
Comparison of pain, functional capacity, balance, and body awareness in individuals with and without fibromyalgia
Body awareness in fibromyalgia
Authors
Abstract
Aim In this study, the comparison of pain, functional capacity, balance, and body awareness in female individuals with and without fibromyalgia (FM) was
investigated.
Methods Women with (n = 33) and without fibromyalgia (n = 33) between the ages of 18-65 were included. Demographic data of the participants were recorded. The pain was evaluated with an algometer. Mobility and functional capacity were assessed with the Timed Up and Go Test (TUG) and the 6-minute walk test (6MWT). The impact of the fibromyalgia syndrome was assessed with Fibromyalgia Impact Questionnaire (FIQ). BA was assessed with the Body Awareness Questionnaire (BAQ). Balance was assessed with the Biodex Balance System (BDS). The data were analyzed with the independent sample t-test and chi-square test.
Results The mean ages of the control group and FM group were 39 ±15.84 years and 41 ±13.10 years. There was a significant difference between the two groups with respect to 6MWT, FIQ score, TUG score, and some pain variables (p < 0.05). These differences were in favor of the control group.
Conclusion In conclusion, scores of all parameters were worse in FM patients. FM has a negative impact on pain level, and FIQ score, especially on functional capacity and mobility. The pain threshold was very low. In light of these results, these parameters should be taken into consideration when evaluating and planning rehabilitation programs aimed at improving functional capacity in FM.
Keywords
Introduction
Fibromyalgia (FM) is defined as a chronic widespread pain syndrome in the musculoskeletal system. FM affects 2.7% of the world population and is the third most common musculoskeletal disease after osteoarthritis and low back pain. Additionally, it is more common in women than in men. A sign of FM is the presence of multiple tender points. Symptoms are diverse; sleep disorders, anxiety, cognitive disorders, depression, and low performance in physical activities can be seen 1.
Pain is a common disorder in FM patients. A low pain threshold and an increased pain response to stimuli are found. Moreover, FM patients also experience balance dysfunction, and decreased muscle strength with low functional capacity 2. Balance dysfunction and physical impairment increase the fall risk and disability. Recent studies have found that patients with musculoskeletal disorders had lower BA. BA has a significant impact on the quality of life of FM patients. Patients with FM have a disruption of body image 3. This condition affects function, social life, and balance, and leads to limitations in daily activities. Decreased BA may affect functional capacity, balance, and pain in patients with FM 4.
Knowledge of pain, functional capacity, balance, and body awareness in those with and without fibromyalgia may be useful in the management and treatment of fibromyalgia patients. Clinicians, physicians, physiotherapists, and health care professionals obtain more information and knowledge. A review of the literature found no study comparing pain, functional capacity, balance, and BA in individuals with and without FM. Based on all this, the aim of this study was to evaluate and compare the parameters of pain, functional capacity, balance mobility, and BA in women with and without FM.
Materials and Methods
ParticipantsThe sample of the study consisted of 66 women without (n = 33) and with (n = 33) FM. The protocol of the Declaration of Helsinki was followed. The study was conducted between November 2022 and March 2023 at the Kirsehir Ahi Evran University School of Physical Therapy and Rehabilitation. Patients were admitted to the Kirsehir Ahi Evran University Physical Medicine and Rehabilitation Outpatient Clinic. The inclusion criteria were women (1) who were over 18 and under 65 years, (2) who were newly diagnosed with FM according to the 1990 American College of Rheumatology criteria, (3) who were cooperative, and (4) who accepted to participate in the study. Subjects with systemic diseases, neurological disorders, and medication history were excluded. The participants were invited to be informed about the aim of the study. To participate, patients were asked to sign a written form of consent.
Body Awareness: Body Awareness Questionnaire (BAQ) was used to evaluate the BA of the participants. BAQ includes 18 variables that were grouped into four distinct. These are (1) prediction of body responses, (2) estimation of illness onset, (3) sleep-wake cycle, and (4) awareness of body process. BAQ is a self-report scale where the participants had to score each statement between 1 and 7 values (1 = not all of them are true of me, 7 = completely true of me). The high total score on the survey indicates a good BA status 5.
PainAn algometer was used to assess the sensitivity of mechanical pain at the 18 tender points. The pressure was applied to these points until the patient reported pain. The applied force was recorded from the display. Values are measured in kg/cm2. This measurement was repeated three times. The average of the scores was recorded 6.
Functional Capacity and MobilityFunctional capacity was measured using the 6-Minute Walk Test (6MWT). The 6MWT was found by the American Thoracic and is reliable in patients with FM. Participants were instructed to walk on a 30-meter corridor for 6 minutes. A stopwatch was used to measure the time. The distance that the patient walked was recorded in meters 7. In the Timed Up and Go Test, the participant must stand up from a chair, walk three meters, turn around at a marked point, and sit back down. To measure the time a chronometer was used 8.
Balance: The Biodex Balance System SD (BBS) (Biodex Medical System Inc., Shirley, USA) was used to assess participants’ ability to maintain balance. Three parameters of dynamic and static balance were applied with eyes open; (1) medial-lateral stability index (MLSI), (2) overall stability index (OSI), and (3) anterior-posterior stability index (APSI). These evaluations for each index were repeated three times. The average of these three scores was calculated by the BBS. A higher score represented low balance capacity 9.
Impact of FibromyalgiaThe Turkish reliability and validity of the Fibromyalgia Impact Questionnaire (FIQ) were established by Sarmer et al. This questionnaire consists of 10 items. The questionnaire is assessed by the subject. The FIQ includes 10 different characteristics; these are as follows: pain, stiffness, work status, fatigue, physical function, depression, anxiety, well- being, morning tiredness, and difficulty at work. The total score of this questionnaire ranges from 0-100 points. Higher scores indicate a low level of functionality 10.
Statistical AnalysisIn this study, for statistical analysis, the SPSS 22.0 package program (IBM Corp., Armonk, NY, USA) was used. The percentage values obtained by counting between the control group and FM group were compared using the Chi-square test. For the correlation between variables, the Pearson correlation analysis was used. The data were normally distributed. The significance of the variables was accepted as a p-value of <0,05.
Ethical ApprovalThe Ethical Committee of Clinical Researches of Kirsehir Ahi Evran University, Faculty of Medicine approved the research protocol (Date: 2022-11-10, No: 2022-18/164).
Results
The socio-demographic and descriptive statistics of women in both groups, FM group and control group, are presented in Table 1. The results in Table 1 indicate that there was no significant difference between the two groups was not significantly different regarding the descriptive characteristics of the participants (P = 0.861, P = 1.000), except for BMI. As the values of the two groups were compared in Table 2, a significant difference was found between 6MWT (P= 0.018), FIQ score (P < 0.001), TUG score (P < 0.001), and in pain threshold variables of the 16 tender points.
Discussion
According to the current study’s result, a significant difference was found between functional capacity (6MWT), FIQ score, TUG score, and pain level in 16 tender points on both sides except the tender points in trapezius r (p < 0.05). These trigger points are as follows: trochanter, knee, occiput, second costa, gluteal, lateral epicondyle, supraspinatus, and cervical. The results of this study indicated that FM had a negative impact on functional capacity and mobility and on pain level.
In the literature, some studies assess the effect of body awareness therapy in FM cases, but no study that determines the level of body awareness. In individuals with FM, the assessment and improvement of BA is useful. It was found that neurological and orthopedic disorders, injuries, and hereditary diseases have an effect on sensory and motor development. As a result, BA is also negatively affected 11. In the current study, no significant difference was found in the BAQ score in those with and without fibromyalgia. In this study, patients with orthopedic injuries or neurological diseases were not included. The patients were directly referred and were seen for the first time. It is suggested that low pain levels in the acute phase may not affect physical and mental function. Behavioral changes reflected in the body language may not be seen during this period.
Recent studies showed that 6MWT scores were reduced as compared with healthy subjects. In the literature, it was found that the walking speed of FM patients is low, and stride length and cycle frequency were decreased, which may be related to bradykinesia 12,13. Costa et al. found decreased distance walking in 6MWT with reduced gait duration and step length in FM patients in comparison to subjects without pain 14. In accordance with the literature, in this study, FM patients presented low functional capacity scores compared to healthy subjects. These results showed that widespread pain in FM patients may restrict walking. It may also reduce stride length, step length, and cycle frequency. Additionally, this result may be explained by the fear of movement and exercise, which may increase pain levels in FM patients. Moreover, low functional capacity may represent inconvenient gait performance, and low blood pressure may lead to altered functional performance.
In a study by Jones et al., balance disorder was found to be associated with FM 15. The enormous decrease in density and volume of the central nervous system (CNS) gray matter in patients may lead to a balance disorder. Balance disturbance may be associated with an increase in pain threshold 17. In addition, a higher frequency of falls was found in FM patients with reduced balance than in healthy subjects 18. Additionally, chronic pain may trigger a process of central sensitization, which is seen in FM. These processes may affect the processing of postural information, leading to balance disorder 19. Contrary to recent studies in the literature, a significant difference between the groups was not found. In this study, the FM patients were referred directly when diagnosed with FM without taking medication. In this acute phase, the CNS may not be affected, and the central sensitization process may be at the beginning stage. Therefore, balance disorder may not be affected in FM patients. When assessing and comparing data, it is suggested to note the stage of FM patients.
The literature is fully in accord with clinical knowledge and observation that pain levels in trigger points in FM patients could be notably lower as compared with healthy subjects 20,21. In accordance with the literature, in this study, the FM group had a low pain threshold similar to the previous studies in the literature. Also, the rate of affected tender points was more similar to previous studies. A significant difference was not found in the left and right trapezius. This may be due to the functional use and tension of muscles. The trapezius muscle is constantly used in posture and daily activities. It can also be tense in individuals without fibromyalgia due to reasons such as stress, poor posture, or long periods of desk work. This may cause the pain threshold to be similar between the two groups. Additionally, the trapezius muscle is one of the muscles directly related to stress. Factors such as anxiety, depression, and stress can cause muscle tension in both fibromyalgia patients and healthy individuals, which can make the pain threshold similar. The result of the study showed that FM negatively affected the functional capacity of patients. Generally, records of parameters such as pain threshold level, balance, BA, and functional capacity were found extremely low in FM patients. Based on existing knowledge of the impact of FM, these parameters could be included when assessing and planning physiotherapeutic rehabilitation programs. Cooperation between investigators, physicians, and physiotherapists is also important to improve patients’ functional capacity and balance. These data will assist decision-making efforts in the diagnosis and analysis of FM. Careful evaluation of the FM symptoms would help to select appropriate devices and to decrease the number of FM symptoms. FM is not yet fully understood, and many questions regarding prevention of FM symptoms remain to be answered. For the prevention of FM, future researches are needed to find the factors influencing FM and additionally, the effective ways to improve the health of the world’s population. Moreover, these results of the study should be taken into account when evaluating people clinically who suffer from FM. The beneficial outcomes should be analyzed to plan a program for rehabilitation and to use the appropriate measurements.
Limitations
A possible limitation of this study is the inclusion of only women patients aged 18 to 65 years, due to the statistically high rate of FM in women. The sex of patients may have an impact on the results. Thus, this topic can be investigated in certain age ranges and different populations, including men. Secondly, we used only field tests for clinical assessment. In future studies, laboratory data from patients with FM could be used to obtain more objective data.
Conclusion
The current study examined the relationship between BA and pain, functional capacity, and balance in women with FM. An important finding is that balance and pain threshold at existing trigger points are interrelated. Moreover, a relationship between balance and functional capacity in FM patients was found. A remarkable finding of the study is the negative impact of FM on the functional capacity of the patients. These parameters should be taken into account when assessing and planning rehabilitation and assessment programs.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Kirsehir Ahi Evran University, Faculty of Medicine (Date: 2022-11-10, No: 2022-18/164)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
References
-
Clauw DJ. Fibromyalgia: A clinical review. JAMA. 2014;311(15):1547-55.
-
Çetin N, Yalbuzdag ŞA, Cabioşlu MT, Turhan N. Fibromiyalji sendromunda yaşam kalitesi üzerine etkili faktörler. Turk J Rheumatol. 2009;24(2):13-29.
-
Akkaya N, Akkaya S, Atalay NS, Balci CS, Sahin F. Relationship between the body image and level of pain, functional status, severity of depression, and quality of life in patients with fibromyalgia syndrome. Clin Rheumatol. 2012;31(6):983-8.
-
Shields SA, Mallory ME, Simon A. The body awareness questionnaire: reliability and validity. J Pers Assess. 1989;53(4):802-15.
-
Karaca S, Bayar B. Turkish version of body awareness questionnaire: validity and reliability study. Turk J Physiother Rehabil. 2021;32(1):44-50.
-
Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum. 1990;33(2):160-72.
-
Pankoff BA, Overend TJ, Lucy SD, White KP. Reliability of the six‐minute walk test in people with fibromyalgia. Arthritis Care Res. 2000;13(5):291-5.
-
Khasnis A, Gokula RM. Romberg’s test. J Postgrad Med. 2003;49(2):169-72.
-
Arnold BL, Schmitz RJ. Examination of balance measures produced by the biodex stability system. J Athl Train. 1998;33(4):323.
-
Sarmer S, Ergin S, Yavuzer G. The validity and reliability of the Turkish version of the Fibromyalgia Impact Questionnaire. Rheumatol Int. 2000;20:9-12.
-
Bravo C, Skjaerven LH, Espart A, Guitard Sein-Echaluce L, Catalan-Matamoros D. Basic Body Awareness Therapy in patients suffering from fibromyalgia: A randomized clinical trial. Physiother Theory Pract. 2019;35(10):919-29.
-
Ulus Y, Akyol Y, Tander B, Bilgici A, Kuru Ö. Knee proprioception and balance in Turkish women with and without fibromyalgia syndrome. Turk J Phys Med Rehabil. 2013;59(2):12-18.
-
Tavares LF, Germano Maciel D, Pereira Barros da Silva TY, Brito Vieira WH. Comparison of functional and isokinetic performance between healthy women and women with fibromyalgia. J Bodyw Mov Ther. 2020;24(1):248-52.
-
Costa IdS, Gamundí A, Miranda JGV, França LGS, De Santana CN, Montoya P. Altered functional performance in patients with fibromyalgia. Frontiers in human neuroscience. 2017;11:14.
-
Jones KD, Horak FB, Winters-Stone K, Irvine JM, Bennett RM. Fibromyalgia is associated with impaired balance and falls. J Clin Rheumatol. 2009;15(1):16-21.
-
Peinado-Rubia A, Osuna-Perez MC, Rodriguez-Almagro D, Zagalaz-Anula N, Lopez-Ruiz MC, Lomas-Vega R. Impaired balance in patients with fibromyalgia syndrome: predictors of the impact of this disorder and balance confidence. Int J Environ Res Public Health. 2020;17(9):3160.
-
D’Onghia M, Ciaffi J, Lisi L, et al. Fibromyalgia and obesity: A comprehensive systematic review and meta-analysis. Semin Arthritis Rheum. 2021;51(2):409- 24.
-
Sarihan K, Uzkeser H. Fibromiyalji Tanılı Hastalarda B 12 Vitamini, D Vitamini, Magnezyum Düzeyleri ile Düşme Riski İlişkisi [The Relationship Between Vitamin B12, Vitamin D, and Magnesium Levels and the Risk of Falling in Patients Diagnosed with Fibromyalgia]. J PMR Sci 2024;27(1):1-10.
-
Núñez-Fuentes D, Obrero-Gaitán E, Zagalaz-Anula N, et al. Alteration of postural balance in patients with fibromyalgia syndrome—a systematic review and meta-analysis. Diagnostics (Basel). 2021;11(1):258-72.
-
Yunus M, Masi AT, Calabro JJ, Miller KA, Feigenbaum SL. Primary fibromyalgia (fibrositis): Clinical study of 50 patients with matched normal controls. Semin Arthritis Rheum. 1981;11(1):151-71.
-
Sola AE. Treatment of myofascial pain syndromes. Adv Pain Res Ther. 1984;(7):467-85.
Tables
Table 1. Descriptive statistics of the participants
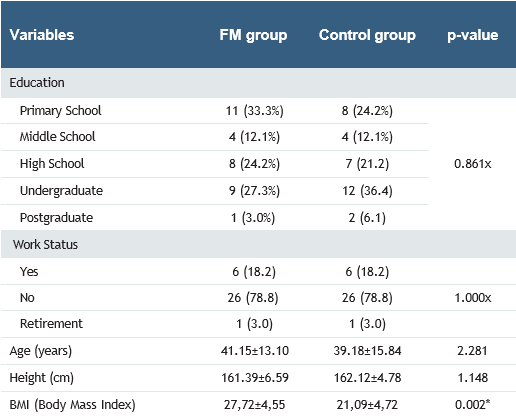
x: Chi-square test, () %: percentage, n: number of participants, *in statistical analysis, the significance value was accepted as p < 0.05.
Table 2. Comparison of the mean values

%: percentage, n: number of participants, R: right, L: left, 6 MWT: 6 Minute Walk Test, A-P: Anterior-Posterior, M-L: Medial-Lateral, BAQ: Body Awareness Questionnaire; sec: second, m: meter, kg: kilogram, cm2: square centimeter, *in statistical analysis, the significance value was accepted as p < 0.05. Pearson Correlation analysis was used.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mensure Aslan, Anıl Özüdoğru, Figen Tuncay. Comparison of pain, functional capacity, balance, and body awareness in individuals with and without fibromyalgia. Ann Clin Anal Med 2025; DOI: 10.4328/ACAM.22535
- Received:
- December 25, 2024
- Accepted:
- April 7, 2025
- Published Online:
- April 25, 2025
- Printed:
- November 1, 2025