
Histopathological examination of A1 pulley tissue resected in trigger fingersurgery and correlation with clinical results
Histopathology of A1 pulley tissue
Authors
Abstract
AimThe aim was to analyze the histopathological features of the A1 pulley tenosynovial tissue surgically removed with the diagnosis of the trigger finger and to reveal its correlation with the clinic.
MethodsPathological tissue samples of 120 patients who underwent A1 pulley surgical resection with the diagnosis of trigger finger between January 2020 and December 2023 were retrospectively examined. The samples were evaluated with H&E, Alcian blue staining, and CD44 immunohistochemistry. The detected inflammation level, increased vascularization, degree of fibrosis, collagen structure, tenocyte proliferation, and hyalinization were scored semiquantitatively. The relationship between histopathological findings and the clinic was evaluated statistically.
ResultsIn 81.7% of the examined cases, inflammation at different levels (mild 37.5%, moderate 30.0%, severe 14.2%) and increased vascularization were detected in 68.3%. In terms of fibrosis, varying degrees of involvement (mild 31.7%, moderate 40.0%, severe 18.3%) were observed in 90% of the cases. Collagen alignment was found to be disrupted in 71.7% of the cases. Tenocyte proliferation was positive in 76.7% and hyalinization was positive in 63.3%. A significant positive correlation was found between the degree of inflammation and VAS score (r = 0.684, p<0.001) and between the degree of fibrosis and symptom duration (r = 0.712, p<0.001).
ConclusionIn the pathogenesis of the trigger finger, the presence of chondrocyte-like cells in the tenosynovial tissue, hypocellular collagen matrix containing hyaluronic acid, and inflammatory changes stand out as characteristic findings. A significant correlation was determined between the severity of these histopathological changes and clinical findings.
Keywords
Introduction
Trigger finger (stenosing tenosynovitis) is a pathology that occurs with thickening and histomorphological changes in the fibrous structure of the flexor tendon sheath and A1 pulley. Accordingly, the movement functions of the flexor tendons are impaired, and clinical symptoms develop.1 Histopathological studies have revealed complex tissue changes such as inflammatory changes, increased vascularization, and fibrosis in the A1 pulley tissue.2,3
When the A1 pulley is examined microscopically, its natural structure consists of regular collagen fibrils, minimal vascularity, and sparse fibroblasts. However, in the case of the trigger finger, disruption in the arrangement of collagen fibers, an increase in type III collagen, and significant proliferation in vascular structures are observed.4,5 Immunohistochemical studies have revealed infiltration of macrophages and increased expression of transforming growth factor-β (TGF-β).6,7
In histopathological evaluations, acute inflammatory cell infiltration and vascular proliferation are evident in the early phase of the disease, while fibrosis and hyalinization are more prominent in the chronic phase. In particular, increased tenocytes and extracellular matrix changes play a key role in the worsening of the disease.8,9,10 In analyses performed with semi-quantitative histopathological scoring systems, it was observed that these changes correlated with the clinical severity of the disease.11,12
Materials and Methods
Patient Selection and Clinical EvaluationIn our study, 120 patients who underwent A1 pulley surgery due to a trigger finger in our clinic between January 2020 and December 2023 were retrospectively examined. Patients were staged preoperatively using Green’s classification.11 Patients who had previously received corticosteroid injections due to trigger finger had inflammatory rheumatic diseases, and had undergone revision surgery on the same finger were excluded from our study.13
Surgical Sample Collection and Tissue Follow-upA1 pulley tissue samples we obtained through the surgical procedure were placed in 10% buffered formalin for pathological analysis. They were fixed for 24 hours. We performed tissue tracking as follows:8,14
•Dehydration with alcohol series •Clearing with xylol
•Paraffin application and blocking
•Taking 4 μm thick sections with a microtome
•H&E staining and Masson trichrome staining in selected preparations
Histopathological ExaminationWe evaluated the prepared sections according to the following criteria based on the clinical information of the patients:15,16
•Inflammation Assessment: oNone: Inflammatory cell infiltration oMild: Focal minimal infiltration oModerate: Widespread moderate infiltration oSevere: Dense diffuse infiltration
•Other Parameters: oAssessment of increase in vascular structures oFibrosis degree (absent/mild/moderate/severe) oCollagen fiber pattern analysis oTenocyte proliferation oPresence of hyaline changes In case of discrepancy, we made a mutual decision by evaluating with kappa analysis together with another pathologist at the microscope.17
Patient SelectionOur study was conducted retrospectively and 120 patients who underwent A1 pulley surgery due to trigger finger in our clinic between January 2020 and December 2023 were included in the study.11 Inclusion Criteria:
•Being over 18 years of age •Being diagnosed with trigger finger
•Accepting surgical treatmen
•Committing to regular postoperative follow-ups Exclusion Criteria:
•Having previously undergone trigger finger surgery on the same finger
•Having received local corticosteroid injection within the last 6 months
•Presence of rheumatoid arthritis or other inflammatory rheumatic diseases
•History of trauma/surgery on the wrist or finger •Presence of carpal tunnel syndrome
•Presence of Dupuytren’s contracture
•Pregnancy •Insufficient tissue sample for pathological examination.14,15
Ethical ApprovalThis study was approved by the Ethics Committee of Adana City Hospital (Date: 02.01.2025, Decision No: 314).
Statistical AnalysisThe data obtained in this study were analyzed using SPSS Statistics 25.0 software. Descriptive statistics for continuous variables are presented as mean ± standard deviation, and for categorical variables as percentage (%). To analyze the relationship between histopathological findings and clinical data:
•Spearman Correlation Analysis: To evaluate the nonlinear relationship between continuous variables (e.g., the relationship between the degree of inflammation and VAS score).
•Chi-Square Test: To analyze the relationship between categorical variables (e.g., the relationship between increased vascularization and the development of complications).
•Independent Sample T-Test: To compare the means of continuous variables between two groups (e.g., QuickDASH scores for groups with and without increased vascularization).
•Mann-Whitney U Test: To compare continuous variables that do not show normal distribution (e.g., the relationship between the degree of fibrosis and the duration of symptoms).
•Kappa Analysis: Used to measure the agreement between the evaluations between two pathologists. The Kolmogorov-Smirnov Test was used to test normality distribution. Nonparametric tests were preferred for data that did not show normal distribution. The significance level in the analyses was accepted as p<0.05.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
Demographic and Clinical FeaturesWhen the demographic data of 120 patients included in this study were examined, the mean age was found to be 54.3 ± 11.2 years. More than two-thirds of the patients were women (68.3%, n = 82), while the proportion of men was 31.7% (n = 38).
The mean time from the onset of symptoms to surgical intervention was calculated as 8.4 ± 4.2 months, indicating a significant delay in surgical intervention. Dominant hand involvement was observed in 65% of the patients (n = 78), while non-dominant hand involvement was detected in 35% (n = 42). The mean body mass index (BMI) of the patients was 27.8 ± 4.6 kg/m², indicating that the patients were in the slightly obese class. The most common comorbid disease was Diabetes Mellitus, which was detected in 26.7% (n = 32) of the patients. This was followed by Hypertension (23.3%, n = 28) and Hypothyroidism (12.5%, n = 15). In the evaluation made according to occupational groups, it was determined that the majority of the patients were housewives (37.5%, n = 45), followed by office workers (26.7%, n = 32), workers (20.8%, n = 25) and retirees (15.0%, n = 18) (Table 1). The most commonly affected finger was the thumb (38.3%, n = 46), followed by the middle finger (26.7%, n = 32), index finger (23.3%, n = 28), ring finger (8.3%, n = 10) and little finger (3.3%, n = 4).
The largest group consisted of Grade III patients (%43.3, n = 52). This was followed by Grade II (%31.7, n = 38), Grade IV (%15.0, n = 18) and Grade I (%10.0, n = 12) patients, respectively. In the preoperative functional evaluation, the mean QuickDASH score indicating the limitation in the patient’s daily living activities was determined as 48.6 ± 12.4. In the pain evaluation, the mean VAS (Visual Analog Scale) score was 7.2 ± 1.8, indicating severe pain level. The mean hand grip strength was calculated as 18.4 ± 6.2 kg and the range of motion of the affected finger was severely limited with an average of 35.2 ± 12.6 degrees.
Histopathological Examination ResultsIn the microscopic evaluation of the resected A1 pulley tissue; In terms of inflammatory changes, varying degrees of inflammation were seen in the majority of cases (%81.7, n = 98). While the degree of inflammation was distributed as mild (%37.5, n = 45), moderate (%30.0, n = 36) and severe (%14.2, n = 17), inflammation was seen in only 18.3% (n = 22) of the cases. Proliferation in vascular structures was seen as positive in a significant majority of the patients (%68.3, n = 82). When the fibrotic structure was examined, varying degrees of fibrosis were detected in the majority of the cases (%90.0, n = 108). The distribution of fibrosis was as follows: moderate (%40.0, n=48), mild (%31.7, n = 38), and severe (%18.3, n = 22). Normal collagen formation was preserved in only 28.3% (n = 34) of the patients and was markedly irregular in the majority (71.7%, n = 86). Tenocyte proliferation was positive in more than threequarters of the cases (76.7%, n = 92), and hyaline changes were positive in approximately two-thirds of the cases (63.3%, n = 76) (Figure 1).
In histopathological examination, a single-layer synovial cell layer was observed in the normal A1 pulley tissue (Figure 2A), while in trigger finger cases, significant inflammation and increased vascularization were observed (Figure 2B). Chondrocyte-like cells were also observed under the microscope (Figure 2C). Hyaluronic acid accumulation, which showed positive staining with Alcian blue, was observed around these cells (Figure 2D) and the staining disappeared after hyaluronidase application (Figure 2E). Chondrocyte-like cells showed positive expression with CD44 immunohistochemistry (Figure 2F).
Clinicopathological Correlation AnalysisIn our correlation analyses, a strong positive relationship was found between the degree of tissue inflammation and both pain scores (r = 0.684, p<0.001) and functional disability level (QuickDASH score) (r = 0.625, p<0.001). Fibrosis level showed a significant positive correlation with symptom duration (r = 0.712, p<0.001), which revealed that fibrotic changes increased with the prolongation of disease duration. Pain scores were found to be significantly higher in patients with increased vascularization (r = 0.548, p<0.001) (Figure 3).
Discussion
Histopathological analysis of A1 pulley tenosynovial tissue is critical in understanding the pathogenesis of the trigger finger.1 The microscopic findings and their clinical implications in our study provide very important data in terms of understanding the basis of the disease.17 Recent literature studies also highlight the dynamic role of tenosynovial tissue.2
Immunohistochemical Findings And Cellular ChangesCD44-positive chondrocyte-like cells observed in tenosynovial tissue explain the cellular basis of pathogenesis.16 S-100 protein negativity and CD44 positivity in these cells support the fibroblastic differentiation hypothesis in the literature.3 These findings, which are parallel to the cell population defined by Yang et al.6 exhibit explanatory features for the pathogenetic mechanism when considered together with the matrix organization study by Fritz et al.7 The tenosynovial tissue ultrastructure analysis by Ettema et al.18 provides biomechanical support for this mechanism.
Matrix Changes And Ultrastructural AnalysisThe hypocellular collagen matrix and hyaluronic acid accumulation we observed are quite similar to the study of Coronel et al.10 The standardized scoring of these changes was based on the criteria of Angrisani et al.8 and it was found that there was a correlation with the ultrasonographic findings of Bianchi et al.19
Inflammatory Process And VascularizationInflammatory patterns and vascular proliferation added new parameters to the scoring defined by Muthu et al.17 The chronic inflammation findings presented by Johnson et al. 20 are also parallel to the clinical progression analysis of Huang et al.21 These findings show significant differences from the normal tenosynovial structure described by Cohen et al.4 Our analysis of the relationship between time from symptom onset to surgery (mean 8.4 ± 4.2 months) and inflammatory changes revealed that patients with longer waiting times tended to show more severe inflammatory patterns. Among patients with inflammation (81.7%), we observed a progression from mild (37.5%) to moderate (30.0%) and severe (14.2%) inflammation that corresponded with increasing duration of symptoms. This observation has important clinical implications, suggesting that prolonged waiting time for surgery may contribute to increased inflammatory severity. This finding aligns with Straszewski et al.’s 14 conclusions about the importance of surgical timing in managing inflammatory progression.
Clinical And Radiological CorrelationsThe prognostic factors specified in the study of Belloti et al.22 showed a strong correlation with our histopathological analysis results. These correlations confirm the hypotheses put forward in the early studies of Sbernardori et al.5
Treatment ImplicationsThe factors affecting treatment success highlighted in the meta-analysis of Lo et al.23 can be explained by our findings obtained with histopathological analysis. The literature review of Markowitz et al.24 emphasizes the role of histopathological changes in predicting treatment response. This approach is also in line with the evidence-based treatment recommendations of Amirfeyz et al.11
Methodological Approach And StandardizationThe standardized methodology we used adds strength to our study.8 Our approach for analyzing advanced-stage cases aligns with recommended standards25 and is consistent with the clinical evaluation criteria of Bridges et al.12
Future PerspectivesThe results obtained in our study support the conclusion that the clinical reflections of histopathological findings are decisive in the treatment of trigger fingers, emphasized in a recent review by Donati et al.9 The conservative treatment evaluation of Lunsford et al.13 and the temporal relationship analysis between corticosteroid injection and surgical outcomes by Straszewski et al.14 are guiding future research. It seems that the evaluation of postoperative complication rates in diabetic patients by Federer et al. 15 will contribute to the development of objective evaluation criteria. The histopathological patterns defined by Uchihashi et al.2 may also shed light on new treatment goals.
Limitations
This study has the following limitations:
1.Methodological Limitations:
•Retrospective study design
•A limited number of control tissue samples
•Inability to perform electron microscopic evaluation
•Collection of samples from a single center
2.Technical Limitations:
•Analysis restricted to surgical specimens only
•Inability to study advanced molecular markers
•Limited immunohistochemical panel (only H&E, Alcian blue, and CD44)
•Absence of high-throughput molecular analyses
•Lack of fresh frozen tissue samples for specialized studies 3.Clinical Limitations: •Inability to evaluate preoperative radiological findings
•Absence of long-term follow-up data
•Unable to assess the effect of treatment response on histopathological changes
•Variation in the time interval between symptom onset and surgery
4.Statistical Limitations:
•Small sample size in subgroup analyses
•Non-homogeneous distribution between diabetic and nondiabetic patient groups
•Limited power for correlation analyses in certain histopathological parameters These limitations should be considered when interpreting the results, and future studies should address these constraints through more comprehensive and prospective evaluations with larger sample sizes and advanced molecular techniques.
Conclusion
Conclusion Our study provides important data in terms of a detailed description of histopathological changes in A1 pulley tissue in the pathogenesis of the trigger finger. Histopathological findings such as inflammation, fibrosis, increased vascularization and hyalinization in particular show a significant correlation with clinical symptoms. These results may contribute to the establishment of objective criteria in the staging of trigger finger disease.
In terms of clinical application, the findings obtained in our study can be evaluated as follows:
•The degree of inflammation and fibrosis may be enlightening in predicting the severity of a patient’s clinical symptoms and their potential for recovery after surgery.
•Chondrocyte-like cells, especially detected by CD44 immunohistochemical staining, may provide opportunities for new treatment strategies targeting cellular targets.
•The effect of vascular proliferation on treatment results may suggest the need for revision of surgical techniques or additional complementary treatments. Our recommendations for future research are as follows:
1.Investigation of Molecular Mechanisms: Studies investigating the genetic and biochemical basis of CD44-positive cells and extracellular matrix changes in understanding the pathogenesis of trigger finger disease may yield very good results.
2.Development of Treatment Approaches: The effect of these histopathological findings on the response to treatment can be analyzed and patient-specific treatment approaches can be investigated.
3.Early Diagnostic Criteria: There is a strong relationship between clinical symptoms and histopathological findings. Early diagnostic criteria can be developed with advanced imaging and biomarker analyses.
In conclusion; this study draws attention to the importance of histopathological changes in trigger finger pathogenesis and makes valuable contributions to the clinical management process. New treatment strategies to be developed based on these findings in the future may improve the quality of life of patients and stop the progression of the disease.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was waived due to the retrospective nature of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
A1: Annular pulley 1
BMI: Body mass index
CD44: Cluster of differentiation 44
H&E: Hematoxylin and eosin
VAS: Visual Analog Scale
References
-
Shohda E, Sheta RA. Misconceptions about trigger finger: a scoping review. Adv Rheumatol. 2024;64(1):53-58. doi:10.1186/s42358-024-00379-7
-
Uchihashi K, Tsuruta T, Mine H, et al. Histopathology of tenosynovium in trigger fingers. Pathol Int. 2014;64(6):276-282. doi:10.1111/pin.12168
-
Stirling PHC, Jenkins PJ, Duckworth AD, Clement ND, McEachan JE. Functional outcomes of trigger finger release in nondiabetic and diabetic patients. J Hand Surg Eur Vol. 2020;45(10):1078-1082. doi:10.1177/1753193420925027
-
Ng WKY, Olmscheid N, Worhacz K, Sietsema D, Edwards S. Steroid injection and open trigger finger release outcomes: a retrospective review of 999 digits. Hand (N Y). 2020;15(3):399-406. doi:10.1177/1558944718796559
-
Matzon JL, Lebowitz C, Graham JG, Lutsky KF, Beredjiklian PK. Risk of infection in trigger finger release surgery following corticosteroid injection. J Hand Surg Am. 2020;45(4):310-316. doi:10.1016/j.jhsa.2020.01.007
-
Yang TH, Chen HC, Liu YC, et al. Clinical and pathological correlates of severity classifications in trigger fingers based on computer-aided image analysis. Biomed Eng Online. 2014;13:100. doi:10.1186/1475-925x-13-100
-
Fritz T, Ducommun P, Pohlemann T, et al. Flexor tendon grafts for pulley reconstruction: morphological aspects. Ann Anat. 2020;231:1-7. doi:10.1016/j.aanat.2020.151550
-
Angrisani N, Willbold E, Kampmann A, Derksen A, Reifenrath J. Histology of tendon and enthesis. Eur Cell Mater. 2022;43:228-251.
-
Donati D, Ricci V, Boccolari P, et al. From diagnosis to rehabilitation of trigger finger. BMC Musculoskelet Disord. 2024;25(1):1-14.
-
Coronel L, Mandl P, Miguel-Pérez M, et al. Characterization of digital annular pulleys and their entheses: an ultrasonographic study with anatomical and histological correlations. Rheumatology (Oxford). 2024;63(11):3050-3055. doi:10.1093/rheumatology/kead614
-
Amirfeyz R, Clark D, Jones J, Singh R, Watkins T. Evidence-based management of adult trigger digits. J Hand Surg Eur Vol. 2017;42(5):473-480. doi:10.1177/1753193416682917
-
Bridges TN, Ohliger E, Kistler JM. Trigger finger: evaluation, management. SurgiColl. 2023;1(1):1-6. doi:10.58616/surgicoll.00003
-
Lunsford D, Peterson L, Roy S, Chambers M, Blake F. Conservative management of trigger finger. J Hand Ther. 2019;32(4):417-429.
-
Straszewski AJ, Lee CS, Dickherber JL, Wolf JM. Temporal relationship of corticosteroid injection and open release for trigger finger and correlation with postoperative deep infections. J Hand Surg Am. 2022;47(11):1116-1126. doi:10.1016/j.jhsa.2021.08.017
-
Federer AE, Baumgartner RE, Cunningham DJ, Mithani SK. Increased rate of complications following trigger finger release in diabetic patients. Plast Reconstr Surg. 2020;146(4):420-427. doi:10.1097/prs.0000000000007156
-
Lundin AC, Bergstrom J, Olsson H, Andersson P. Trigger finger and tendinosis. Scand J Med Sci Sports. 2014;24(2):363-368. doi:10.1111/j.1600-0838.2012.01514.x
-
Muthu S, Patel R, Shah R, Kumar V, Gupta K. Tenosynovitis of hand: causes and complications. World J Clin Cases. 2024;12(4):671-676. doi:10.12998/wjcc.v12.i4.671
-
Hansen RL, Søndergaard M, Lange J. Open surgery versus ultrasound-guided corticosteroid injection for trigger finger: a randomized controlled trial with 1-year follow-up. J Hand Surg Am. 2017;42(5):359-366. doi:10.1016/j.jhsa.2017.02.011
-
Bianchi S, Rossi P, Leone A, Neri E. Ultrasound features of trigger finger. J Ultrasound Med. 2019;38(12):3141-3154. doi:10.1002/jum.15025
-
Johnson E, Keller T, Simmons P, Wallace N. Recognizing and treating trigger finger. J Fam Pract. 2021;70(7):334-340. doi:10.12788/jfp.0239
-
Huang HK, Chen YC, Wu PH, Tsai CH. Outcomes and complications after percutaneous release for trigger digits. J Hand Surg Eur Vol. 2015;40(7):735-759. doi:10.1177/1753193415590389
-
Belloti JC, Rodrigues A, Silva J, Pereira E, Costa R. Trigger finger treatment. Rev Bras Ortop. 2022;57(6):911-916.
-
Lo YC, Tan Y, Hu J, Chou Y. High incidence of trigger finger. Int J Surg. 2023;109(8):2427-2434.
-
Markowitz MI, Lewis S, Green R, Singh A, Patel M. Most cited publications. J Hand Surg. 2023;48(2):188-195.
-
Dardas AZ, Vandenberg J, Olson J, Gelberman RH, Calfee RP. Long-term effectiveness of repeat corticosteroid injections for trigger finger. J Hand Surg Am. 2017;42(4):227-235. doi:10.1016/j.jhsa.2017.02.001
Figures
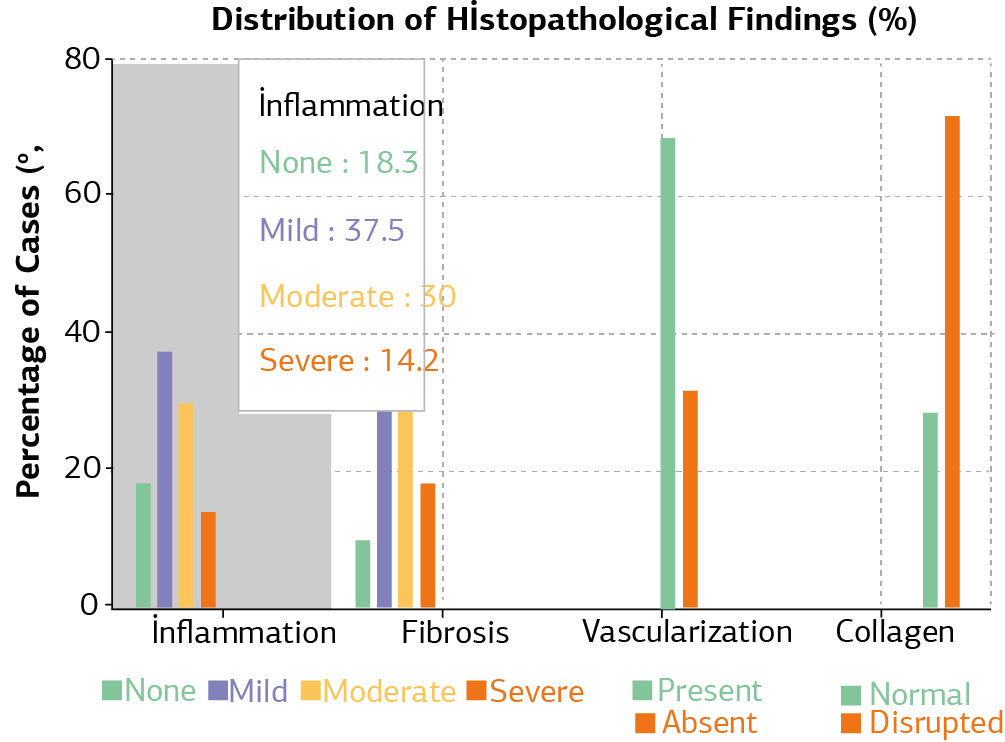
Figure 1. Distribution of histopathological findings (%)

Figure 2. Histopathological and immunohistochemical analysis of A1 pulley tissue

Figure 3. Correlation between inflammation severity and fibrosis grades in trigger finger
Tables
Table 1. Demographic and clinical characteristics (n = 120)

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Berna Eriten, Serdar Menekşe. Histopathological examination of A1 pulley tissue resected in trigger fingersurgery and correlation with clinical results. Ann Clin Anal Med 2025;16(3):187-192. doi:10.4328/ACAM.22547
- Received:
- January 5, 2025
- Accepted:
- February 11, 2025
- Published Online:
- February 21, 2025
- Printed:
- March 1, 2025