
Videoscope visualization and videoscope-assisted minimally invasive surgery in dentistry: a narrative review
Videoscope and dentistry
Authors
Abstract
A variety of magnification systems are applied in the field of dentistry to facilitate surgical procedures in a limited area. The development of the videoscope device has been intended to overcome various disadvantages that occur during surgical operations. The purpose of this review is to discuss 1) the use of videoscope-assisted minimally invasive surgery in periodontology and 2) the usage of videoscope in dentistry. An electronic search of literature published in English was carried out by two reviewers. Although videoscope usage has been documented to result in favourable outcomes, particularly in periodontal minimally invasive surgeries, further well-designed studies are recommended to provide more robust evidence.
Keywords
Introduction
In periodontics, minimally invasive surgery (MIS) was first described in 1995 to minimize surgical flap reflection, increase the patient’s postoperative comfort, and achieve better clinical results in the regenerative treatment of periodontal intrabony defects.1 Thereafter, variations in MIS techniques were described, such as minimally invasive surgery technique (MIST),2 modified-MIST3, and entire papilla preservation technique.3,4 In MIS techniques, the small flap is generally elevated with a single-surface approach utilizing different flap designs to position the periosteum approximately 1-2 mm apical to the coronal aspect of the alveolar bone and limit the number of sutures required following surgery.2,3,4,5,6 Since indications for MIS techniques are primarily for the treatment of isolated interproximal periodontal intrabony defects, MIS procedures are usually completed with the use of graft materials and biomimetic agents such as enamel matrix derivate (EMD).7,8 It has been reported that patient morbidity and discomfort are low while clinical success rates are high utilizing these techniques.3,9 However, due to the size limitations associated with the flap design for MIS procedures, attempts have been made to improve surgical visualization with the help of devices such as dental loupes and flexible fiber optic endoscopes.2,10,11,12,13 Moreover, magnification with a surgical microscope can limit surgical access and restrict visualization to a buccal approach, which places limitations on surgical flap design for all variations of MIS.
A review of the literature reported that the ideal imaging device for periodontal surgery is expected to be small enough to allow a very small surgical incision and to be able to provide direct visualization and easy maneuvering throughout the entire surgical field.13 To increase visualization of the surgical field, the videoscope device utilizes a small camera with adjustable lighting, which can be placed into intra-bony defects utilizing either buccal or lingual elevated flaps.8 The camera has a magnification value up to 40X, and utilizing its 2.7 mm carbon fiber retractor attachment, the camera can be easily rotated and adapted to most surgical fields.8 AirShield® technology, a low-pressure air flow, is passed over the camera lens to ensure that direct surgical visualization is not blocked by blood, debris, and fogging [available at: https://microsightdental.com/wpcontent/themes/microSight/images/MicroSight-Datasheet-201910.pdf].
Limited studies/case reports utilizing this technique/technology have been published. The purpose of this narrative review is to discuss the literature published to date regarding videoscope-assisted minimally invasive surgery (VMIS) and the use of videoscope in dentistry.
Materials and Methods
Due to the design and presentation of this study as a narrative review, there is no need for ethics committee approval.
Focused QuestionWhat are the clinical outcomes when using the videoscope in periodontal regenerative surgery? Can the videoscope device be used in other branches of dentistry?
Information SourcesAn electronic search of literature published in English between January 1977 and June 2024 was carried out by 2 reviewers (B.G.A and H.A) using PubMed, Google Scholar, Scopus, and the University of Illinois Chicago Library Database. Reference lists of studies were also hand-searched for relevance. The MeSH terms used for the search included ‘videoscope’ OR ‘videoscope-assisted minimal invasive surgery’ OR ‘videoscope and dentistry’.
Selection CriteriaStudies were included for the review if the following inclusion criteria were fulfilled:
1. Studies specific to the use of a videoscope in dentistry, 2. In vitro and in vivo studies relevant to videoscope in dentistry, and 3. Written in English.
Videoscope methods used outside the field of dentistry, applications with other magnification devices used other than the videoscope device, and non-English literature were excluded from this study.
Statistical AnalysisNo statistical analysis was performed in this study because it is a narrative review based on previously published literature.
Ethics ApprovalEthical approval was not required for this study because it is a narrative review and does not involve human participants or animal subjects.
Reporting GuidelinesThis manuscript was prepared and reported as a narrative review of the existing literature.
Results
Data Extraction ResultsThe following data were extracted from selected clinical studies: authors and year of publication, study design, number of patients and interproximal defects, age, surgical treatment type, biomaterial for regenerative treatment, the mean probing depth (PD), clinical attachment level (CAL) and gingival recession (GR) before treatment (T0) and last follow-up sessions (T1)(Table 1).
As a result of the literature search, a total of 572 articles related to keywords were found. When the abstracts of the studies were evaluated, it was found that a total of 17 articles were related to the videoscope. Of these articles, two book chapters, four reviews, and two manuscripts related to forensic studies were excluded. A total of 9 articles were included for evaluation in this study. Evaluation of the risk of reporting bias is not performed because of the single randomized-controlled study.
Videoscope-Assisted Minimal Invasive Surgery TechniqueThe VMIS surgical technique was first presented in the literature in 2013.8 This study provided proof of principle and introduced the device and surgical technique (Figure 1). VMIS utilizes the following criteria (1) a single small lingual flap design, (2) split thickness incisions, (3) avoiding the use of a periosteal elevator, (4) retaining the buccal papilla and esthetic facial gingiva intact and unreflected whenever possible, and (5) simple suturing techniques avoiding passage of sutures through the marginal tissue of the incision.14 In the current protocol, amelogenins (Emdogain®, Straumann, Basel, Switzerland) and particulate bone allografts are utilized. If surgical incision was performed correctly, the facial papilla remains intact, and the videoscope retractor tip can be inserted into the defect without interference. Granulation tissues are removed, and deposits of calculus on the root surface are easily detected using the videoscope, permitting thorough mechanical root debridement due to the 20-40X magnification image projected onto a video display. Thereafter, 24% ethylenediaminetetraacetic acid (EDTA) is applied on the root surface, and the regenerative treatment of the intra-bony defect is completed with the application of EMD/graft material (Figure 2).8 The use of EMD alone or in combination with bone particulate is common in other forms of minimal invasive surgeries.7,8,9,10,11,12 However, a membrane cannot be applied using MIS due to the limited incisions and flap reflection.9,13 Care must be taken not to overfill the defect with graft materials, which will prevent primary wound closure and likely result in graft material exposure to the oral environment.
Periodontal Regenerative Surgery In the first case series published on VMIS, 29 intra-bony defects were evaluated. EMD was applied to all defects, and 6-month results were reported. A significant decrease in mean PD and mean CAL values without changes in mean GR compared to the baseline values was reported.8 It is notable that studies on other MIS techniques emphasize that GR occurs, although at a minimum rate.12,15,16
A case series reported outcomes on systemically healthy patients with interproximal periodontal defects ≥ 5 mm, clinical attachment loss ≥ 2 mm, and bone loss detected radiographically after Phase-I treatment.16 A total of 30 patients and 110 defects were included in the study, and intra-bony defects were classified according to the number of walls: 64 had one-wall defects, 44 had two-wall defects, and two had three-wall defects. PD, CAL, and GR values before and after treatment were recorded.16 The VMIS protocol was used in all cases, including application of EDTA to the root surface, followed by application of EMD + cortical freeze-demineralized dried bone allograft into the intra-bony defect. At 6 months, PD and CAL values decreased significantly compared to the initial values in single-, two-, and three-walled defects, while no significant difference in GR was noted.16 A follow-up study reported 12 month outcomes on the same patient cohort and included patient morbidity data and the analyzes performed on 18 patients and 26 defects, there was no significant difference in PD and CAL values between the 6 and 12 months in all patient groups while statistically significant differences were maintained to 12 months compared to baseline and no significant changes in GR were observed.17 When postoperative pain was measured using a Visual analog scale (VAS), 1/30 (3.3%) reported a VAS value between 1 and 3 within the first two weeks post-surgery.17 Moreover, 36-month results of the same patient cohort on 14 patients were reported. When changes between baseline to 36 months were evaluated, statistically significant differences in PD and CAL were maintained during the 3-year follow-up period, with no significant difference in GR values.18
Detection of Root Surface Anomalies and Calculus with VideoscopeThe videoscope was used to determine the frequency of microgrooves associated with osseous defects in patients and dried skulls.19 In vitro, 69 sites with vertical bone loss were identified and evaluated in 200 dried skulls using the videoscope. Using 66 consecutive videos takes from VMIS surgeries, 50 teeth (79%) were found to have microgrooves. The authors concluded that microgrooves may represent a risk factor for site-specific progression of periodontal destruction.19 Significantly, the ability to visualize and magnify the surgical field using the videoscope played a large part in identifying the microgrooves, which would otherwise be difficult to detect using other forms of magnification.
Magnification of root surfaces during VMIS procedures identified small deposits of material resembling calculus, termed micro islands of calculus. To verify that these were indeed residual calculus deposits and if they can be removed with chelating agents, 22 teeth with heavy calculus were included in an ex vivo study using the videoscope. Following tooth extraction, one root surface per tooth was selected, and 5 mm² areas were marked for evaluation. A 655-nm diode laser was utilized for fluorescent detection of calculus. Digital images of the marked evaluation area were made using the videoscope.20 After the removal of visible calculus using 3.5X surgical loops, ultrasonic scaler, and gracey curettes, the test area was burnished with EDTA for 30 seconds, and imaging was repeated. Results indicated that micro islands of calculus remain on root surface after instrumentation using 3.5X magnification despite obtaining a visually “clean” surface. The study showed that there was a statistically significant difference in calculus deposits before and after the application of EDTA using both the videoscope and laser fluorescence imaging. Thus, the application of EDTA for 30 seconds after scaling and root planning (SRP) was useful in reducing or eliminating micro islands of calculus on tooth root surfaces.20
In a randomized-controlled, split-mouth clinical study, Dunegan et al. sought to determine if the videoscope can be used as a visual adjunct to SRP in combination with MIS.21 Twenty-five pairs of periodontally hopeless teeth with PD ≥ 5 mm and heavy calculus scheduled for extraction were randomly assigned to either scaling and root planing with minimal surgical access using 3.5X surgical loupes (control) or the videoscope (test). In 89 interproximal areas evaluated, residual calculus ratio was visually detected in 2.61% and 2.71% of the control and test groups, respectively, with no significant difference observed.21 The study confirmed a significant relationship between maximum PD and the percentage of calculus remaining on root surfaces. When the surgical duration was evaluated, a statistically significant difference was observed.21
Peri-implantitis TreatmentThere is only one case report in the literature regarding the use of VMIS in the surgical treatment of peri-implantitis. In a 67-year-old healthy female patient, a PD value of 10+ mm was detected on a cemented-retained, tissue-level maxillary dental implant, which had been functional for 6 years. Following VMIS flap elevation, excess cement and granulation tissues were removed. A demineralized freeze-dried bone allograft with EMD was placed in the bone defect. At the one-year follow-up, PD was 3 mm, and GR was 2 mm, with improvements in radiographic outcomes noted.22
The Use of the Videoscope in Endodontic TreatmentsA study compared dental operating microscope (DOM), surgical loupes, and high-resolution videoscope devices in terms of depth of field, resolution, effects on fine motor skills, and endodontist preference.23 Results indicated that DOM showed significantly higher and better accuracy values than either the videoscope or surgical loupes. Residents achieved more acceptable results than dental students when using DOM or dental loupe. However, there was no significant difference between students and residents in the use of the videoscope. The shortest operation time was associated with surgical loupes, while the videoscope had the longest operating time. Survey results emphasized that using DOM was easier in terms of visualization, time efficiency, ergonomics, and orientation. This study noted that the most negative aspect of using the videoscope was related to hand fatigue and orientation.23
Discussion
The videoscope was patented and introduced in 20138; however, a review of the literature noted very limited publications on this topic. When clinical studies were evaluated, only one randomized controlled clinical study was found that specifically evaluated MIS treatment in periodontics but was aimed at evaluating residual calculus on extracted teeth and to determine if EDTA was useful in removing micro islands of calculus. No clinical measurements were presented.21 As such, there is a need to conduct randomized-controlled clinical studies in which clinical, radiographic, and biochemical analysis of the effectiveness of VMIS treatment can be measured. In the literature, VMIS has generally been used with interproximal vertical defects, which may have created the notion that utilization of the videoscope and VMIS technique has a limited surgical indication. There is a need to evaluate the utility of this instrument in other periodontal/peri-implant procedures and indications.
The prevalence of peri-implantitis is increasing, and a systematic review reported that the prevalence was 12.53% in implant-based and 19.53% in patient-based cases.24 The videoscope may be useful in the treatment of peri-implantitis, especially in evaluating the areas between implant threads using a minimally invasive approach. This stands as another area in need of further research.
Limitations
Studies related to the VMIS technique evaluated a single graft material and/or EMD.8,16,17,18 However, as a limitation, characteristics of the graft material and/or brand were not reported. Therefore, the application of different graft materials, such as putty or particulate biomaterials, with the VMIS technique should be evaluated in future studies. In endodontics, a study reported that endodontic surgery and retrograde approaches with dental operating microscopes were quite difficult in posterior teeth.25 In cases where the field of view is narrow, the direct visualization feature of the videoscope and clear field of view may be an advantage.
The interpretation of non-invasive and invasive interventions and conservative and complicated interventions often depends on surgeon experiences.26 Thus, very limited information can be obtained by only using VAS evaluation aspect of surgeon and patient’s perceptions. The number of randomized controlled studies on the use of videoscopes in minimally invasive surgery and other related fields is relatively limited, and the results of these studies are often contradictory due to the lack of available data.
Conclusion
Although MIS associated with the videoscope has been used successfully in different surgical applications in the clinic, the quality of the studies needs to be improved. Further research is necessary to reach a conclusion regarding the efficacy and safety of videoscopes. Large multicenter clinical studies using the videoscope and VMIS technique should include patient and clinician perception to go along with clinical and biological findings.
Declarations
Ethics Declarations
This article is a narrative review of previously published studies and does not involve any new studies with human participants or animals performed by the authors.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was not required as this study does not include any individual patient data.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: B.G.A., S.N.
Methodology: B.G.A., H.A.
Literature Search and Data Curation: B.G.A., H.A.
Writing – Original Draft Preparation: B.G.A.
Writing – Review & Editing: S.N., T.F.T.
Supervision: S.N., T.F.T.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
CAL: Clinical Attachment Level
DOM: Dental Operating Microscope
EDTA: Ethylenediaminetetraacetic Acid
EMD: Enamel Matrix Derivative
GR: Gingival Recession
MIS: Minimally Invasive Surgery
PD: Probing Depth
RCT: Randomized Controlled Trial
SRP: Scaling and Root Planing
VAS: Visual Analog Scale
VMIS: Videoscope-Assisted Minimally Invasive Surgery
References
-
Harrel SK, Rees TD. Granulation tissue removal in routine and minimally invasive procedures. Compend Contin Educ Dent. 1995;16(9):960-964.
-
Cortellini P, Tonetti MS. A minimally invasive surgical technique with an enamel matrix derivative in the regenerative treatment of intra-bony defects: A novel approach to limit morbidity. J Clin Periodontol. 2007;34(1):87-93.
-
Cortellini P, Tonetti MS. Improved wound stability with a modified minimally invasive surgical technique in the regenerative treatment of isolated interdental intrabony defects. J Clin Periodontol. 2009;36(2):157-163.
-
Aslan S, Buduneli N, Cortellini P. Reconstructive surgical treatment of isolated deep intrabony defects with guided tissue regeneration using entire papilla preservation technique: A prospective case series. J Periodontol. 2021;92(4):488-495.
-
Windisch P, Iorio-Siciliano V, Palkovics D, Ramaglia L, Blasi A, Sculean A. The role of surgical flap design on the healing of intrabony defects treated with an enamel matrix derivative: A 12-month two-center randomized controlled clinical trial. Clin Oral Investig. 2022;26(2):1811-1821.
-
Pasqualini E, Castro F, Curado D, et al. Minimally invasive periodontal regeneration with the buccal approach: A systematic review and meta-analysis of clinical studies. Evid Based Dent. 2024;25(1):54.
-
Aslan S, Buduneli N, Cortellini P. Clinical outcomes of the entire papilla preservation technique with and without biomaterials in the treatment of isolated intrabony defects: A randomized controlled clinical trial. J Clin Periodontol. 2020;47(4):470-478.
-
Harrel SK, Wilson TG Jr, Rivera-Hidalgo F. A videoscope for use in minimally invasive periodontal surgery. J Clin Periodontol. 2013;40(9):868-874.
-
Cortellini P. Minimally invasive surgical techniques in periodontal regeneration. J Evid Based Dent Pract. 2012;12(3 Suppl):89-100.
-
Harrel SK, Wilson TG, Nunn ME. Prospective assessment of the use of enamel matrix proteins with minimally invasive surgery. J Periodontol. 2005;76(3):380-384. doi:10.1902/jop.2005.76.3.380
-
Harrel SK, Wilson TG Jr, Nunn ME. Prospective assessment of the use of enamel matrix derivative with minimally invasive surgery: 6-year results. J Periodontol. 2010;81(3):435-441.
-
Cortellini P, Nieri M, Prato GP, Tonetti MS. Single minimally invasive surgical technique with an enamel matrix derivative to treat multiple adjacent intrabony defects: Clinical outcomes and patient morbidity. J Clin Periodontol. 2008;35(7):605-613.
-
Harrel SK. Videoscope-assisted minimally invasive surgery (VMIS) for bone regeneration around teeth and implants: A literature review and technique update. Dent J (Basel). 2018;6(3):30. doi:10.3390/dj6030030
-
Nares S, ed. Advances in Periodontal Surgery: A Clinical Guide to Techniques and Interdisciplinary Approaches. Springer Nature; 2019:87-99.
-
Harrel SK, Nunn ME, Belling CM. Long-term results of a minimally invasive surgical approach for bone grafting. J Periodontol. 1999;70(12):1558-1563. doi:10.1902/jop.1999.70.12.1558
-
Harrel SK, Abraham CM, Rivera-Hidalgo F, Shulman JD, Nunn ME. Videoscope-assisted minimally invasive periodontal surgery (V-MIS). J Clin Periodontol. 2014;41(9):900-907.
-
Harrel SK, Abraham CM, Rivera-Hidalgo F, Shulman JD, Nunn ME. Videoscope-assisted minimally invasive periodontal surgery: One-year outcome and patient morbidity. Int J Periodontics Restorative Dent. 2016;36(3):363-371.
-
Harrel SK, Nunn ME, Abraham CM, Rivera-Hidalgo F, Shulman JD, Tunnell JC. Videoscope-assisted minimally invasive surgery (VMIS): 36-month results. J Periodontol. 2017;88(6):528-535.
-
Harrel SK, Valderrama P, Barnes JB, Blackwell EL. Frequency of root surface microgrooves associated with periodontal destruction. Int J Periodontics Restorative Dent. 2016;36(6):841-846.
-
Harrel SK, Wilson TG Jr, Tunnell JC, Stenberg WV. Laser identification of residual microislands of calculus and their removal with chelation. J Periodontol. 2020;91(12):1562-1568.
-
Dunegan KA, Deas DE, Powell CA, Ruparel NB, Kotsakis GA, Mealey BL. Subgingival scaling and root planing during minimally invasive periodontal surgery: A randomized controlled split-mouth trial. J Periodontol. 2024;95(1):9-16.
-
Wilson TG Jr. A new minimally invasive approach for treating peri-implantitis. Clin Adv Periodontics. 2019;9(2):59-63.
-
Al Shaikhly B, Harrel SK, Umorin M, Augsburger RA, Jalali P. Comparison of a dental operating microscope and high-resolution videoscope for endodontic procedures. J Endod. 2020;46(5):688-693.
-
Diaz P, Gonzalo E, Villagra LJG, Miegimolle B, Suarez MJ. What is the prevalence of peri-implantitis? A systematic review and meta-analysis. BMC Oral Health. 2022;22(1):449. doi:10.1186/s12903-022-02493-8
-
Kim S, Kratchman S, eds. Microsurgery in Endodontics. 1st ed. Wiley Blackwell; 2018:221-226.
-
Ryder MI, Armitage GC. Minimally invasive periodontal therapy for general practitioners. Periodontol 2000. 2016;71(1):7-9.
Figures
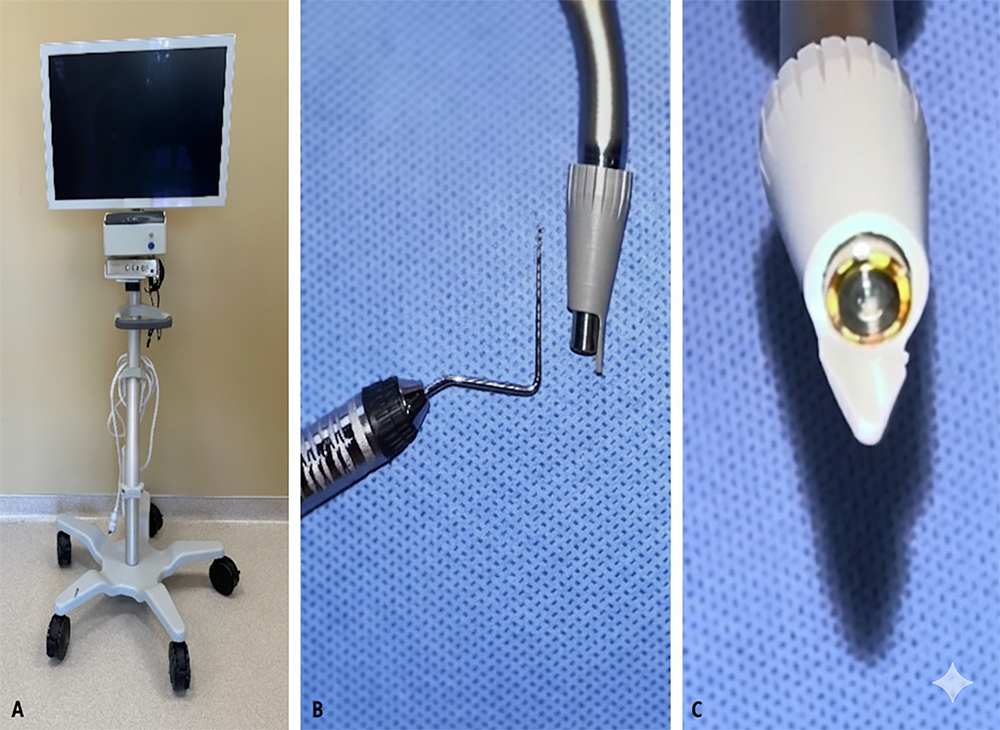
Figure 1. The images of A. Videoscope Device B. Videoscope camera tip C. Front view of videoscope camera tip
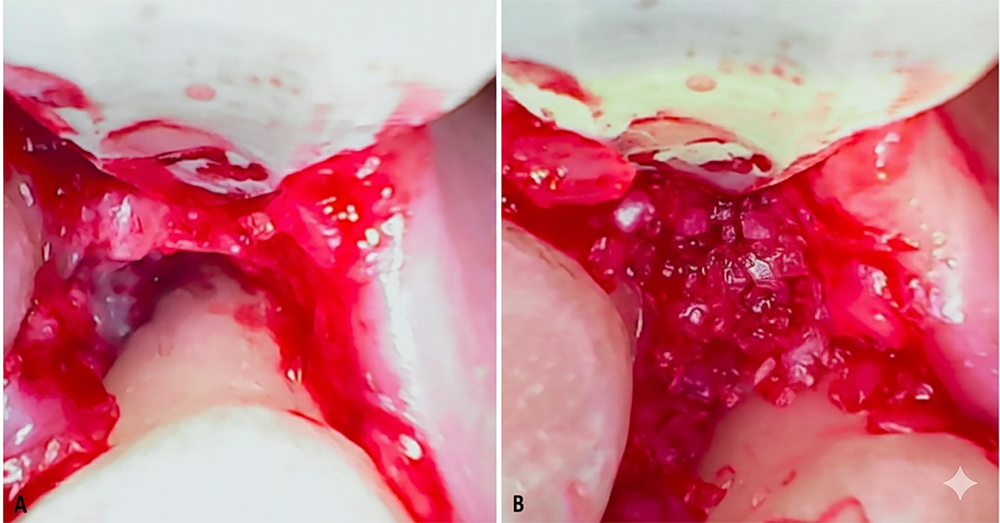
Figure 2. Videoscope images at periodontal regenerative surgery A. Three-wall periodontal defect view B. The image of periodontal defect filling with biomaterial
Tables
Table 1. Clinical Studies related to videoscope and videoscope-assisted minimal invasive surgery
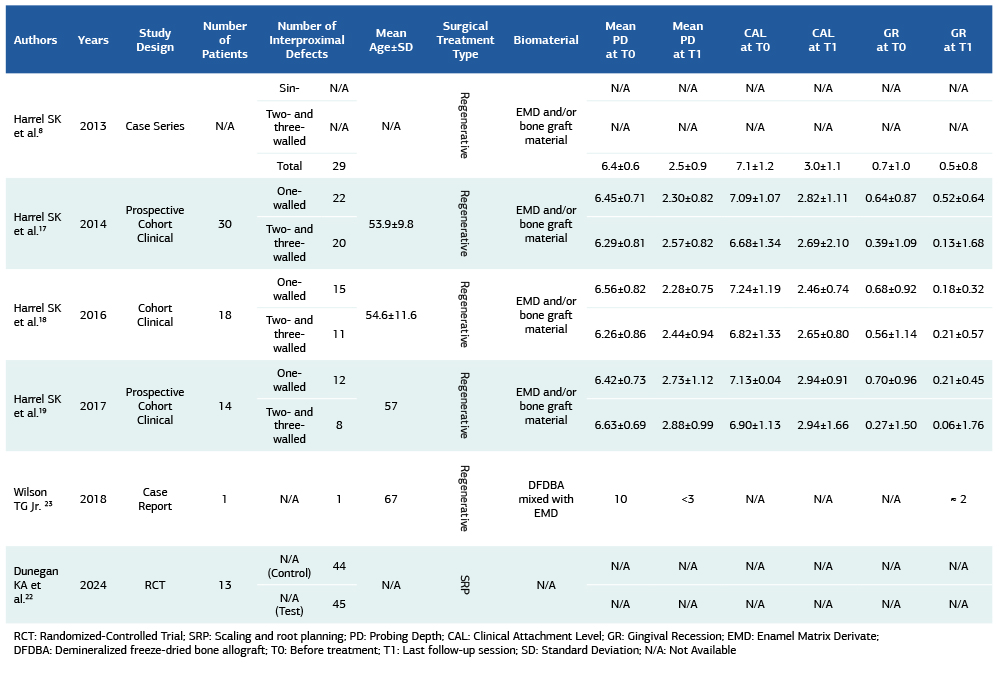
RCT: Randomized-Controlled Trial; SRP: Scaling and root planning; PD: Probing Depth; CAL: Clinical Attachment Level; GR: Gingival Recession; EMD: Enamel Matrix Derivate; DFDBA: Demineralized freeze-dried bone allograft; T0: Before treatment; T1: Last follow-up session; SD: Standard Deviation; N/A: Not Available
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Berceste Guler Ayyildiz, Halil Ayyildiz, Salvador Nares, Tolga Fikret Tozum. Videoscope visualization and videoscope-assisted minimally invasive surgery in dentistry: a narrative review. Ann Clin Anal Med 2026;17(Suppl 1):S93-98
- Received:
- January 20, 2025
- Accepted:
- March 3, 2025
- Published Online:
- March 13, 2025
- Printed:
- February 20, 2026