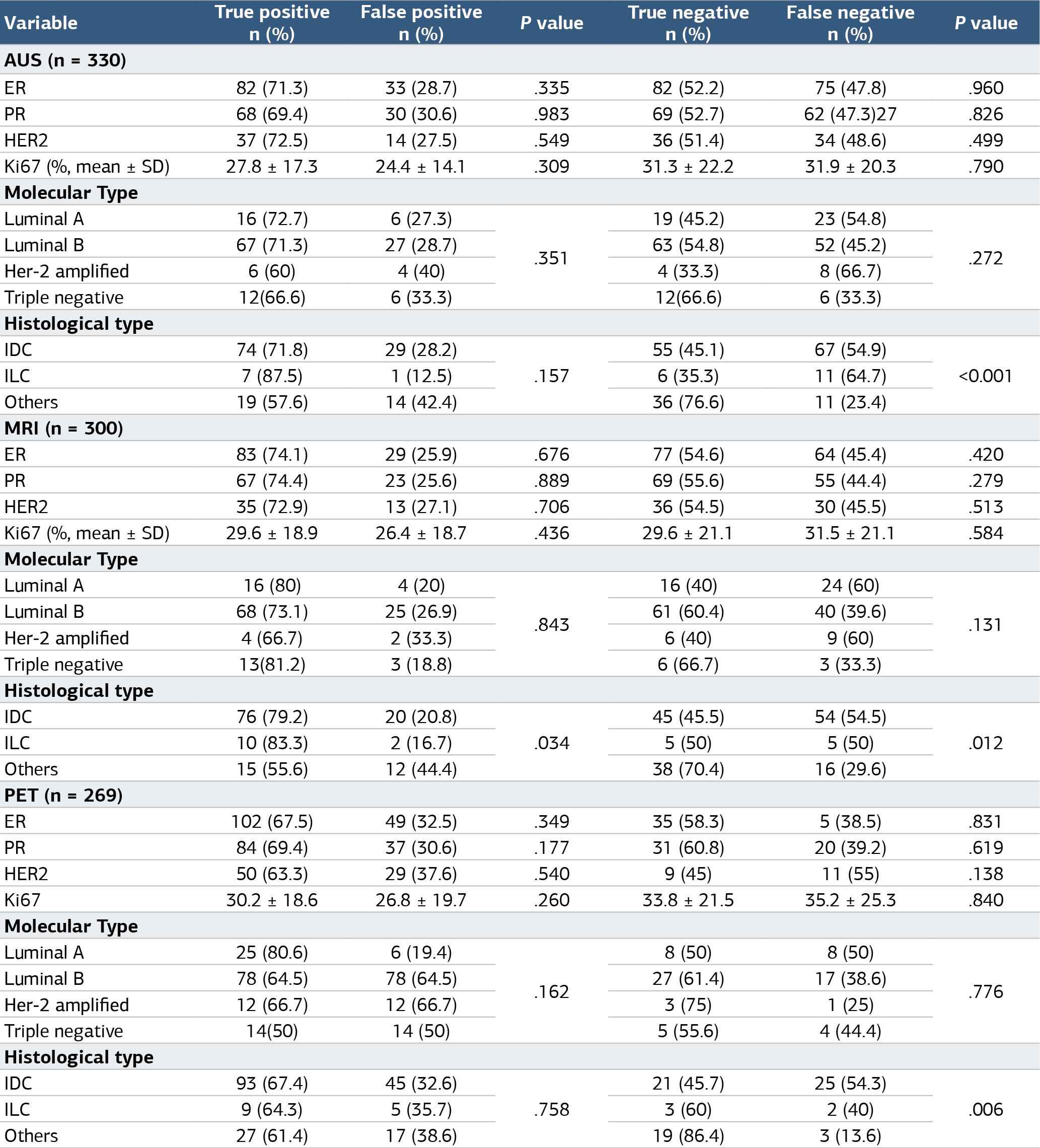
The relationships between imaging modalities and tumor immunohistochemical features and luminal subtypes are given in Table 3. When three imaging modalities (AUS, MRI, 18F-FDGPET/CT) were examined, it was found that only the histological type of the tumor statistically significantly affected true positivity, false positivity, true negativity, and false negativity. True positivity rates in AUS are 71.8% in IDC, 87.5% in ILC, and 57.6% in other histological types. True negativity rates in ultrasonography are 45.1% in invasive ductal carcinoma (IDC), 35.3% in invasive lobular carcinoma, and 76.6% in other histological types (p<0.001). True positivity rates in MRI are 79.2% in IDC, 83.3% in ILC, and 55.6% in other histological types. True negativity rates are 45.5% in IDC, 50% in ILC, and 70.4% in other histological types (p=0.012). If it is 18F-FDGPET/CT, true negativity rates are 45.7% in IDC, 60% in ILC, and 86.4% in other histological types (p=0.006). No statistically significant correlation was found between true/false positivity and true/false negativity of all three imaging methods and ER, PR, HER2, Ki67, and molecular types.
Discussion
In breast cancer, the status of the lymph nodes is the most substantial independent prognostic factor and is decisive in determining the treatment modality at the time of diagnosis.11 Neoadjuvant therapy facilitates breast-conserving surgery by reducing the tumor burden, protecting the axilla, and determining the response to systemic therapy before surgery.12
There is an opinion that breast cancer has a worse prognostic profile in younger and premenopausal women than in postmenopausal women. Multivariate analyses to evaluate the association of age and menopausal status with other clinical and pathological features (high histological grade and high tumor proliferation, lack of steroid hormone receptors) did not consider either variable an independent adverse prognostic factor.13,14 However, several studies have shown younger age or premenopausal status as independent predictors of disease recurrence.15 According to our study, premenopausal status was found to be a risk factor for increasing lymph node metastasis in breast cancer, but age could not be shown to affect ALNM positivity.
Viale et al. studied data from 4351 patients and found other histological types have a significantly lower risk of axillary lymph node metastasis than IDC.16 Similarly, a lower frequency of axillary nodal metastasis in ILC than in IDC has been reported in several studies.17 In our patient series, it was concluded that IDC and ILC have a higher tendency to metastasize to axillary lymph nodes compared to other breast cancers.
Hasebe et al. reported in two series that LVI was the strongest independent predictor of nodal involvement, and the grading system for lymph vessel tumor embolism was a very useful histological grading system for accurately predicting lymph node metastasis in IDC.18,19 Duraker et al. found that PNI is more likely in hormone-sensitive, mixed-type, or ductal carcinoma and less likely in axilla-negative or smaller tumors.20 Another study found that PNI predicted >3 lymph node involvement.21 Based on our results, lymphovascular invasion, and perineural invasion positivity increase the risk of ALNM. The neoadjuvant systemic therapy method is decided according to the molecular subtype determined concerning ER, PR, HER2, and Ki-67 status. They are also used to predict the prognosis of breast cancer patients.13 We evaluated our patient series’ effects of ER, PR, HER2, Ki-67, and molecular subtypes on nodal metastasis; we concluded that none had a statistically significant effect on lymph node metastasis.
Radiologic evaluation of ALN is done with AUS, MRI, and 18F-FDG-PET/CT. AUS is an easy-to-apply, inexpensive, nonradiation-free, non-invasive method used to assess lymph nodes in breast cancer.4 Besides being non-invasive and radiationfree, breast MRI has advantages such as giving anatomical information about the condition of the breast and axilla and showing lesions that ultrasound and mammography cannot detect.5,22,23 On the other hand, 18F-FDG-PET/CT used for distant metastasis screening is expensive, contains isotopic radiation, has high false-positive rates in inflammation, and has low sensitivity for detecting nodal micrometastases.4,5
When Aktaş et al. evaluated sensitivity, PPV, and accuracy to accurately detect the presence of axillary metastases, they found the order of reliability as MRI, AUS, and 18F-FDG-PET/ CT.24 Although there was no significant difference in our study, MRI was the most reliable, followed by 18F-FDG-PET/ CT and AUS. When the specificity, NPV, and accuracy rates are examined, the order of reliability in estimating axilla negativity is again MRI, 18F-FDG-PET/CT, and AUS.
In addition, it was concluded in our study that only the histological tumor type can be considered in the radiologically correct prediction of axillary lymph node metastasis in breast cancer, and other immune histochemical markers do not have a beneficial effect in this regard.
If the tumor type is IDC or ILC, breast MRI and AUS may be superior to predict axilla positivity. However, the reliability of AUS, breast MRI, and 18F-FDG-PET/CT in predicting axilla negativity may be low in these two tumor types.
In other tumor types, while AUS, breast MRI, and 18F-FDGPET/CT may be superior in predicting negative axilla, their reliability may be low in predicting axillary metastasis positivity.
Limitations
Limitations of our study: being a retrospective study, we could not reach the AUS, MRI, or 18F-FDG-PET/CT of each patient because imaging data were obtained in different imaging centers in some patients, and AUS is an operator-dependent modality.
Conclusion
The conclusions to be drawn from our study: premenopausal status, tumor histology being invasive ductal/lobular carcinoma, and the presence of lymphovascular invasion or perineural invasion are factors that increase the risk of axillary lymph node metastasis in breast cancer. Although there is no substantial superiority between them, MRI is the most reliable radiological method to accurately predict axillary lymph node metastasis in breast cancer, followed by 18F-FDG-PET/CT and AUS, respectively. When the relationship between the histopathological and immunohistochemical markers of the tumor and imaging methods was evaluated, If tumor types are IDC and ILC, AUS and breast MR may be superior in predicting axillary metastasis positivity. In the other tumor types, AUS, breast MRI, and 18F-FDG-PET/CT may be reliable in accurately predicting axilla negativity in all three imaging modalities.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants and their caregivers prior to inclusion in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
18F-FDG-PET/CT: 18F-fluorodeoxyglucose positron emission tomography/computed tomography
ALN: Axillary lymph node
ALNM: Axillary lymph node metastasis
AUS: Axillary ultrasonography
FNAC: Fine-needle aspiration cytology
HER2: Human epidermal growth factor receptor 2
IDC: Invasive ductal carcinoma
ILC: Invasive lobular carcinoma
LVI: Lymphovascular invasion
PNI: Perineural invasion
SLNB: Sentinel lymph node biopsy
STROBE: Strengthening the Reporting of Observational Studies in Epidemiology
References
-
Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249. doi:10.3322/caac.21660
-
Cronin KA, Scott S, Firth AU, et al. Annual report to the nation on the status of cancer, part 1: national cancer statistics. Cancer. 2022;128(24):4251-4284. doi:10.1002/cncr.34479
-
Sohn YM, Hong IK, Han K. Role of [18F]fluorodeoxyglucose positron emission tomography-computed tomography, sonography, and sonographically guided fine-needle aspiration biopsy in the diagnosis of axillary lymph nodes in patients with breast cancer: comparison of diagnostic performance. J Ultrasound Med. 2014;33(6):1013-1021. doi:10.7863/ultra.33.6.1013
-
Hwang SO, Lee SW, Kim HJ, Kim WW, Park HY, Jung JH. The comparative study of ultrasonography, contrast-enhanced MRI, and 18F-FDG PET/CT for detecting axillary lymph node metastasis in T1 breast cancer. J Breast Cancer. 2013;16(3):315-321. doi:10.4048/jbc.2013.16.3.315
-
Marino MA, Avendano D, Zapata P, Riedl CC, Pinker K. Lymph node imaging in patients with primary breast cancer: concurrent diagnostic tools. Oncologist. 2020;25(2). doi:10.1634/theoncologist.2019-0427
-
Ahn HS, Jang M, Kim SM, La Yun B, Lee SH. Usefulness of preoperative breast magnetic resonance imaging with a dedicated axillary sequence for the detection of axillary lymph node metastasis in patients with early ductal breast cancer. Radiol Med. 2019;124(12):1220-1228. doi:10.1007/s11547-019-01072-2
-
Yenidunya S, Bayrak R, Haltas H. Predictive value of pathological and immunohistochemical parameters for axillary lymph node metastasis in breast carcinoma. Diagn Pathol. 2011;6:18. doi:10.1186/1746-1596-6-18
-
Gompel A. Hormones et cancers du sein [Hormone and breast cancer]. Presse Med. 2019;48(10):1085-1091. doi:10.1016/j.lpm.2019.09.021
-
Miglioretti DL, Zhu W, Kerlikowske K, et al. Breast tumor prognostic characteristics and biennial vs annual mammography, age, and menopausal status. JAMA Oncol. 2015;1(8):1069-1077. doi:10.1001/jamaoncol.2015.3084
-
Zhang J, Jia Z, Zhou M, et al. The SUVmax for 18F-FDG correlates with molecular subtype and survival of previously untreated metastatic breast cancer. Clin Nucl Med. 2013;38(4):256-262. doi:10.1097/rlu.0b013e3182816318
-
Fisher ER, Costantino J, Fisher B, Redmond C. Pathologic findings from the National Surgical Adjuvant Breast Project Protocol 4: discriminants for 15-year survival. Cancer. 1993;71(6):2141-2150.
-
Jeong YS, Kang J, Lee J, Yoo TK, Kim SH, Lee A. Analysis of the molecular subtypes of preoperative core needle biopsy and surgical specimens in invasive breast cancer. J Pathol Transl Med. 2020;54(1):87-94. doi:10.4132/jptm.2019.10.14
-
Zhu JW, Charkhchi P, Adekunte S, Akbari MR. What is known about breast cancer in young women? Cancers (Basel). 2023;15(6):1917. doi:10.3390/cancers15061917
-
El Saghir NS, Seoud M, Khalil MK, et al. Effects of young age at presentation on survival in breast cancer. BMC Cancer. 2006;6:194. doi:10.1186/1471-2407-6-194
-
Lyman GH, Kuderer NM, Lyman SL, et al. Menopausal status and the impact of early recurrence on breast cancer survival. Cancer Control. 1997;4(4):335-341. doi:10.1177/107327489700400405
-
Viale G, Zurrida S, Maiorano E, et al. Predicting the status of axillary sentinel lymph nodes in 4351 patients with invasive breast carcinoma treated in a single institution. Cancer. 2005;103(3):492-500. doi:10.1002/cncr.20809
-
Toikkanen S, Pylkkänen L, Joensuu H. Invasive lobular carcinoma of the breast has better short- and long-term survival than invasive ductal carcinoma. Br J Cancer. 1997;76(9):1234-1240. doi:10.1038/bjc.1997.540
-
Hasebe T, Okada N, Iwasaki M, et al. Grading system for lymph vessel tumor emboli: significant outcome predictor for invasive ductal carcinoma of the breast. Hum Pathol. 2010;41(5):706-715. doi:10.1016/j.humpath.2009.10.015
-
Hasebe T, Tamura N, Iwasaki M, et al. Grading system for lymph vessel tumor emboli: significant outcome predictor for patients with invasive ductal carcinoma of the breast who received neoadjuvant therapy. Mod Pathol. 2010;23(4):581-592. doi:10.1038/modpathol.2010.3
-
Duraker N, Caynak ZC, Turkoz K. Perineural invasion has no prognostic value in patients with invasive breast carcinoma. Breast. 2006;15(5):629-634. doi:10.1016/j.breast.2005.12.003
-
Hadi NI, Jamal Q. Comparison of clinicopathological characteristics of lymph node-positive and lymph node-negative breast cancer. Pak J Med Sci. 2016;32(4):863-868. doi:10.12669/pjms.324.10324
-
Chayakulkheeree J, Pungrassami D, Prueksadee J. Performance of breast magnetic resonance imaging in axillary nodal staging in newly diagnosed breast cancer patients. Pol J Radiol. 2019;84. doi:10.5114/pjr.2019.89690
-
Arslan G, Altintoprak KM, Yirgin IK, Atasoy MM, Celik L. Diagnostic accuracy of metastatic axillary lymph nodes in breast MRI. Springerplus. 2016;5(1):735. doi:10.1186/s40064-016-2419-7
-
Aktaş A, Gürleyik MG, Aydın Aksu S, Aker F, Güngör S. Diagnostic value of axillary ultrasound, MRI, and 18F-FDG PET/CT in determining axillary lymph node status in breast cancer patients. Eur J Breast Health. 2021;18(1):37-47.
Tables
Table 1. Patient and tumor characteristics classified by ALNM status are presented
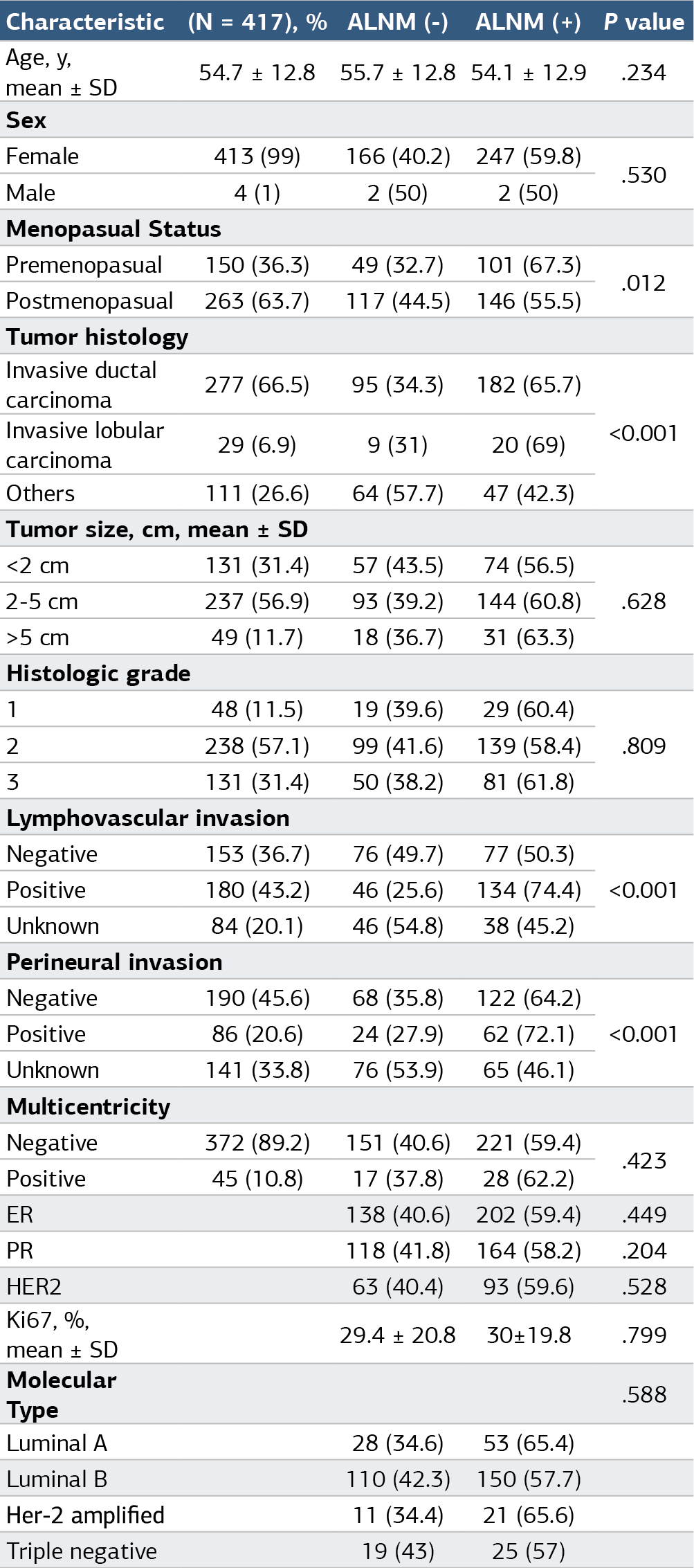
ALNM: Axillary lymph node metastasis, ER: Estrogen receptor, PR: Progesterone receptor.
Table 2. The diagnostic performance of imaging methods in detecting axillary lymph node metastases

The sensitivity, specificity, PPV, NPV, and accuracy of AUS for detecting ALN metastases were 59.9%, 62.7%, 69.4%, 51.5%, and 60.5%, respectively. For MRI, these values were 61.9%, 67.9%, 73.6%, 55.4%, and 64.4%, respectively, and for 18F-FDG-PET/CT, they were 61.8%, 63.4%, 70.8%, 53.5%, and 62.4%, respectively.
Table 3. The relationships between imaging modalities and tumor immunohistochemical features and luminal subtypes
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Tansu Altintas, Naciye Cigdem Arslan. Immunohistochemical markers affecting nodal metastasis in breast cancerand imaging methods for detection of axillary lymph node metastasis. Ann Clin Anal Med 2025;16(3):171-176. doi:10.4328/ACAM.22517
- Received:
- December 5, 2024
- Accepted:
- January 23, 2025
- Published Online:
- February 7, 2025
- Printed:
- March 1, 2025