
The importance of the levels of autotaxin and lysophosphatidic acid levels for patients with colon cancer
ATX and LPA in colon cancer patients
Authors
Abstract
Aim Whether plasma levels of autotaxin (ATX) and lysophosphatidate (LPA) could be distributed to diagnostic biomarkers for colon cancer is ill-defined. In our
study, we appraised the possibility of plasma LPA and ATX as cancer biomarkers.
Methods A total of 90 patients hospitalized at the general surgery clinic with the diagnosis of colon cancer were included in the study. The control group consisted of 50 healthy individuals who had no known disease. There were 30 cases of early-stage (I/II), 50 cases of late-stage (III-IV) colon cancer, and 50 cases of lymph node metastasis (N1/N2).
Results Preoperative serum ATX levels were higher in patients with colon cancer according to the healthy control group (p<0.001). Preoperative serum LPA levels were higher in patients with colon cancer (56.2±13.06 ng/mL, median: 62 ng/mL, range 23-69.6 ng/mL) according to the healthy control group (8.77±2.3 ng/mL, median: 9 ng/mL, range 4-12 ng/mL) (p<0.001). The concentration of ATX in the preoperative serum of the patients with Stage T4 (298.57 ± 19.7 ng/L, median 300 ng/L, with a range of 20-330 ng/L) was significantly higher compared to patients with Stages T1, T2, and T3. The levels of ATX in the serum of the patients with T3 (219.41 ± 19.7 ng/L, median 200 ng/L, with a range of 180-250 ng/L) were significantly higher compared to the patients with Stages T1 and T2.
Conclusion It appears that our analysis of ATX is to be a useful prognostic marker to predict the survival of patients with colon cancer, along with their response to dissimilar therapeutic agents.
Keywords
Introduction
Although there has been a large number of studies on colon cancer, it remains one of the leading types of cancer that results in death both in men and women worldwide.1 Today, colon cancer is the third and second most commonly diagnosed cancer in males and females, respectively.2 It causes approximately 800,000 deaths each year globally.3 According to the latest epidemiological database, there were more than 1.9 million new colon cancer cases and 0.9 million deaths in 2020.4 This heavy public health burden is estimated to increase if no improvement in early detection and effective interventions for late-stage colon cancer are discovered.5 The increasing incidence in some countries is a result of lifestyle changes such as obesity, physical inactivity, excessive alcohol consumption, smoking, and high red meat intake.6 Family history of disease and increasing age are the other factors affecting the development of colon cancer.
The diagnosis and treatment of colon cancer are considered social and economic challenges due to high mortality rates. Despite the rapidly developed cancer screening methods, many patients are diagnosed at an advanced stage. Current pathophysiological evaluation, treatment decisions, and prognostic predictions for colon cancer mainly rely on factors such as TNM staging and molecular markers.7 Several biomarkers have been used in predicting the diagnosis and prognosis of colon cancer. Among these biomarkers, carcinoembryonic antigen (CEA) greater than five ng/mL indicates a poor prognosis, but its sensitivity (46%) is low. Carbohydrate antigen (CA19-9) is a cancer antigen whose elevated serum levels are detected in case of colon cancer. It is a tumor biomarker that is observed in elevated serum concentration with metastatic colon cancer. However, its sensitivity is also low. In addition, serum CA19-9 can be found in both benign and malignant processes.8 It is necessary to identify new indicators for the evaluation of prognosis and targeted therapy of colon cancer.9
Autotaxin (ATX) is a secreted lysophospholipase D that produces most of the extracellular lysophosphatidate (LPA) from hydrolysis of choline from lysophosphatidylcholine (LPC).10 ATX was described for the first time as an “autocrine motility factor” found in the cell culture medium of melanoma cells in 1992.11 Later work in 1995 revealed that LPA among lysophospholipids could exert cell signaling events through unique receptors in breast cancer and thus could be a potential target for therapy.12 Subsequent studies have shown that LPA has the capability of merging intrinsic oncogenic activation and extrinsic inflammatory pathways to sustain cell proliferation and promote cell survival, invasion, and metastasis.13,14 However, despite the increasing evidence associating ATX with cancer, direct evidence suggesting ATX as a potential therapeutic target for colon cancer is lacking. Therefore, the objective of this study was to investigate the diagnostic and prognostic value of ATX and LPA in patients with colon cancer.14
Materials and Methods
A total of 90 patients hospitalized at the general surgery clinic with the diagnosis of colon cancer were included in the study. The control group consisted of 50 healthy individuals who had no known disease. There were 30 cases of early-stage (I/II), 50 cases of late-stage (III-IV) colon cancer, and 50 cases of lymph node metastasis (N1/N2).
Determination of ATX and LPA LevelsA total of 10 mL venous blood was collected from each participant into sterile vacutainers preoperatively. The samples were centrifuged at 3500 g for 10 min, and serum parts were separated and stored at -80oC until the analysis. The serum samples were then warmed before measurement of ATX and LPA blood levels. Serum levels of ATX (MyBiosource; Catalog no: MBS167516; Sensitivity: 4.65 ng/L; Detection range: 10- 3000 ng/L) and LPA (MyBiosource; Catalog no: MBS707269; Sensitivity: <3.9 ng/mL; detection range: 3.9-250 ng/mL) were assayed by enzyme-linked immunosorbent assay (ELISA) and determined by production from a standard curve produced using known extents of each protein. The samples were serially diluted with phosphate-buffered saline (PBS) and assessed again to ensure that the concentrations were within measurable ranks. The researchers were blinded to sample origins, and all tests were performed in triplicate following the manufacturer’s instructions.
Ethical ApprovalThis study was approved by the Ethics Committee of Van Yuzuncu Yil University (Date: 2022-11-18, No: 2022/11-2).
Statistical AnalysisNormality was checked by using Shapiro Wilk and single-sample Kolmogorov Smirnov tests, histogram, Q-Q plot, and box plot graphs. The variables are expressed as median, minimum, maximum, frequency, and percentage. Bi-category variables were analyzed with the Mann-Whitney U test. Variables with three or more categories were compared with Kruskal Wallis’s one-way analysis of variance. Multiple comparisons were made with Dunn’s test. Nominal variables were evaluated with the Chi-square test. The correlation between the variables was evaluated using Spearman’s correlation test. p<0.05 values were considered statistically significant. The statistical analysis was performed using the NCSS 10 (2015. Kaysville, Utah, USA) software.
Reporting GuidelinesThe study was reported in accordance with STROBE.
Results
The patient group consisted of 43 males and 47 females, with ages ranging from 50 to 70 years (60.42 ± 5.30 years). The control group consisted of 43 males and 47 females, with ages ranging from 53 to 70 years (mean: 62.46 ± 4.29 years). No statistically significant difference was found between the patient and control groups in terms of age and gender (both p>0.05) (Figure 1).
Preoperative serum ATX levels were statistically significantly higher in patients with colon cancer (221.04 ± 84.24 ng/mL, median: 250 ng/mL, range 90-330 ng/mL) compared to the healthy control group (16.2 ± 1.94 ng/mL, median: 16 ng/mL, range 12-20 ng/mL) (p<0.001). Preoperative serum LPA levels were higher in patients with colon cancer (56.2 ± 13.06 ng/mL, median: 62 ng/mL, range 23-69.6 ng/mL) compared to the healthy control group (8.77 ± 2.3 ng/mL, median: 9 ng/mL, range 4-12 ng/mL) (p<0.001). Figure 2 shows the preoperative serum ATX and LPA comparison between the groups.
The concentration of ATX in the preoperative serum of the patients with Stage T4 (298.57 ± 19.7 ng/L, median 300 ng/L, with a range of 250-330 ng/L) was significantly higher compared to the patients with Stages TI, T2, and T3 (Table 1). Also, the levels of ATX in the serum of the patients with Stage T3 (219.41 ± 19.7 ng/L, median 200 ng/L, with a range of 180- 250 ng/L) were significantly higher compared to the patients with Stages TI and T2 (both, p<0.001) (Table 1).
The levels of ATX in the preoperative serum of the patients with N2 (275.76 ± 18.79 ng/L, median 280 ng/L, with a range of 10- 330 ng/L) were statistically significantly higher compared to the patients with N0 and N1 (p<0.001). We found no difference between N0 and N1 in terms of ATX values (p>0.05) (Table 1). The concentrations of ATX in the preoperative serum of the patients with M1 (242.64 70.96 ng/L, median 280 ng/L, with a range of 110-330 ng/L) were statistically significantly higher compared to the patients with M0 (p<0.001) (Table 1).
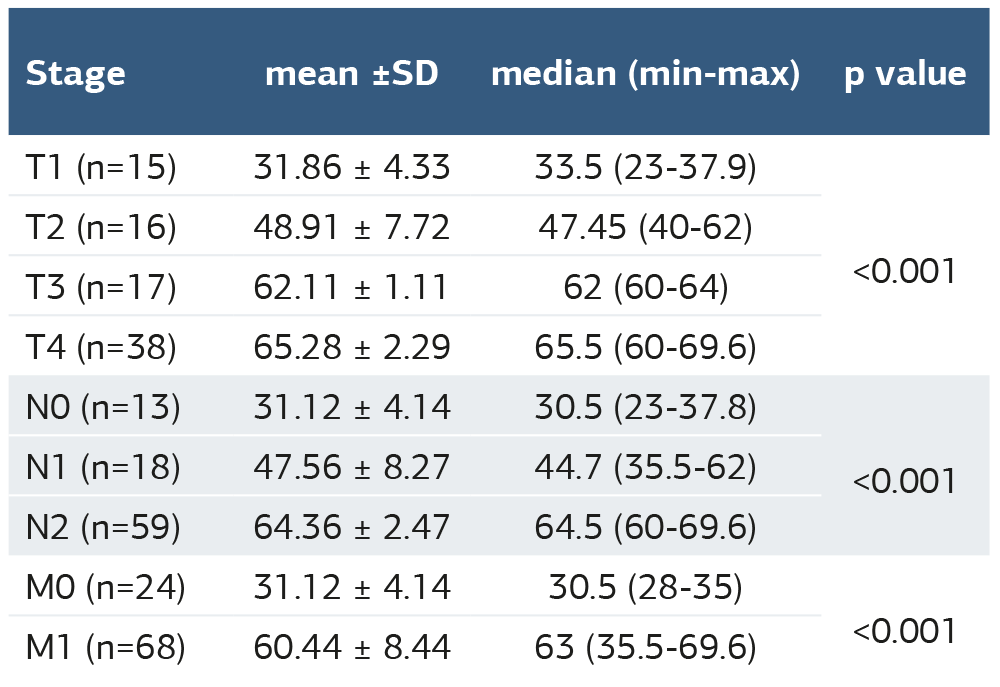
The concentration of LPA in the preoperative serum of the patients with Stage T4 (65.28 ± 2.29 ng/mL, median 65.5 ng/mL, with a range of 60-69.6 ng/mL) was significantly higher compared to the patients with Stages T1, T2 and T3 (p<0.001) (Table 2). Also, the levels of LPA in the serum of the patients with Stage T3 (62.11 ± 1.11 ng/mL, median 62 ng/mL, with a range of 60-69.6 ng/mL) were statistically significantly higher compared to the patients with Stages T1 and T2 (both, p<0.001) (Table 2).
The levels of LPA in the preoperative serum of the patients with N2 (64.36 ± 002.47 ng/mL, median 64.5 ng/mL, with a range of 60-69.6 ng/mL) were significantly higher compared to the patients with N0 and N1 (both, p<0.001). We found no difference between N0 and N1 (p>0.05) (Table 2).
The concentrations of LPA in the preoperative serum of the patients with M1 (60.44 8.44 ng/mL, median 63 ng/mL, with a range of 35.5-69.6 ng/mL) were higher compared to the patients with M0 (p<0.001) (Table 2).
When the relationship between ATX and LPA was examined, no significant correlation was found in the control group (r=0.22; p=0.12). However, there was a strong correlation in the same direction between ATX and LPA in the patient groups (r=0.85; p<0.001) (Figure 3).
Discussion
In this study, we investigated the diagnostic and prognostic value of ATX and LPA. We found that preoperative serum levels of both ATX and LPA were statistically significantly higher in the patients with colon cancer compared to the controls.
Many tumor markers are commonly used to evaluate diagnosis, treatment, and prognosis. Relevant studies have shown that the levels of tumor biomarkers can be modulated before and after treatment, but its specific mechanism is yet to be elucidated. Colon cancer, a strain of malignant tumor in the sustaining canal, has a higher incidence and mortality. Metastasis is the leading cause of high mortality in colon cancer patients.15
A non-normally powerful expression of the ATX has been characteristically observed by ELISA. ATX is over-expressed in response to DNA double-bond breaks secondary to oxidative stresses in cancer cells. The ATM-ATX-dependent coil advance propagates inflammation and extra double bond breaks, leading to the overproduction of ATX.16 In a study, post-transcriptional regulation of ATX proved that the RNA-binding proteins improve ATX mRNA stability in melanoma cells and thence raise ATX production.17 Some studies reported that ATX is upregulated in thyroid cancer in response to prolonged autocrine-induced inflammation, and this can discriminate cancer from benign disease.18 Nevertheless, breast cancer cells secrete little ATX resembling the basal rank from breast adipose tissue. Therefore, LPA rises within the tumor microenvironment and validates a cruel coil of inflammatory-driven ATX production since LPA evaluates the production of great inflammatory cytokines and COX-2. Likewise, tumor-induced inflammation in mammary adipose tissue raises macrophage enlisting, which persuades it to advance inflammation and ATX production.19 Elevated serum ATX activity was virtually major for cancer in an assessment of serum ATX levels in a legion of gastrointestinal cancers implicating cancers of the esophagus, stomach, biliary tract, and pancreas.20
In our study, we showed that these markers are mediated by cancer stem cells, which in colon cancer construct plentiful ATX, and they express high levels of LPA. A new study has enlarged our knowledge of LPA biology in cancer. The transcriptional factor NFAT1 has a role in both natural and adaptable immune responses and enhances metastatic possibility by immediately upregulating IL-8 and MMP-3. This is secondary to autocrine ATX production and LPA signaling.21 LPA had very important metastasis, representing the major role of LPA signaling in confirming an admissible environment for cancer cell scattering.22 Because LPA is the enzymatic by-product of ATX activity, it is sensible to regard the ATX-LPA axis as a mediator of systemic immune activation.23 Pathways of the ATX-LPA and oxidative stress are probably retained. ATX is highly expressed during oxidative stress, virtually combining with the grade of tumor aggressiveness. Concentrations of ATX are usually conjoining with levels of the ATX enzymatic activity product LPA, a lipid mediator that signals through LPA receptors. Since systemic immune activation is assortative of morbidity and mortality during inflammation, and since ATX-LPA signaling furnishes immune activation, advanced searches of the relationship between ATX-LPA signaling and morbidity during tumor invasions are approved.
Limitations
The major limitations of this study include being conducted in a single center and relatively small number of patients. In addition, since there is no similar study in the literature, we could not compare our results with previous studies exactly. We believe that our findings will be guiding for future comprehensive studies.
Conclusion
We demonstrated that the over expression of the ATX is associated with advanced grades of colon cancer as well as an increasing TNM stage. This phenomenon could be created via different signaling pathways and finally administered to cancer cell proliferation. It appears that our analysis of ATX could be a useful prognostic marker to predict the survival of patients with colon cancer, along with their response to dissimilar therapeutic agents. Further studies are needed to enlighten the specific role of this enzyme in the advancement of colon cancer.
Declarations
Ethics Declarations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and its later amendments. All procedures involving human participants complied with institutional and national research committee standards. The study protocol was reviewed and approved by the Ethics Committee of Van Yuzuncu Yil University (Date: 2022-11-18; No: 2022/11-2).
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants prior to inclusion in the study.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: E.E., R.K.
Methodology: E.E., S.A.
Investigation: E.E., R.K., O.K., E.A.
Data curation: E.E., S.A.
Formal analysis: S.A.
Writing – original draft: E.E.
Writing – review & editing: R.K., O.K., E.A.
Supervision: E.E.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of this article, including study design, data collection, analysis and interpretation, and manuscript preparation and final approval.
Abbreviations
ATX: Autotaxin
CA19-9: Carbohydrate antigen 19-9
CEA: Carcinoembryonic antigen
ELISA: Enzyme-linked immunosorbent assay
LPA: Lysophosphatidic acid
LPC: Lysophosphatidylcholine
PBS: Phosphate-buffered saline
TNM: Tumor–node–metastasis
References
-
Gupta R, Bhatt LK, Johnston TP, Prabhavalkar KS. Colon cancer stem cells: Potential target for the treatment of colorectal cancer. Cancer Biol Ther. 2019;20(8):1068-1082. doi: 10.1080/15384047.2019.1599660
-
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018;68(6):394–424. doi: 10.3322/caac.21492
-
Siegel RL, Miller KD, Goding Sauer A, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020;70(3):145-164.
-
Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209-249. doi: 10.3322/caac.21660
-
Kraik K, Tota M, Laska J, et al. The Role of Transforming Growth Factor-β (TGF-β) in Asthma and Chronic Obstructive Pulmonary Disease (COPD). Cells. 2024;13(15):1271.
-
Kerr J, Anderson C, Lippman SM. Physical activity, sedentary behavior, diet, and cancer: an update and emerging new evidence. Lancet Oncol. 2017;18(8): e457-e471. doi: 10.1016/S1470-2045(17)30411-4
-
Hu H, Krasinskas A, Willis J. Perspectives on current tumor-node-metastasis (TNM) staging of cancers of the colon and rectum. Semin Oncol. 2011;38(4):500- 510.
-
Lakemeyer L, Sander S, Wittau M, Henne-Bruns D, Kornmann M, Lemke J. Diagnostic and Prognostic Value of CEA and CA19-9 in Colorectal Cancer. Diseases. 2021;9(1):21.
-
Chen H, Luo J, Guo J. Development and validation of a five-immune gene prognostic risk model in colon cancer. BMC Cancer. 2020;20(1):395. doi: 10.1186/s12885-020-06799-0
-
Benesch MG, Ko YM, McMullen TP, Brindley DN. Autotaxin in the crosshairs: taking aim at cancer and other inflammatory conditions. FEBS Lett. 2014;588(16):2712-2727.
-
Stracke ML, Krutzsch HC, Unsworth EJ, et al. Identification, purification, and partial sequence analysis of autotaxin, a novel motility-stimulating protein. J Biol Chem. 1992;267(4):2524-2529.
-
Xu Y, Fang XJ, Casey G, Mills GB. Lysophospholipids activate ovarian and breast cancer cells. Biochem J. 1995;309 (Pt 3)(Pt 3):933-940.
-
Yun CC. Lysophosphatidic Acid and Autotaxin-associated Effects on the Initiation and Progression of Colorectal Cancer. Cancers (Basel). 2019;11(7):958.
-
Yu X, Zhang Y, Chen H. LPA receptor 1 mediates LPA-induced ovarian cancer metastasis: an in vitro and in vivo study. BMC Cancer. 2016;16(1):846.
-
Mlecnik B, Bindea G, Kirilovsky A, et al. The tumor microenvironment and Immunoscore are critical determinants of dissemination to distant metastasis. Sci Transl Med. 2016;8(327):327ra26.
-
Zheng H, Högberg J, Stenius U. ATM-activated autotaxin (ATX) propagates inflammation and DNA damage in lung epithelial cells: a new mode of action for silica-induced DNA damage. Carcinogenesis. 2017;38(12):1196-1206.
-
Sun S, Zhang X, Lyu L, Li X, Yao S, Zhang J. Autotaxin expression is regulated at the post-transcriptional level by the RNA-binding proteins HuR and AUF1. J Biol Chem. 2016;291(50):25823-25836.
-
Benesch MGK, MacIntyre ITK, McMullen TPW, Brindley DN. Coming of Age for Autotaxin and Lysophosphatidate Signaling: Clinical Applications for Preventing, Detecting and Targeting Tumor-Promoting Inflammation. Cancers (Basel). 2018;10(3):73.
-
Benesch MG, Ko YM, Tang X, et al. Autotaxin is an inflammatory mediator and therapeutic target in thyroid cancer. Endocr Relat Cancer. 2015;22(4):593-607.
-
Nakai Y, Ikeda H, Nakamura K, et al. Specific increase in serum autotaxin activity in patients with pancreatic cancer. Clin Biochem. 2011;44(8-9):576-581.
-
Shoshan E, Braeuer RR, Kamiya T, et al. NFAT1 Directly Regulates IL8 and MMP3 to Promote Melanoma Tumor Growth and Metastasis. Cancer Res. 2016;76(11):3145-3155.
-
Lee SC, Fujiwara Y, Tigyi GJ. Uncovering unique roles of LPA receptors in the tumor microenvironment. Receptors Clin Investig. 2015;2(1): e440.
-
Benesch MGK, Tang X, Dewald J, et al. Tumor-induced inflammation in mammary adipose tissue stimulates a vicious cycle of autotaxin expression and breast cancer progression. FASEB J. 2015;29(9):3990-4000.
Figures
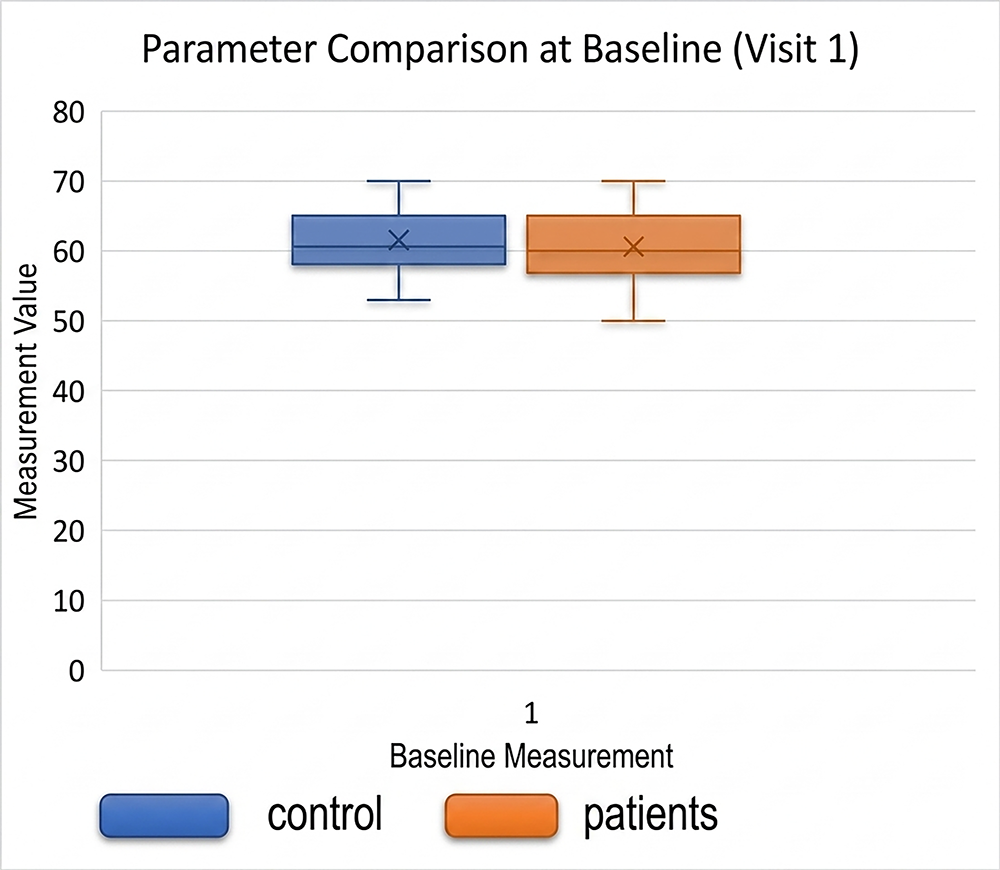
Figure 1. Age ranges of the patient and control groups
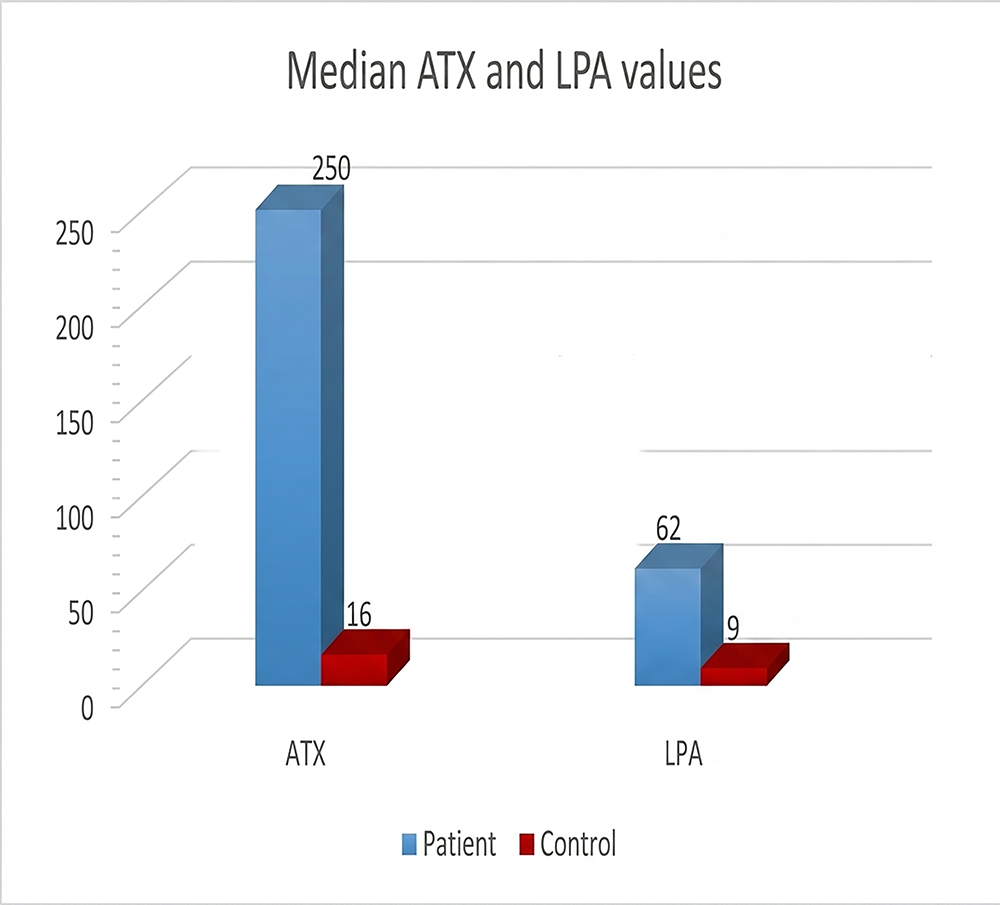
Figure 2. Median values of ATX and LPA according to the groups
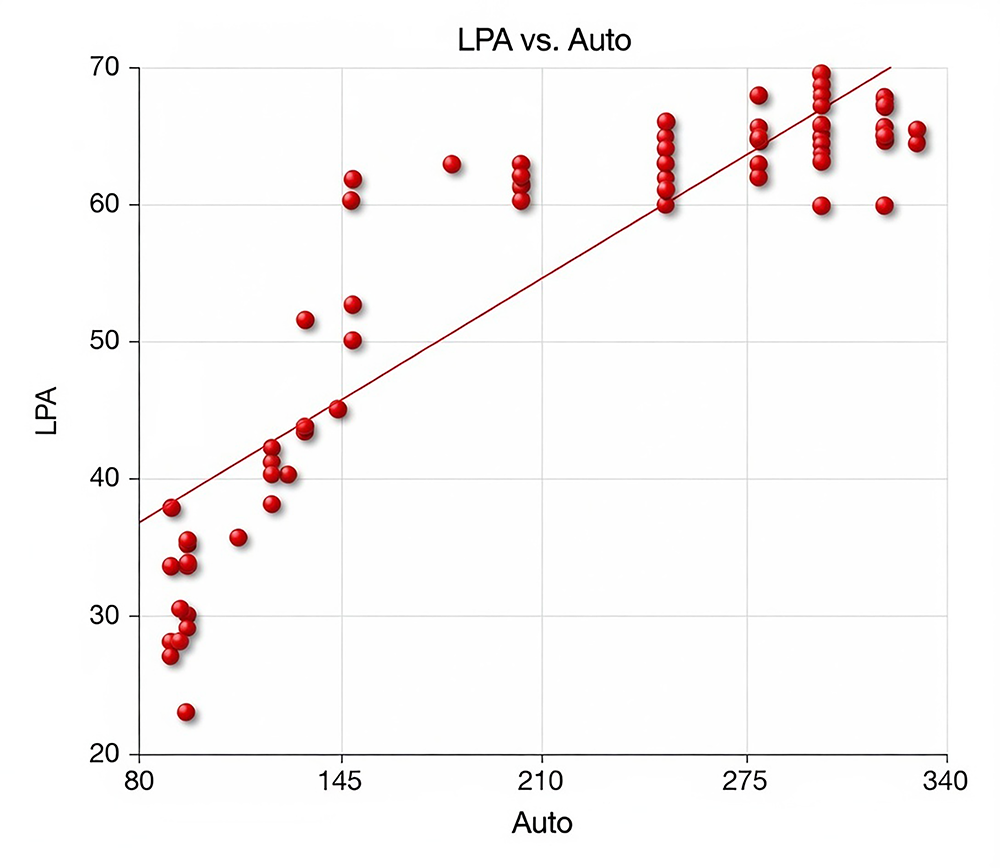
Figure 3. Correlation between ATX and LAP in the patient group
Tables
Table 1. Preoperative serum ATX values of the patient and control groups
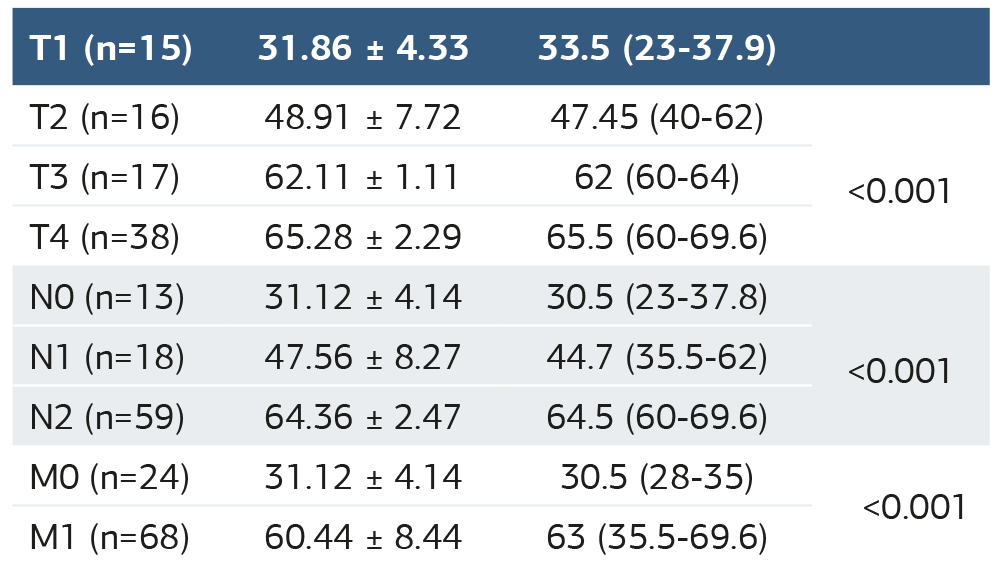
Table 2. Preoperative serum LPA values of the patient and control groups
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ersan Eroglu, Remzi Kiziltan, Sermin Algul, Ozgur Kemik, Ediz Altinli. The importance of the levels of the autotaxin and lysophosphatidic acid levels for patients with colon cancer. Ann Clin Anal Med 2026;17(Suppl 2):S99-103. doi: 10.4328/ACAM.22524
- Received:
- December 18, 2025
- Accepted:
- May 26, 2025
- Published Online:
- July 12, 2025
- Printed:
- March 20, 2026