
Ai-powered screening for psoriatic arthritis: a comparative study withexisting tools
Ai-powered screening for psoriatic arthritis
Authors
Abstract
AimPsoriatic arthritis (PsA) is common in psoriasis patients but is sometimes overlooked. Delayed diagnosis of PsA can lead to joint erosion, axial damage, and impaired physical function. Screening tools are essential for early diagnosis and selecting the right patients for rheumatological evaluation. We aimed to develop a practical and comprehensive screening tool using the ChatGPT and compare its performance with that of validated questionnaires.
MethodsA prospective study was conducted on adult psoriasis patients who had musculoskeletal complaints but were not diagnosed with PsA. Artificial intelligence (AI)-powered PsA screening (AIPS) was developed by selecting questions on peripheral arthritis, axial inflammation, and enthesitis from multivariate analyses conducted via Chat GPT 4.0. The Psoriasis Epidemiology Screening Tool (PEST), the Early Arthritis for Psoriatic Patients Questionnaire (EARP), and the AIPS questionnaires were completed concurrently by all psoriasis patients. All patients were evaluated for PSA diagnosis by three rheumatologists who were blinded to the questionnaire responses.
ResultsThe study included 199 patients, 115 (57.8%) of whom were female. The mean age was 44.4 ± 13.3 years. PSA was detected in 84 psoriasis patients (42.2%). The sensitivity of the EARP questionnaire, 98%, was greater than those of the AIPS and PEST questionnaires, which had 92% and 83% sensitivity values, respectively. However, the AIPS had a higher specificity at 96% than did the PEST and EARP, with specificities of 91% and 80%, respectively.
ConclusionThe AIPS questionnaire is an effective tool for screening for PsA, exhibiting high sensitivity and specificity. Artificial intelligence can help screen patients, saving time and money.
Keywords
Introduction
Psoriasis is a common chronic inflammatory papulosquamous skin disease with various clinical presentations. Psoriatic arthritis (PsA) has a higher frequency, reaching 30% in psoriasis patients, and causes dysfunction by turning into severe arthritis.1 It is estimated that approximately 80% of patients with PsA present to dermatology clinics with cutaneous psoriasis up to 10 years before the onset of arthritis.2 As a result, the patient is more likely to be seen by a dermatologist before a rheumatologist. Furthermore, a dermatologist’s therapy decision for a psoriasis patient is determined by the presence or absence of PsA.3 A meta-analysis revealed that the prevalence of undiagnosed PsA in psoriasis patients attending dermatology clinics was 17.4%.4 PsA diagnosis is challenging due to the variability of symptoms and the lack of serum biomarkers. A comprehensive evaluation by a rheumatologist is essential for an accurate diagnosis of PsA to prevent misdiagnosis and avoid unnecessary treatment.5 It is therefore crucial to identify psoriasis patients with a higher risk of PsA development to stop the progression of PsA. Clinical predictors of PsA include nail, scalp, and genital psoriasis, obesity, arthralgia, history of uveitis, and having a first-degree relative with PsA.6 However, it is difficult to determine the presence of PsA by evaluating these predictors independently. Sending every psoriasis patient to a rheumatologist may lead to labor, time, and economic losses, therefore dermatologists need to filter patients and refer patients in need to rheumatologists for early diagnosis of PsA. A potential shift in the practice of dermatologists away from the examination of the musculoskeletal system may present challenges in screening for PsA. In this instance, the utilization of screening tools becomes a crucial aspect. Several screening tools were developed that combine clinical predictors and joint complaints to reduce unnecessary patient referrals to rheumatologists.7,8,9,10 Nevertheless, the current screening tools are time-consuming, complex, and have a high false positive rate, which limits their use in dermatological routines.11
As healthcare systems globally encounter challenges such as increased costs, restricted access, and rising demand for personalized care, there is growing evidence to suggest that using AI can assist in resolving these issues.12 In numerous medical disciplines, including dermatology and rheumatology, the utilization of AI for the processing of patient data has the potential to facilitate a more personalized approach to healthcare.13 Furthermore, AI applications have provided regular monitoring and recommendations to patients as medical assistants in chronic diseases such as diabetes, cardiac, and pulmonary diseases.14
A Generative Pretrained Transformer (GPT) is a game-changing form of AI that can produce text that closely resembles a human. OpenAI has developed this AI language model, which is known as ChatGPT.15 It has quickly reached a large number of users, surpassed social media platforms, and has become one of the pioneers of AI.16 This technology has several healthcare applications that improve patient care, research and planning, and treatment options.15,16
The objective of this study was to evaluate the performance of the AI-powered PsA Screening (AIPS) tool, developed by ChatGPT, in detecting psoriatic arthritis (PsA) compared to the validated Psoriasis Epidemiology Screening Tool (PEST) and Early ARthritis for Psoriatic patients (EARP) screening questionnaires.
Materials and Methods
Material and Methods This prospective study included participants over 18 years old with musculoskeletal complaints but without a diagnosis of PsA. Patients with a previous diagnosis of PsA or other rheumatological diseases were excluded from the study. The PEST, EARP, and AIPS questionnaires were tested on 199 psoriasis patients. The diagnosis of psoriasis was based on clinical features and histopathological findings reported by a dermatologist (Ozge Sevil Karstarli Bakay).
We asked ChatGPT to create a custom questionnaire designed to screen for PsA effectively, which was specifically tailored for individuals with psoriasis to either self-administer or share with their healthcare providers. The AIPS comprises questions relevant to peripheral arthritis, axial inflammation, and enthesitis. These questions were selected from multivariate analyses conducted via Chat GPT 4.0. Turkish translations of the PEST and EARP questionnaires are available. Patients were then referred to rheumatologists and examined for clinical signs of axial and peripheral arthritis (enthesopathy, axial spondyloarthritis, and swelling of the fingers and toes). All patients were assessed by three rheumatologists (Umut Bakay, Tugba Izci Duran and Zeynep Dundar Ok) who were blinded to the questionnaire responses. After the initial examination, if PsA was suspected, further investigations (sonography, radiography, and MRI) were performed to confirm the diagnosis. PsA was diagnosed according to the CASPAR (Classification criteria for psoriatic Arthritis) criteria.17
Evaluation of the PEST, EARP, and AIPS Questionnaires PESTThere are five questions: 1. Have you ever had a swollen joint (or joints)? 2. Has a doctor ever told you that you have arthritis? 3. Do your fingernails or toenails have holes or pits? 4. Have you ever had pain in your heel? 5. Have you ever had a finger or toe completely swollen and painful for no apparent reason? The total PEST score was calculated as the sum of the ‘yes’ answers. Univariate and multivariate analyses have shown an increased incidence of PsA in patients with a PEST score >3.13
EARPIt consists of 10 yes/no questions and the cut-off to be considered positive is 3 or higher. 1. Do your joints hurt? 2. Have you taken anti-inflammatory drugs for joint pain more than twice a week in the last 3 months? 3. Do you wake up at night because of back pain? 4. Do you feel stiffness in your hands for more than 30 minutes in the morning? 5. Do your wrists and fingers hurt? 6. Do your wrists and fingers swell up? 7. Has any finger been sore and swollen for more than 3 days? 8. Is your Achilles tendon swelling? 9. Do your feet or ankles hurt? 10. Do your elbows or hips hurt?
AIPS1. Joint pain: Have you had any joint pain in the last month? 2. Morning stiffness: Do you experience stiffness or restricted movement in your joints in the morning? 3. Swollen joints: Have you had swollen joints in the past? 4. Swollen fingers or feet: Have you had complete swelling (like a sausage) of your fingers or feet? 5. Nail changes: Have you noticed pits, discoloration, or other abnormalities in your nails? 6. Eye problems: Have you had any eye redness, pain, or blurred vision? Pain at night and in the morning: Does your joint pain get worse at night or in the morning? 8. Family history: Do you have a family history of psoriatic arthritis or any other inflammatory joint disease?
Scoring3 or more ‘yes’ answers: This indicates that the patient is at high risk of developing psoriatic arthritis and should be referred for rheumatological assessment.
1-2 ‘Yes’ answers: This indicates that the patient is at moderate risk and should be monitored closely. A rheumatological assessment may be considered if necessary.
0 “Yes” answers: This indicates that the patient is at low risk of psoriatic arthritis. However, an assessment should be made in the light of the patient’s clinical symptoms and medical history.
Ethical ApprovalThis study was approved by the Ethics Committee of Pamukkale University (Date: 04.07.2024, Decision No: E.547543).
Statistical AnalysisData are presented as counts and percentages, mean ± standard deviation, or median (min-max). The normality of the distribution of numerical variables was tested with the Shapiro-Wilk test. The independent-samples t-test and the Mann-Whitney U were used for intergroup comparisons of numerical variables. Categorical data were evaluated with the χ2 test and Fisher exact test.
The receiver operating characteristic (ROC) curves were constructed to investigate the diagnostic performance of EARP, PEST, and the newly developed Chat-GPT questionnaire. The area under the curve (AUC) provided a measure of the overall discriminative ability of the prediction rule. The cut-off value was determined with the Youden index (Youden index = sensitivity + specificity - 1) as it is the cut-off value with the highest AUC and aims to maximize the difference between the true positive rate and the false positive rate. The sensitivity and specificity were determined for several cut-off values of the prediction score. A p-value of <0.05 was considered significant.
Statistical analysis was performed with SPSS, version 22.0 (IBM Corp., Armonk, NY, USA).
Reporting GuidelinesThe study was reported in accordance with STARD guideline.
Results
A total of 199 patients (115 [57.8%] female, with a mean age of 44.4 ± 13.3) were enrolled in the study. The prevalence of PsA based on rheumatologist diagnosis was 42.2% (84 patients). The demographic and clinical data of psoriasis patients are shown in Table 1. Out of the patients, 22.6% (n = 45) were diagnosed with fibromyalgia, 15.1% (n = 30) with osteoarthritis, 11.1% with disc herniation, and 9% with nonspecific musculoskeletal complaints.
The comparison between patients with PsA and those without it, as diagnosed by the rheumatologist, showed no significant differences in terms of age, gender, duration of psoriasis disease, or family history (p>0.05). It was found that 18 patients diagnosed with PsA by AIPS were not considered to have PsA by the rheumatologist. Furthermore, PsA patients had significantly higher AIPS, PEST, and EARP scores (p<0.001) (Table 2).
The AIPS (AUC 0.982, p<0.05, 95% confidence interval [CI] 0.967-0.997), PEST (AUC 0.949, p<0.05, 95% CI 0.922-0.975), and EARP (AUC 0.960, p<0.005, 95% CI 0.937-0.984) were identified as predictors of diagnosis of PsA (Figure 1). The AIPS questionnaire demonstrated superior efficacy in predicting the diagnosis of PsA. The Youden index was employed to ascertain the optimal cut-off value for the AIPS score, which was determined to be 4. When the cutoff of 3 was selected for EARP and PEST based on the previous studies7,8 (7, 8), the calculated sensitivity and specificity by the ROC curve are presented in Figure 1. The sensitivity of 98% observed for EARP was superior to that of AIPS and PEST, which exhibited sensitivity values of 92% and 83%, respectively. On the other hand, the specificity of AIPS (96%) was superior to that of PEST and EARP (91% and 80%, respectively).
Discussion
This study demonstrates that the PsA screening tool developed by ChatGPT, which we called AI-powered PsA Screening (AIPS), outperformed the current and validated questionnaires EARP and PEST in predicting PsA. Another important finding of the study is that 42.2% of psoriasis patients with musculoskeletal complaints were diagnosed with PsA.
We asked ChatGPT to create a PsA screening tool to help psoriasis patients and healthcare professionals. The ’’AIPS’’ questionnaire inquired about morning stiffness and axialperipheral joint involvement. In addition to the previous questionnaires, it included questions about eye problems and family history of joint disease, which are risk factors for PsA. ChatGPT, similar to other surveys, only asked about nail involvement and did not ask about cutaneous involvement.
Interestingly, it did not include questions regarding enthesitis, such as heel pain.
Psoriatic arthritis frequently presents as dactylitis, enthesitis, spondylitis, and peripheral arthritis. In established PsA, persistent joint pain is anticipated with or without morning stiffness lasting longer than thirty minutes.18 So, it’s unsurprising that the AIPS, like other screening tools, asks about joint pain, swelling, and morning stiffness.7,8,9,10 However, especially in the early stages, joint pain and morning stiffness may not be as noticeable as in other joint diseases such as rheumatoid arthritis or ankylosing spondylitis.18 Therefore, we speculate that ChatGPT questions characteristics such as eye problems and family history, which are risk factors for PsA and that can be defined by patients themselves, to detect early PsA cases that are not fully clinically established.
Psoriatic disease is a complex inflammatory condition involving skin and joint symptoms, and numerous comorbidities and extra-articular manifestations such as inflammatory bowel disease and uveitis. The prevalence of uveitis is between 2% and 25% of patients with PsA.19 A recent meta-analysis showed an increased risk of uveitis in cases of psoriasis and PsA, with a higher risk in PsA than in psoriasis. The results of this meta-analysis suggested an overall positive bidirectional association between psoriasis and uveitis.20
First-degree relative with PsA is a significant predictor of developing PsA in patients with psoriasis. A cohort study revealed that first-degree relatives of patients with PsA were 39 times more likely to develop PsA than those without a family history.21
Evaluation of enthesitis in patients with psoriasis is important for the diagnosis of PsA, but due to the wide range of signs and symptoms that partially overlap or coexist with the clinical features of fibromyalgia, evaluation of enthesitis by history or physical examination alone may be inadequate. Patient-based evaluations are misleading in the diagnosis of enthesitis and evaluation with ultrasound provides more accurate results.22 Probably, ChatGPT did not include enthesitis-associated questions to increase specificity, since it prepared a patientbased questionnaire.
Following these questions, the AIPS demonstrated an excellent capacity to accurately identify patients with psoriatic arthritis, with a sensitivity of 92% and a specificity of 96%. In comparison, the validated screening tools, namely EARP (sensitivity 98%, specificity 80%) and PEST (sensitivity 83%, specificity 91%), demonstrated satisfactory performance, albeit with slightly lower overall results. In a study comparing four validated screening tools, EARP had the highest sensitivity (91%), similar to ours; the sensitivities of PASE 44, PASE 47, PEST, and ToPAS II were found to be 80%, 76%, 53%, and 44%, respectively. EARP, PASE 44, PASE 47, PEST, and ToPAS II specificities were 88%, 95%, 95%, 95%, and 97% respectively.23 However, a recent systematic review evaluated eleven validated PsA screening tools, including the EARP and PEST. It was found that existing screening tools were not supported by very high-quality evidence of content validity. The main problem they identified with the screening tools was that they lacked items that accurately reflected the full spectrum of the disease to perform a true screening in patients with probable or intact PsA, and there was insufficient information to support item reduction methods.24
It has been reported that in patients with psoriasis, 47% of those in the initial diagnosis period and approximately 80% of those who have completed the five-year disease period present with accompanying musculoskeletal complaints. However, not all these cases are associated with PsA. Other pathologies, such as fibromyalgia and osteoarthritis, can also manifest with these symptoms. In addition, half of the patients who did not have PsA at the time of diagnosis developed PsA symptoms later.25 In the present study, only patients with psoriasis and musculoskeletal complaints were included, and 42.2% of these patients were diagnosed with psoriatic arthritis by rheumatologists. This result indicates that musculoskeletal complaints should not be taken lightly, but that not every patient requires rheumatologist evaluation. Furthermore, dermatologists should incorporate this approach into their routine evaluations, bearing in mind that even if these patients are not diagnosed with PSA, some may develop PsA symptoms in the future. AI is a promising tool for dermatologists, offering a way to detect potential cases of PsA in their busy clinical routines. In our study, AIPS incorrectly diagnosed 18 patients as having PsA despite the absence of PsA. It is important to note that artificial intelligence is not infallible and may err in its assessments. This potential shortcoming can be addressed in the future through the advancement of technology or a reevaluation of the patient at each examination.
Artificial intelligence will certainly bring advantages to healthcare, but it may also lead to ethical and social challenges. Furthermore, it is important to consider that AI algorithms cannot apply a holistic approach to clinical scenarios and cannot fully consider the psychological and social aspects of human nature that are usually considered by skilled healthcare professionals.12
Limitations
The study’s limitation is a relatively small number of patients.
However, its prospective design and multidisciplinary nature are its strengths.
Conclusion
Musculoskeletal complaints in patients with psoriasis do not necessarily indicate the presence of PsA, so it is not always necessary to refer these patients to a rheumatologist. Implementing appropriate screening tools has the potential to reduce economic costs and time loss. AIPS developed by ChatGPT, with 92% sensitivity and 96% specificity, suggests that artificial intelligence is a promising topic in this regard and worth working on.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants prior to inclusion in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
AI Usage Disclosure
ChatGPT was used to create the Artificial Intelligence–Powered PsA Screening questionnaire, which was specifically tailored for individuals with psoriasis to either self-administer or share with their healthcare providers.
Abbreviations
AI: Artificial Intelligence
AIPS: Artificial Intelligence–Powered PsA Screening
AUC: Area Under the Curve
CASPAR: Classification Criteria for Psoriatic Arthritis
CI: Confidence Interval
EARP: Early Arthritis for Psoriatic Patients
MRI: Magnetic Resonance Imaging
PEST: Psoriasis Epidemiology Screening Tool
PsA: Psoriatic Arthritis
ROC: Receiver Operating Characteristic
SPSS: Statistical Package for the Social Sciences
References
-
FitzGerald O, Ogdie A, Chandran V, et al. Psoriatic arthritis. Nat Rev Dis Primers. 2021;7(1):59. doi:10.1038/s41572-021-00293-y
-
Lebwohl M, Langley RG, Paul C, et al. Evolution of patient perceptions of psoriatic disease: results from the Understanding Psoriatic Disease Leveraging Insights for Treatment survey. Dermatol Ther (Heidelb). 2022;12(1):61-78. doi:10.1007/s13555-021-00635-4
-
Mease PJ, Palmer JB, Hur P, et al. Utilization of the validated Psoriasis Epidemiology Screening Tool to identify signs and symptoms of psoriatic arthritis among those with psoriasis: a cross-sectional analysis from the US-based Corrona Psoriasis Registry. J Eur Acad Dermatol Venereol. 2019;33(5):886-892. doi:10.1111/jdv.15443
-
Villani AP, Rouzaud M, Sevrain M, et al. Prevalence of undiagnosed psoriatic arthritis among psoriasis patients: systematic review and meta-analysis. J Am Acad Dermatol. 2015;73(2):242-248. doi:10.1016/j.jaad.2015.05.001
-
Ohta R, Sano C. Challenges in diagnosing psoriatic arthritis in primary care: a meta-ethnographic study. Cureus. 2023;15(11). doi:10.7759/cureus.49443
-
Hioki T, Komine M, Ohtsuki M. Diagnosis and intervention in early psoriatic arthritis. J Clin Med. 2022;11(7):2051. doi:10.3390/jcm11072051
-
Tinazzi I, Adami S, Zanolin EM, et al. The Early Psoriatic Arthritis Screening Questionnaire: a simple and fast method for the identification of arthritis in patients with psoriasis. Rheumatology (Oxford). 2012;51(11):2058-2063. doi:10.1093/rheumatology/kes187
-
Ibrahim GH, Buch MH, Lawson C, Waxman R, Helliwell PS. Evaluation of an existing screening tool for psoriatic arthritis in people with psoriasis and the development of a new instrument: the Psoriasis Epidemiology Screening Tool questionnaire. Clin Exp Rheumatol. 2009;27(3):469-474. doi:10.1002/art.24608
-
Gladman DD, Schentag CT, Tom BD, et al. Development and initial validation of a screening questionnaire for psoriatic arthritis: the Toronto Psoriatic Arthritis Screen. Ann Rheum Dis. 2009;68(4):497-501. doi:10.1136/ard.2008.089441
-
Husni ME, Meyer KH, Cohen DS, Mody E, Qureshi AA. The PASE questionnaire: pilot-testing a psoriatic arthritis screening and evaluation tool. J Am Acad Dermatol. 2007;57(4):581-587. doi:10.1016/j.jaad.2007.04.001
-
Belinchón I, Salgado-Boquete L, López-Ferrer A, et al. Dermatologists’ role in the early diagnosis of psoriatic arthritis: expert recommendations. Actas Dermosifiliogr (Engl Ed). 2020;111(10):835-846.
-
Poalelungi DG, Musat CL, Fulga A, et al. Advancing patient care: how artificial intelligence is transforming healthcare. J Pers Med. 2023;13(8):1214. doi:10.3390/jpm13081214
-
Chinnadurai S, Mahadevan S, Navaneethakrishnan B, Mamadapur M. Decoding applications of artificial intelligence in rheumatology. Cureus. 2023;15(9). doi:10.7759/cureus.46164
-
Subramanian M, Wojtusciszyn A, Favre L, et al. Precision medicine in the era of artificial intelligence: implications in chronic disease management. J Transl Med. 2020;18(1):472. doi:10.1186/s12967-020-02658-5
-
Ferreira RM. New evidence-based practice: artificial intelligence as a barrier breaker. World J Methodol. 2023;13(5):384-389. doi:10.5662/wjm.v13.i5.384
-
Johnson KB, Wei WQ, Weeraratne D, et al. Precision medicine, AI, and the future of personalized health care. Clin Transl Sci. 2021;14(1):86-93. doi:10.1111/cts.12884
-
Taylor W, Gladman D, Helliwell P, et al. Classification criteria for psoriatic arthritis: development of new criteria from a large international study. Arthritis Rheum. 2006;54(8):2665-2673. doi:10.1002/art.21972
-
Savage L, Tinazzi I, Zabotti A, Laws PM, Wittmann M, McGonagle D. Defining preclinical psoriatic arthritis in an integrated dermato-rheumatology environment. J Clin Med. 2020;9(10):3262. doi:10.3390/jcm9103262
-
Novelli L, Lubrano E, Venerito V, et al. Extra-articular manifestations and comorbidities in psoriatic disease: a journey into the immunologic crosstalk. Front Med (Lausanne). 2021;8:737079. doi:10.3389/fmed.2021.737079
-
Li CR, Chen L, Wang LF, et al. Association between uveitis and psoriatic disease: a systematic review and meta-analysis based on the evidence from cohort studies. Int J Ophthalmol. 2020;13(4):650-659. doi:10.18240/ijo.2020.04.19
-
Gottlieb AB, Merola JF. A clinical perspective on risk factors and signs of subclinical and early psoriatic arthritis among patients with psoriasis. J Dermatolog Treat. 2022;33(4):1907-1915. doi:10.1080/09546634.2021.1942423
-
Macchioni P, Salvarani C, Possemato N, et al. Ultrasonographic and clinical assessment of peripheral enthesitis in patients with psoriatic arthritis, psoriasis, and fibromyalgia syndrome: the ULISSE study. J Rheumatol. 2019;46(8):904-911. doi:10.3899/jrheum.171411
-
Mishra S, Kancharla H, Dogra S, Sharma A. Comparison of four validated psoriatic arthritis screening tools in diagnosing psoriatic arthritis in patients with psoriasis: COMPAQ study. Br J Dermatol. 2017;176(3):765-770. doi:10.1111/bjd.14929
-
Landini Enríquez VV, Jurado Santa-Cruz F, Peralta-Pedrero ML, Morales-Sánchez MA. Content validity of psoriatic arthritis screening questionnaires: systematic review. Int J Dermatol. 2020;59(8):902-914. doi:10.1111/ijd.14821
-
Merola JF, Patil D, Egana A, et al. Prevalence of musculoskeletal symptoms in patients with psoriasis and predictors associated with the development of psoriatic arthritis: retrospective analysis of a US claims database. Dermatol Ther (Heidelb). 2023;13(11):2635-2648. doi:10.1007/s13555-023-01025-8
Figures
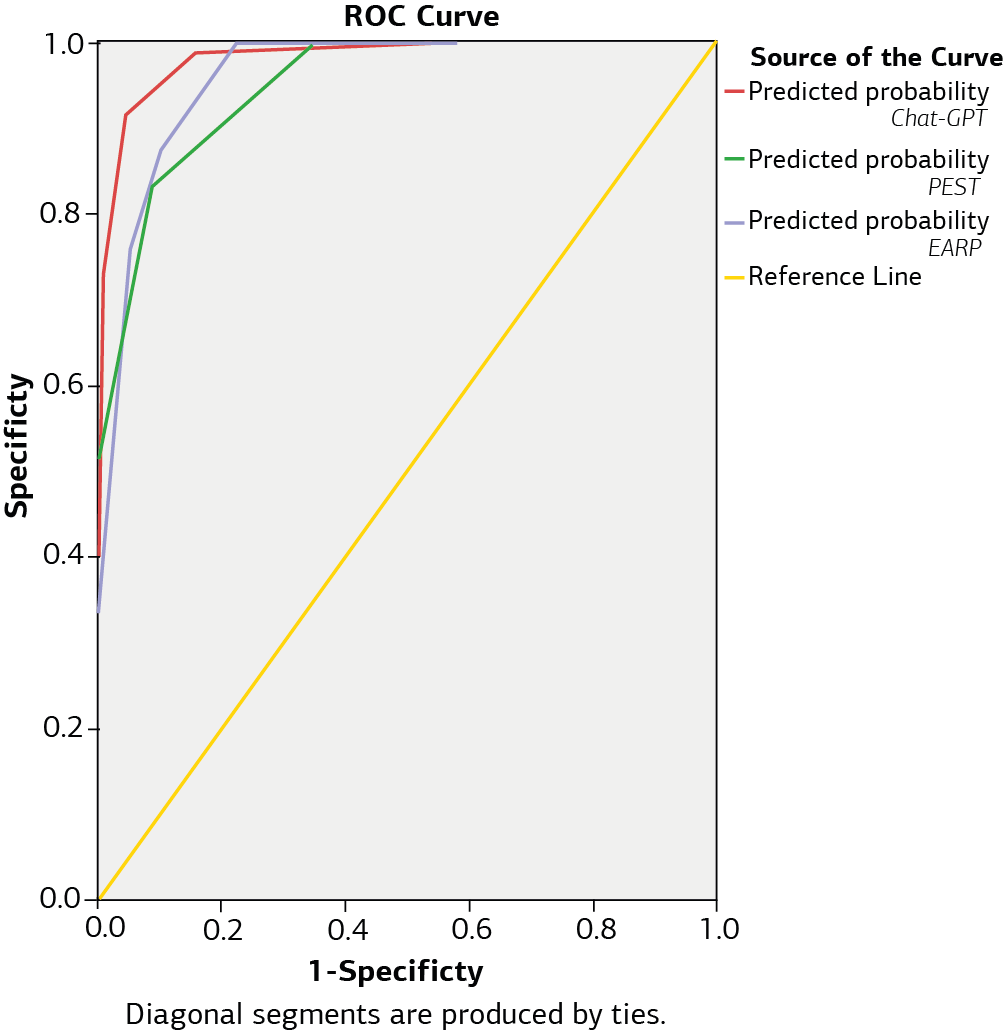
Figure 1. ROC curve analysis: The area under the ROC curve was the largest for the AIPS (ChatGPT)
Tables
Table 1. Demographic and clinical characteristics of psoriasis patients
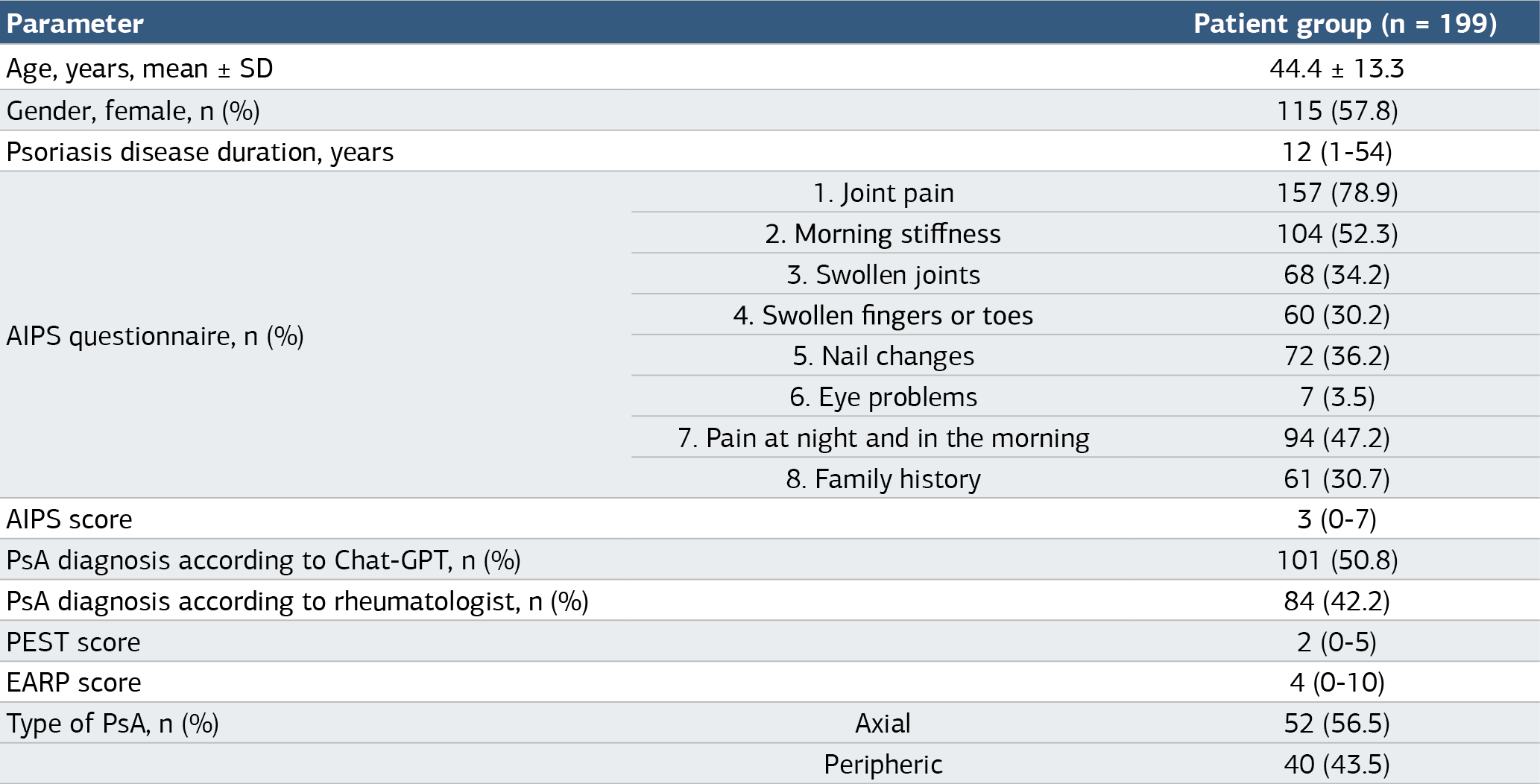
Unless otherwise stated, values are presented as median (min-max).
Table 2. Demographic characteristics of psoriasis patients with and without PsA according to rheumatologist

Unless otherwise stated, values are presented as median (min-max).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Özge Sevil Karstarli Bakay, Umut Bakay, Tuğba İzci Duran, Zeynep Dündar Ok. Ai-powered screening for psoriatic arthritis: a comparative study withexisting tools. Ann Clin Anal Med 2025;16(3):203-208. doi:10.4328/ACAM.22563
- Received:
- January 15, 2025
- Accepted:
- February 23, 2025
- Published Online:
- February 28, 2025
- Printed:
- March 1, 2025