
Preoperative and postoperative evaluation of patients undergoneappendectomies either in spinal or general anesthesia
Spinal anesthesia for appendectomy during COVID-19
Authors
Abstract
AimThe Coronavirus 2019 (COVID-19) pandemic has changed healthcare practices, leading to heightened protective measures and conservative management strategies. In acute appendicitis (AA) cases, conservative surgical and anesthetic approaches, such as spinal anesthesia, were increasingly adopted. However, studies focusing specifically on conventional appendectomy during the pandemic remain limited.
Methods126 patients underwent open appendectomy in a single center retrospectively analyzed. Patients are categorized based on COVID status and anesthesia administrations. Cox regression tests were utilized for analyzing factors affecting longer hospitalization.
ResultsMajor complications (9.8% vs. 25.0%, p=0.044) and ileus development (0.0% vs. 4.1%, p=0.038), CRP levels (23.64 ± 23.54 vs. 64.42 ± 69.41; p<0.001), time to initiate oral feeding (1.24 ± 0.91 vs. 1.54 ± 1.74; p=0.018), length of hospital stay (1.74 ± 1.30 vs. 2.17 ± 3.48; p=0.021), and surgical durations (35.39 ± 6.74 vs. 37.08 ± 12.93; p=0.016) were frequent in COVID-19 positive patients. CRP levels (39.98 ± 54.20 vs. 26.13 ± 26.80; p=0.003), time to initiate oral feeding (1.50 ± 1.60 vs. 1.17 ± 0.65; p=0.002) and length of hospital stay (2.00 ± 2.87 vs. 1.71 ± 0.93; p=0.002) were more frequent in general anesthesia. General anesthesia (OR: 32.337; p<0.001), advanced age (OR: 1.089; p<0.001), perforation (OR: 15.906; p=0.005), and the development of major complications (OR: 33.056; p=0.005) were independent risk factors for prolonged hospital stay in multivariate analysis.
ConclusionOpen Appendectomy under spinal anesthesia was found to be a safe option in patients with AA which also protects both patients and healthcare professionals and lowers hospitalization stays.
Keywords
Introduction
The Coronavirus Disease 2019 (COVID-19) pandemic, since its onset in 2020, has caused significant changes in the behaviors and attitudes of both patients and healthcare professionals. During the pandemic, many outpatient services were temporarily suspended to reduce contact and limit the number of visits, while protective measures were heightened. Patients, on the other hand, developed an instinct to avoid seeking hospital care unless their symptoms were unbearable.1,2,3
In cases of acute appendicitis (AA), which represents the highest emergency surgical workload in general surgery, more conservative approaches were adopted by both surgical and anesthesia teams.4,5 Surgical teams prioritized conservative management strategies, such as close monitoring and antibiotic therapy, while anesthesia teams increasingly preferred sedation or spinal anesthesia instead of general anesthesia.6,7,8
During the pandemic, numerous studies were published on appendicitis cases in which these approaches were adopted. While these studies have evaluated laparoscopic appendectomy, literature focusing on conventional appendectomy remains limited. This study aims to determine the impact of anesthesia method selection on perioperative and postoperative outcomes in acute appendicitis cases treated at a public hospital designated as a “pandemic hospital” during the pandemic period.
Materials and Methods
Study DesignThe study was designed based on patients who presented with acute appendicitis and underwent conventional appendectomy during the pandemic period between 2020 and 2021. Monocentric data collection began after obtaining ethical approval. Since this was a retrospective study, the requirement for informed consent was waived by the ethics committee.
Inclusion CriteriaThe study included patients aged 18 years or older who underwent emergency surgery for AA using conventional methods. Only patients whose surgeries were completed via McBurney modified McBurney (Lanz or Langer incision), or Rockey-Davis incisions were included. Additionally, patients who were directly scheduled for surgery without clinical followup after admission were also included.
Exclusion CriteriaPatients initially managed with medical follow-up despite suspicion of AA and later operated on, those younger than 18 years, patients who underwent exploratory laparotomy or conversion to median laparotomy after the initial incision, and patients diagnosed with phlegmonous appendicitis who only had a drain placed with interval appendectomy planned were excluded from the study. Additionally, patients with incomplete data required for the study were also excluded.
Preoperative VariablesAppendectomy records were extracted from operating room logs throughout the pandemic. Preoperative data collected for these patients included COVID-19 antigen positivity, COVID-19 Reporting and Data System (CO-RADS) scores from computed tomography scans, C-reactive protein (CRP) levels, and oxygen saturation at the time of admission.9,10,11
Additionally history of diabetes, were recorded. Preoperative anesthesia evaluations included American Society of Anesthesiology (ASA) scores and body mass index (BMI) values.12,13
Surgery DataAnesthesia was administered using previously described techniques for both spinal and general anesthesia. During the COVID-19 pandemic, spinal anesthesia was preferred whenever possible. General anesthesia was performed in patients with failed spinal anesthesia, a history of lumbar surgery, or those using anticoagulants.14 All surgeries were initiated using McBurney, modified McBurney (Lanz or Langer incision), or Rockey-Davis incisions. Depending on the patients’ adhesions and presentation, mesocolic or retrocolic dissection was performed to access the appendix base. The base of the appendix was ligated with double-layer silk sutures and subsequently resected. In patients with abscesses, the cavity was irrigated and aspirated. All patients received 2 grams of cefazolin 60 minutes before the surgical incision. Postoperatively, the peritoneal and muscular layers were closed with polyglactin 910 sutures, the fascial layer was repaired with polydioxanone sutures, and the skin was closed with sharp, non-absorbable monofilament sutures.
Oral feeding was initiated after the return of bowel gas passage in the postoperative period. Postoperative management included only analgesics, antiemetics, and fluid replacement. In patients with perforations and significantly elevated CRP levels, metronidazole therapy was started at a dose of 500 mg twice daily. For COVID-19-positive patients, additional treatments were administered according to the Ministry of Health’s suggested guidelines at the time.15
Surgical duration, intraoperative bleeding or abscess presence, and perforated cases were extracted from the surgical records. Additionally, postoperative data, including ileus development, time to oral feeding, fistula formation, superficial incisional surgical site infections, intra-abdominal abscess formation, readmissions, length of hospital stay, and major morbidity were recorded. Major morbidities were defined as complications classified as grade 3 or higher according to the Clavien-Dindo classification.16
Ethical ApprovalThis study was approved by the Ethics Committee of Zonguldak Bülent Ecevit University Faculty of Medicine (Date: 19.12.2024, Decision No: 2024/22/10).
Statistical AnalysisIBM® SPSS® (Statistical Package for the Social Sciences) version 27 (IBM Corp. Armonk, NY, USA) used for statistical analysis. The distribution of numerical data was performed using the Kolmogorov–Smirnov test with the normal distribution results. Qualitative data were presented as frequency and percentage. Continuous measurements were presented as mean and standard deviation (sd). The chi-square test is used for comparisons involving categorical variables. The relationship between continuous parameters with COVID status or anesthesia type was analyzed through the application of the independent t-test. For the analysis of factors influencing longer hospitalization; multivariate Cox regression tests were conducted. A significance level of 0.05 was considered for all tests.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
The study was conducted by compiling data from patients who underwent emergency appendectomy at the Ministry of Health Besni State Hospital between March 2020 and June 2021. Two surgeons and one anesthesiologist were involved in the surgical procedures in this single-center study. Data from a total of 126 surgical patients were collected.
When patients were evaluated based on their COVID-19 status, the majority of COVID-19-positive patients were classified as ASA 3E, while most COVID-19-negative patients were categorized as ASA 1E (p=0.022). In CO-RADS assessments, the frequencies of CO-RADS 4 and 5 were significantly higher in COVID-19-positive patients compared to COVID-19 negative patients (5.8% vs. 33.3% and 0.0% vs. 4.1%, respectively; p<0.001). In admission parameter evaluations, arterial oxygen saturation (SO2) levels were lower in COVID-19-positive patients (16.6% vs. 37.5%; p=0.011). Major complications (9.8% vs. 25.0%, p=0.044) and ileus development (0.0% vs. 4.1%, p=0.038) were also more frequent in COVID-19-positive patients. CRP levels were significantly higher in COVID-19- positive patients (23.64 ± 23.54 vs. 64.42 ± 69.41; p<0.001). Additionally, the time to initiate oral feeding (1.24 ± 0.91 vs. 1.54 ± 1.74; p=0.018), length of hospital stay (1.74 ± 1.30 vs. 2.17 ± 3.48; p=0.021), and surgical durations (35.39 ± 6.74 vs. 37.08 ± 12.93; p=0.016) were longer in COVID-19 positive patients. Other parameters showed similar distributions (Table 1).
When patients were evaluated based on the chosen anesthesia method, overweight (35.4% vs. 20.5%) and obese patients (14.5% vs. 6.4%) were more frequently observed in the general anesthesia group (p=0.037). Among perioperative findings, perforated appendicitis (31.2% vs. 11.5%; p=0.006) and bleeding cases (8.3% vs. 0.0%; p=0.010) were more common in the general anesthesia group. CRP levels were higher in the general anesthesia group (39.98 ± 54.20 vs. 26.13 ± 26.80; p=0.003), and both the time to initiate oral feeding (1.50 ± 1.60 vs. 1.17 ± 0.65; p=0.002) and length of hospital stay (2.00 ± 2.87 vs. 1.71 ± 0.93; p=0.002) were longer. However, surgical durations were similar between the two groups (36.87 ± 10.03 vs. 35.00 ± 6.88; p=0.099). Other variables were evenly distributed between the groups (Table 2).
To evaluate length of hospital stay, regression analysis was conducted using both the parameters found to be significant in each group and other known influencing factors from the literature, such as fistula at the appendix base, surgical duration, and surgical site incisions.17,18,19,20,21 Univariate analysis identified general anesthesia use (OR: 4.211; p<0.001), age (OR: 1.038; p=0.015), elevated CRP levels (OR: 0.989; p=0.031), surgical duration (OR: 0.947; p=0.031), the presence of perforation (OR: 4.857; p=0.001), and the development of major complications (OR: 8.211; p=0.002) as significant risk factors. Variables found to be significant were included in a multivariate analysis, which demonstrated that general anesthesia use (OR: 32.337; p<0.001), advanced age (OR: 1.089; p<0.001), perforation (OR: 15.906; p=0.005), and the development of major complications (OR: 33.056; p=0.005) were independent risk factors for prolonged hospital stay (Table 3).
Discussion
Our study shows similar perioperative findings and postoperative follow-up data were observed compared to patients who underwent general anesthesia in cases where appendectomy was performed under spinal anesthesia, While morbidity rates were comparable between the two groups, patients receiving spinal anesthesia had shorter hospital stays. Our study demonstrated that, during the COVID-19 pandemic, the preference for spinal anesthesia in appendectomies contributed to reduced hospital stays, thereby lowering the workload and potentially reducing morbidity for both patients and healthcare workers. This suggests that spinal anesthesia can be a suitable option for appendectomy in appropriate patients.
The COVID-19 pandemic has left striking impacts not only on medical history but also on modern world history. Throughout the pandemic, many physicians and healthcare professionals worked selflessly to manage the crisis. In our country, physicians took on the care of COVID-19 patients outside their specialties during the crisis management process. Beyond this increased workload, the global effects of the pandemic disrupted international trade, causing delays in the supply of medications and medical devices.22,23
Conventional appendectomy is increasingly being replaced by laparoscopic appendectomy in modern surgical practice. However, during global crises like the COVID-19 pandemic, where the availability and supply of medical equipment may be disrupted, conventional appendectomy remains a reliable alternative. It can be easily performed with a single surgical set and basic sutures, ensuring its continued relevance in resourcelimited situations.2,4
When evaluating other studies in the literature, one study comparing the pre-pandemic and post-pandemic periods reported an increase in complicated appendicitis cases from 8.0% to 33.9% after the pandemic. Although this shift aimed to prioritize the safety of both patients and healthcare professionals by managing cases more conservatively, the study found that the incidence of perforated and phlegmonous appendicitis was higher post-pandemic. Additionally, hospital stays for appendectomy patients were shown to be longer after the pandemic.2
During the pandemic, studies on appendectomy primarily focused on patients operated on under spinal anesthesia, often evaluating laparoscopic surgeries or combining two surgical techniques. A multicenter analysis from Italy reported that the conversion rate to open surgery in patients with complications was 2.4 times higher, and open surgery was performed 2.24 times more frequently.24 In a single-center study conducted in Turkey, 588 patients presenting with acute appendicitis were included, and an increase in conversion from laparoscopy to open surgery was observed in cases of perforated appendicitis. Both studies demonstrated that hospital stays were prolonged in cases of perforated appendicitis.25 Similarly, our study also showed that perforated appendicitis significantly prolonged the length of hospital stay.
Studies comparing only open appendectomy cases are limited. There is only one case series that specifically evaluates these patients. In that series, no major complications were reported among the 11 operated cases, and hospital stays were described as short. Similarly, our study demonstrated that general anesthesia does not increase major complications or prolong hospital stays, consistent with the findings of this series. However, unlike the previous study, our research included a larger patient population. Additionally, by including patients with positive COVID-19 antigen tests or CO-RADS imaging findings, our study uniquely evaluated outcomes specific to the pandemic context.4
Limitations
Our study has several limiting factors. First, it was designed as a retrospective study. Due to the restricted availability of medical equipment during the pandemic, laparoscopic surgery cases were excluded because of technical limitations at the center where the study was conducted. Lastly, the exact onset times of patients’ symptoms were unknown and therefore could not be included in the analysis. As a strength, the study exclusively focused on a single surgical method, evaluated in a single center by the same surgical team, ensuring consistency in the findings. Also as a technique comparison; interval appendectomy or medical approach patients weren’t included which contributes to a more homogenous patient cohort.
Conclusion
Open appendectomy performed under spinal anesthesia demonstrates similar morbidity rates to those under general anesthesia while resulting in shorter hospital stays. Although open appendectomy has largely been replaced by laparoscopy in modern practice, it remains a safe and reliable option under spinal anesthesia during crisis periods, such as the COVID-19 pandemic, when access to minimally invasive techniques may be limited or delayed.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
The requirement for informed consent was waived by the Ethics Committee due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
AA: Acute appendicitis
ASA: American Society of Anesthesiologists
BMI: Body mass index
CO-RADS: COVID-19 Reporting and Data System
COVID-19: Coronavirus disease 2019
CRP: C-reactive protein
DM: Diabetes mellitus
OR: Odds ratio
SI-SSI: Superficial incisional surgical site infection
SO2: Arterial blood oxygen saturation
References
-
Akrida I, Verras GI, Bouchagier K, et al. The impact of the COVID-19 pandemic on the number of patients presenting with appendicitis to the emergency department. Prz Gastroenterol. 2024;19(2):194-197. doi:10.5114/pg.2023.129495
-
Turhan N, Arıcan CD. The effects of the COVID-19 pandemic on patients with acute appendicitis. Ulus Travma Acil Cerrahi Derg. 2022;28(6):756-761. doi:10.14744/tjtes.2021.53929
-
Ergun E, Sozduyar S, Gurbanova A, et al. An indirect effect of the COVID-19 pandemic: increased pediatric perforated appendicitis rate due to delayed admission. Turk J Surg. 2021;37(4):318-323.
-
Mai DVC, Sagar A, Claydon O, Park JY, Tapuria N, Keeler BD. Open appendicectomy under spinal anesthesia: a valuable alternative during COVID-19. Surg J (N Y). 2021;7(2). doi:10.1055/s-0041-1725933
-
Boleken ME, Günendi T, Kocaman OH, Dogan F, Karahan MA. How the COVID-19 pandemic affects our perspective on the medical treatment of acute appendicitis in children. J Pediatr Surg. 2022;57(4):780-781. doi:10.1016/j.jpedsurg.2021.10.009
-
Lock JF, Wiegering A. Changes in the management of acute appendicitis during the COVID-19 pandemic. Langenbecks Arch Surg. 2021;406(2):503-504. doi:10.1007/s00423-021-02099-8
-
Choi YS, Yi JW, Chung CTY, Shin WY, Choi SK, Heo YS. Clinical experience of emergency appendectomy under the COVID-19 pandemic in a single institution in South Korea. Medicina (Kaunas). 2022;58(6):783. doi:10.3390/medicina58060783
-
Bedwani NH, Smith C, Kelada M, et al. Two-year outcomes of conservatively managed appendicitis during the COVID-19 pandemic: a multicentre cohort study. Langenbecks Arch Surg. 2023;408(1):307.
-
Yamayoshi S, Sakai-Tagawa Y, Koga M, et al. Comparison of rapid antigen tests for COVID-19. Viruses. 2020;12(12):1420. doi:10.3390/v12121420
-
Drago F, Gozzo L, Li L, Stella A, Cosmi B. Use of enoxaparin to counteract COVID-19 infection and reduce thromboembolic venous complications: a review of the current evidence. Front Pharmacol. 2020;11:579886. doi:10.3389/fphar.2020.579886
-
Ali AM, Rostam HM, Fatah MH, Noori CM, Ali KM, Tawfeeq HM. Serum troponin, D-dimer, and CRP level in severe coronavirus (COVID-19) patients. Immun Inflamm Dis. 2022;10(3). doi:10.1002/iid3.582
-
Abbassi F, Pfister M, Lucas KL, et al. Milestones in surgical complication reporting: Clavien-Dindo Classification 20 years and Comprehensive Complication Index 10 years. Ann Surg. 2024;280(5):763-771. doi:10.1097/sla.0000000000006471
-
Austin TM, Miller BE. BMI- and age-related associations with mortality from COVID-19. Anaesthesia. 2022;77(1):107. doi:10.1111/anae.15478
-
Erdem VM, Donmez T, Uzman S, Ferahman S, Hatipoglu E, Sunamak O. Spinal/epidural block as an alternative to general anesthesia for laparoscopic appendectomy: a prospective randomized clinical study. Wideochir Inne Tech Maloinwazyjne. 2018;13(2):148-156. doi:10.5114/wiitm.2018.72684
-
Bartoletti M, Azap O, Barac A, et al. ESCMID COVID-19 living guidelines: drug treatment and clinical management. Clin Microbiol Infect. 2022;28(2):222-238. doi:10.1016/j.cmi.2021.11.007
-
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205-213. doi:10.1097/01.sla.0000133083.54934.ae
-
Bancke L, Maak M, Langheinrich M, et al. Risk factors for postoperative morbidity, prolonged length of stay, and hospital readmission after appendectomy for acute appendicitis. Eur J Trauma Emerg Surg. 2023;49(3):1355-1366.
-
Clemente-Gutiérrez U, Santes O, Sarre-Lazcano C. ERAS for appendectomy: a model that is here to stay. Cir Cir. 2019;87(5):600-601.
-
Zhang P, Zhang Q, Zhao H, Li Y. Factors affecting the length of hospital stay after laparoscopic appendectomy: a single-center study. PLoS One. 2020;15(12). doi:10.1371/journal.pone.0243575
-
Panahi A, Bangla VG, Divino CM. Diabetes as a risk factor for perforated appendicitis: a national analysis. Am Surg. 2023;89(2):204-209. doi:10.1177/00031348221124334
-
Calpin GG, Hembrecht S, Giblin K, Hehir C, Dowling GP, Hill ADK. The impact of timing on outcomes in appendicectomy: a systematic review and network meta-analysis. World J Emerg Surg. 2024;19(1):24. doi:10.1186/s13017-024-00549-4
-
Haldane V, De Foo C, Abdalla SM, et al. Health systems resilience in managing the COVID-19 pandemic: lessons from 28 countries. Nat Med. 2021;27(6):964-980. doi:10.1038/s41591-021-01381-y
-
Yeoh K, Wu Y, Chakraborty S, et al. Global health system resilience during encounters with stressors: lessons learnt from cancer services during the COVID-19 pandemic. Clin Oncol (R Coll Radiol). 2023;35(4). doi:10.1016/j.clon.2023.01.004
-
Sartori A, Podda M, Botteri E, et al. Appendectomy during the COVID-19 pandemic in Italy: a multicenter ambispective cohort study by the Italian Society of Endoscopic Surgery and new technologies (the CRAC study). Updates Surg. 2021;73(6):2205-2213. doi:10.1007/s13304-021-01126-z
-
Sevinc MM, Karagulle OO, Kaya R, Erturk C, Dogan S. Evaluation of the appendectomy cases performed under emergency conditions during the COVID-19 pandemic and discussed with the pathology reports. Ulus Travma Acil Cerrahi Derg. 2022;28(5):703-710.
Tables
Table 1. Patient characteristics based on COVID-19 status

COVID-19: Coronavirus Disease 2019, ASA: American Society of Anesthesiologists, BMI: Body Mass Index, DM: Diabetes, HT: Hypertension, CAD: Coronary Artery Disease, COPD: Chronic Obstructive Pulmonary Disease, CO-RADS: COVID-19 Reporting and Data System, SO2: Arterial Blood Oxygen Saturation, SI-SSI: Superficial Incisional Surgical Site Infection, CRP: C-Reactive Protein, †: Chi-Square Test, ‡ Indipendent t Test, *: p ≤0.05, **: p ≤0.01, ***: p ≤0.001
Table 2. Patient characteristics based on anesthesia type
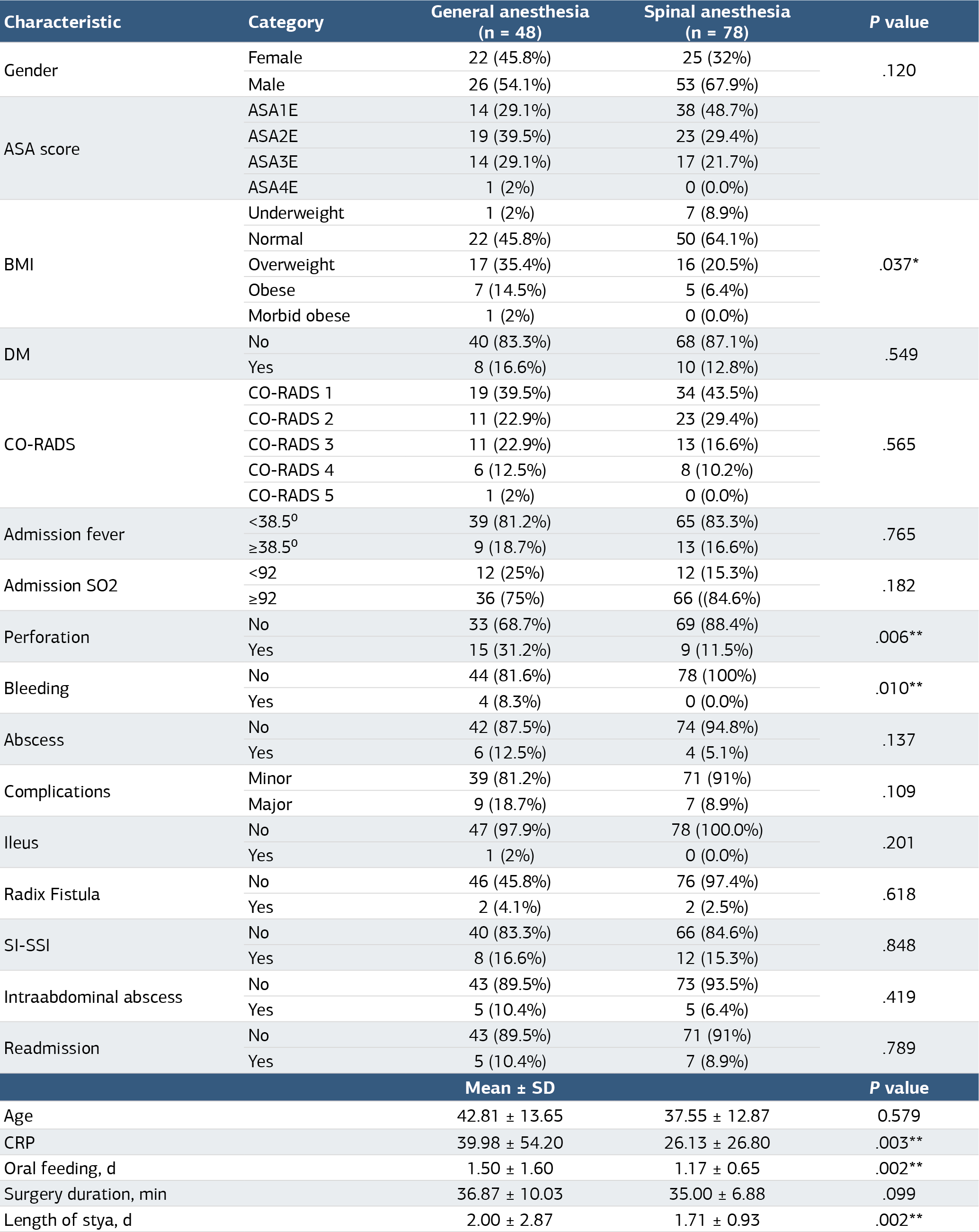
COVID-19: Coronavirus disease 2019, ASA: American Society of Anesthesiologists, BMI: Body mass index, CAD: Coronary artery disease, COPD: Chronic obstructive pulmonary disease, CO-RADS: COVID-19 reporting and data system, CRP: C-reactive protein, DM: Diabetes mellitus, HT: Hypertension, SI-SSI: Superficial incisional surgical site infection, SO2: Arterial blood oxygen saturation, †: Chi-square test, ‡: Independent t test, *: P ≤0.05, **: P ≤0.01, ***: P ≤0.001.
Table 3. Regression analysis of factors associated with discharge within 24 hours after surgery

ASA: American Society of Anesthesiologists, BMI: Body mass index, CI: Confidence interval, CO-RADS: COVID-19 reporting and data system, COVID-19: Coronavirus disease 2019, CRP: C-reactive protein, DM: Diabetes mellitus, OR: Odds ratio, SI-SSI: Superficial incisional surgical site infection, SO2: Arterial blood oxygen saturation, *: P ≤0.05, **: P ≤0.01, ***: P ≤0.001.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
İsa Caner Aydın, Saadet Kılıç, Emine Özdemir. Preoperative and postoperative evaluation of patients undergoneappendectomies either in spinal or general anesthesia. Ann Clin Anal Med 2025;16(3):214-220. doi:10.4328/ACAM.22571
- Received:
- January 19, 2025
- Accepted:
- February 17, 2025
- Published Online:
- February 26, 2025
- Printed:
- March 1, 2025