
Postoperative patient satisfaction and oncological outcomes of grisotti flapvs. total mastectomy: a retrospective analysis
Grisotti flap mastectomy: satisfaction and outcomes
Authors
Abstract
AimThis study aimed to compare Grissoti flap tecnique technique and total mastectomy regarding postoperative patient satisfaction, oncological outcomes, and recurrence rates in patients with centrally located breast tumors.
MethodsA retrospective analysis was conducted on 45 patients who underwent either the Grisotti flap technique (n = 15) or total mastectomy (n = 30) from August 2021 and January 2024. Demographic, clinicopathological, and prognostic data were analyzed, including tumor stage, surgical margins, recurrence rates, and BREAST-Q scores for breast satisfaction , psychosocial well-being, and sexual well-being.
ResultsPatients in the Grisotti group were younger (mean age 47.6 ± 11.4 vs. 57.2 ± 6.31 years, p=0.004) and had smaller tumors (median size 15 mm vs. 30 mm, p=0.006). Breast satisfaction (84 vs. 71, p<0.001), psychosocial well-being (80 vs. 70, p<0.001), and sexual well-being scores (81.5 vs. 66, p<0.001) were significantly higher in the Grisotti group. There were o significant differences were observed in local recurrence, axillary dissection, or re-excision rates between the two groups.
ConclusionThe Grisotti flap technique demonstrated superior patient satisfaction and psychosocial outcomes while maintaining oncological safety comparable to that of mastectomy. The Grisotti flap tecnique offers a viable alternative to mastectomy, particularly in patients prioritizing aesthetic outcomes. Future studies with larger cohorts are needed to confirm these findings.
Keywords
Introduction
Breast cancer is one of the most common types of cancer among women and remains a significant cause of morbidity and mortality worldwide.1,2 Modern breast cancer surgery aims not only to achieve effective tumor excision but also to optimize aesthetic and functional outcomes.3 In this context, oncoplastic surgical approaches play a critical role in ensuring both cancer control and aesthetic balance.4 Grisotti oncoplastic surgical technique was developed to provide aesthetic reshaping of defects resulting from the excision of tumors located near the nipple-areola complex.5 This method aims to preserve the anatomical and functional characteristics of the breast tissue while simultaneously ensuring optimal oncological outcomes.6
Mastecomy is a common procedure involving complete breast removal, often followed by reconstruction. It is preferred in cases where the tumor is extensive, breast-conserving surgery is not feasible, or the patient is at high risk.7,8,9 Both surgical methods yield different outcomes based on criteria such as postoperative patient satisfaction, adequacy of surgical resection margins, and long-term recurrence rates. However, studies directly comparing these parameters between Grisotti technique and mastectomy remain limited in the literature. This study aims to compare Grisotti oncoplastic surgical technique and mastectomy in terms of postoperative patient satisfaction, adequacy of oncological excision margins, and recurrence rates. The study seeks to elucidate the clinical efficacy and patient-centered outcomes of these two surgical approaches.
Materials and Methods
We retrospectively analyzed 106 patients treated for centrally located breast tumors at our clinic from August 2021 to January 2024 with either total mastectomy or the Grisotti flap technique. Demographic and clinical data, including gender, age, surgical method applied, and postoperative outcomes, were obtained from the institutional database.
A total of 45 patients were included in the study. The analysis comprised 15 patients who underwent Grisotti flap technique (Group 1) and 30 patients who underwent total mastectomy (Group 2). A comparison was made between the two groups (Figure 1).
The clinicopathological and prognostic data collected in the study included parameters such as age, tumor T and N stages, preferred surgical method, surgical resection status, margin positivity, and local recurrence. In accordance with our standard clinical procedures, the BREAST-Q questionnaire was administered to patients who had completed surgical operations and adjuvant therapy at least six months prior to the study, and informed consent was obtained from all participants. To ensure comprehension in Turkish, the original Swedish version of the questionnaire underwent a validated translation process. The BREAST-Q questionnaire is a patient-reported outcome measure designed to assess the impact of breast reconstruction surgeries on patient satisfaction. The modules used in this study were as follows:
1. Satisfaction with Breasts: A 16-item scale assessing satisfaction with breast shape, symmetry, sensation, and appearance.
2. Psychosocial Well-being: A 10-item scale evaluating selfconfidence in social settings and the extent to which individuals feel equal to or normal compared to other women.
3. Sexual Health: A 6-item scale addressing the impact of breast appearance and surgical intervention on sexual life. Responses from each scale were combined and converted into standardized scores ranging from 0 to 100, which were analyzed using the official scoring system of the BREAST-Q.10
The exclusion criteria for the study were as follows:
1. Missing clinicopathological or follow-up data
2. Presence of multicentric or multifocal breast cancer, inflammatory breast cancer, or distant metastases
3. Occurrence of minor complications (e.g., infection, hematoma, seroma)
4. Absence of centrally located breast tumors
5. Conditions contraindicating radiotherapy
6. History of undergoing symmetry surgery
7. Incomplete completion of the questionnaire or nonparticipation in the survey
8. Comorbidities (collagen collective tissue disease, rheumatoid arthritis, etc)
Ethical ApprovalThis study was approved by the Ethics Committee of the University of Health Sciences Antalya Training and Research Hospital (Date: 19.12.2024, Decision No: 20/30).
Statistical AnalysisStatistical analyses were performed using IBM SPSS Statistics for Windows, version 29.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range (IQR)), and categorical variables as number (percentage). Appropriate parametric or nonparametric tests were used for group comparisons. A two-sided p<0.05 was considered statistically significant.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
The study included 45 patients (median age: 52 years, range: 34-77). Of these, 15 (33.3%) underwent the Grisotti flap technique, and 30 (66.6%) underwent mastectomy. Regarding tumor stage, 5 patients (11.1%) were classified as stage 1A, 5 patients (11.1%) as stage 2A, 19 patients (42.2%) as stage 2B, 10 patients (22.2%) as stage 3A, 1 patient (2.2%) as stage 3B, and 5 patients (11.1%) as stage 3C. The mean follow-up duration was 19.7 ± 4.36 months, and the median body mass index (BMI) of the patients was 26.1 kg/m² (IQR: 22-35). The median BREAST-Q score for satisfaction with breast appearance was 74 (range: 40-90), for psychosocial wellbeing was 72 (range: 42-86), and for sexual well-being was 68 (range: 46-92) (Table 1). Differences in age, tumor size, and pathological subtypes between patients undergoing Grisotti technique and mastectomy were evaluated. The mean age of patients in the Grisotti group was 47.6 ± 11.4 years, whereas the mean age in the mastectomy group was 57.2 ± 6.31 years. This difference was statistically significant (p=0.004). The median pathological tumor size was 15 mm (IQR: 11-29) in Grisotti group and 30 mm (IQR: 25-48.8) in the mastectomy group, showing a significant difference (p=0.006). Regarding pathological subtypes, 86.7% of patients (13 individuals) in Grisotti group and 86.7% of patients (26 individuals) in the mastectomy group were classified as having ductal carcinoma, with no statistically significant difference in subtype distribution (p=0.223).
No significant differences were observed between the groups concerning axillary dissection, re-excision, or DCIS rates. However, the rate of DCIS was calculated as 66.7% in Grisotti group and 33.3% in the mastectomy group (p=0.056). These findings suggest that Grisotti technique and mastectomy may differ in terms of patient profiles and pathological characteristics (Table 2).
Significant differences were found in the BREAST-Q scores between patients in Grisotti and mastectomy groups. The median satisfaction score with breast appearance was 84 (IQR: 82–86) in Grisotti group and 71 (IQR: 68–74) in the mastectomy group, with this difference being statistically significant (p<0.001). In terms of psychosocial well-being, Grisotti group had a median score of 80 (IQR: 78–82.5), compared to 70 (IQR: 66.5–72) in the mastectomy group (p<0.001). Sexual well-being scores were also significantly higher in Grisotti group, with a median of 81.5 (IQR: 80–82.5) compared to 66 (IQR: 62–68) in the mastectomy group (p<0.001). These findings suggest that Grisotti technique yields better outcomes in terms of patient satisfaction and well-being compared to mastectomy (Table 3).
Discussion
The Grisotti flap technique is increasingly preferred for treating NAC involvement and centrally located breast tumors due to its ability to provide a wide resection area.Additionally, the preservation of breast shape using dermoglandular flaps allows this method to offer significant superiority in terms of aesthetic and functional outcomes.11,12 In our study, we demonstrated that Grisotti technique provides both oncologically safe and cosmetically satisfactory results in patients with NAC involvement or tumors located close to this region.
Traditionally, mastectomy was the first choice for centrally located breast cancers. However, the development of oncoplastic techniques and the widespread use of volumepreserving surgeries in recent years have led to a significant decline in the popularity of mastectomy.13 Studies have shown no significant differences in oncological outcomes between mastectomy and breast-conserving techniques.14 Similarly, research comparing mastectomy with oncoplastic techniques has reported no significant differences in oncological outcomes, strongly recommending oncoplastic techniques for both oncological and cosmetic advantages.15 In a multicenter study by Davies et al., similar findings were observed, and patients were encouraged to choose oncoplastic breast-conserving surgery over mastectomy.16
Various techniques are available for centrally located breast cancers, including methods like the melon slice and Grisotti flap techniques for tumors involving or close to the nippleareola complex.17,18 A study by Teh et al. examining the 5-year experience of Asian women undergoing Grisotti flap technique for centrally located breast cancers reported high cosmetic satisfaction.19 Similarly, other long-term studies on oncoplastic breast-conserving surgery have demonstrated excellent cosmetic outcomes with Grisotti flap technique.20,21 In their study on Grisotti flap technique applied to central breast cancers, Dabiri et al. emphasized its ease of application, high cosmetic satisfaction, and low complication rates, concluding that it is a viable option.22 Additionally, Kılıç et al. found that oncoplastic techniques combined with Grisotti flap are preferable to mastectomy in terms of both oncological and cosmetic outcomes for selected advanced-stage breast cancer cases.23
In our study, we compared the oncological outcomes and BREAST-Q satisfaction survey scores between patients who underwent Grisotti flap technique and those who had mastectomy for tumors involving or near the NAC. The average “Satisfaction with Breasts” score was 84% in Grisotti group, compared to 71% in the mastectomy group, where the unilateral loss of breast tissue was a factor. This difference was statistically significant. Similarly, the “Psychosocial Well-Being” score was 80% in Grisotti group and 70% in the mastectomy group, with Grisotti group showing a statistically significant advantage. The “Sexual Well-Being” score was also significantly higher in Grisotti group, which may be associated with reduced feelings of insecurity due to the preservation of breast tissue. In terms of oncological outcomes, no statistically significant differences were observed between the groups regarding re-excision and local recurrence rates. Adequate resection margins achieved in patients undergoing Grisotti flap technique contributed to favorable oncological results. Additionally, the mean age of patients in Grisotti group was significantly lower, which may be linked to the increased aesthetic concerns in younger patients.
Limitations
This study has several limitations. Firstly, its retrospective design inherently introduces potential biases and limits the ability to establish causal relationships. Additionally, the relatively small sample size and single-center design may restrict the generalizability of the findings. Another limitation is that only two surgical techniques—mastectomy and oncoplastic surgery with the Grisotti method—were compared, while other breast-conserving techniques were not included in the analysis. Furthermore, surgeries were performed by different surgical teams, which may have introduced variability in operative techniques and postoperative outcomes. The relatively short follow-up period may have also limited the ability to comprehensively assess long-term outcomes, such as recurrence rates and patient satisfaction. Finally, the reliance on subjective data for psychosocial and sexual health evaluations introduces potential bias, as these outcomes can be influenced by individual perceptions and cultural differences. These limitations should be considered when interpreting the results of this study.
Conclusion
Grisotti flap technique emerges as an effective option for treating NAC involvement or centrally located tumors, offering both oncological safety and aesthetic success. Our study demonstrates that this technique is significantly superior to mastectomy in terms of patient satisfaction, psychosocial well-being, and sexual health. The absence of differences in oncological outcomes between the two methods supports the preference for Grisotti flap technique in appropriate patient groups with aesthetic concerns. These findings may pave the way for future studies evaluating Grisotti flap technique in larger patient populations.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all participants.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Abbreviations
BREAST-Q: Breast-Q questionnaire
DCIS: Ductal carcinoma in situ
IQR: Interquartile range
NAC: Nipple-areola complex
References
-
Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249. doi:10.3322/caac.21660
-
Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. doi:10.3322/caac.21763
-
Riis M. Modern surgical treatment of breast cancer. Ann Intern Med. 2020;56:95. doi:10.1016/j.amsu.2020.09.021
-
Piper M, Peled AW, Sbitany H. Oncoplastic breast surgery: current strategies. Gland Surg. 2015;4(2):154-163. doi:10.3978/j.issn.2227-684x.2015.03.01
-
Cantürk NZ, Şimşek T, Gürdal SÖ. Oncoplastic breast-conserving surgery according to tumor location. Eur J Breast Health. 2021;17(3):220-233. doi:10.4274/ejbh.galenos.2021.2021-1-2
-
Johnson M, Cook L, Rapisarda FI, Betal D, Bonomi R. Oncoplastic breast surgery technique for retroareolar breast cancer: a technical modification of the Grisotti flap in patients with short nipple to inferior mammary crease distance. J Surg Case Rep. 2020;2020(9). doi:10.1093/jscr/rjaa285
-
Freeman MD, Gopman JM, Salzberg CA. The evolution of mastectomy surgical technique: from mutilation to medicine. Gland Surg. 2018;7(3):308-315. doi:10.21037/gs.2017.09.07
-
Munhoz AM, Montag E, Filassi JR, Gemperli R. Immediate nipple-areola-sparing mastectomy reconstruction: an update on oncological and reconstruction techniques. World J Clin Oncol. 2014;5(3):478-494. doi:10.5306/wjco.v5.i3.478
-
Baker JL, Dizon DS, Wenziger CM, et al. “Going flat” after mastectomy: patient-reported outcomes by online survey. Ann Surg Oncol. 2021;28(5):2493-2505. doi:10.1245/s10434-020-09448-9
-
Dahlbäck C, Ullmark JH, Rehn M, Ringberg A, Manjer J. Aesthetic result after breast-conserving therapy is associated with quality of life several years after treatment: Swedish women evaluated with BCCT.core and BREAST-Q. Breast Cancer Res Treat. 2017;164(3):679-687. doi:10.1007/s10549-017-4306-5
-
Clough KB, Ihrai T, Oden S, Kaufman G, Massey E, Nos C. Oncoplastic surgery for breast cancer based on tumour location and a quadrant-per-quadrant atlas. Br J Surg. 2012;99(10):1389-1395. doi:10.1002/bjs.8877
-
Fitzal F, Nehrer G, Hoch D, et al. An oncoplastic procedure for central and medio-cranial breast cancer. Eur J Surg Oncol. 2007;33(10):1158-1163. doi:10.1016/j.ejso.2007.04.004
-
Farouk O, Attia E, Roshdy S, et al. The outcome of oncoplastic techniques in defect reconstruction after resection of central breast tumors. World J Surg Oncol. 2015;13(1):285. doi:10.1186/s12957-015-0688-1
-
Wagner E, Schrenk P, Huemer GM, Sir A, Schreiner M, Wayand W. Central quadrantectomy with resection of the nipple-areola complex compared with mastectomy in patients with retroareolar breast cancer. Breast J. 2007;13(6):557-563. doi:10.1111/j.1524-4741.2007.00492.x
-
Hossino D, Silverstein MJ, Savalia N, Jayich M, Khan S. Extreme oncoplasty: oncologically safe when compared with mastectomy. Ann Surg Oncol. 2024;31(11):7284-7288. doi:10.1245/s10434-024-15791-y
-
Davies C, Johnson L, Conefrey C, et al. Clinical and patient-reported outcomes in women offered oncoplastic breast-conserving surgery as an alternative to mastectomy: ANTHEM multicentre prospective cohort study. Br J Surg. 2024;112(1).
-
Essa MS, Ahmad KS, Salama AMF, Zayed ME. Cosmetic and oncological outcome of different oncoplastic techniques in female patients with early central breast cancer. Int J Surg Open. 2021;32:100336. doi:10.1016/j.ijso.2021.100336
-
Moustafa A, Fakhr I. Outcome of different oncoplastic surgical techniques for centrally located breast cancer. J Egypt Natl Canc Inst. 2014;26(4):203-209. doi:10.1016/j.jnci.2014.10.003
-
Teh MS, Teoh LY, Jamaris S, Lai LL, See MH. Outcomes of Asian women treated with Grisotti flap reconstruction for centrally located breast cancers: 5-year single-institutional experience. Ann Plast Surg. 2021;87(2):132-135. doi:10.1097/sap.0000000000002631
-
Emiroglu M, Sert I, Karaali C, et al. The effectiveness of simultaneous oncoplastic breast surgery in patients with locally advanced breast cancer. Breast Cancer. 2016;23(3):463-470. doi:10.1007/s12282-015-0585-z
-
Sanchez AM, De Lauretis F, Bucaro A, et al. Long-term safety of level II oncoplastic surgery after neoadjuvant treatment for locally advanced breast cancer: a 20-year experience. J Clin Med. 2024;13(13). doi:10.3390/jcm13133665
-
Dabiri C, Hotton J, Wehbe K, et al. Assessment of the Grisotti oncoplastic procedure for the management of central breast tumors. Breast J. 2021;27(7):595-602. doi:10.1111/tbj.14256
-
Kilic B, Bademler S, Ilhan B, et al. Pushing the limits of breast-conserving surgery with extreme oncoplasty. Breast Care (Basel). 2023;18(5):366-373. doi:10.1159/000531533
Figures

Figure 1. Flow chart
Tables
Table 1. Demographic and Clincal Characteristics of the Patients
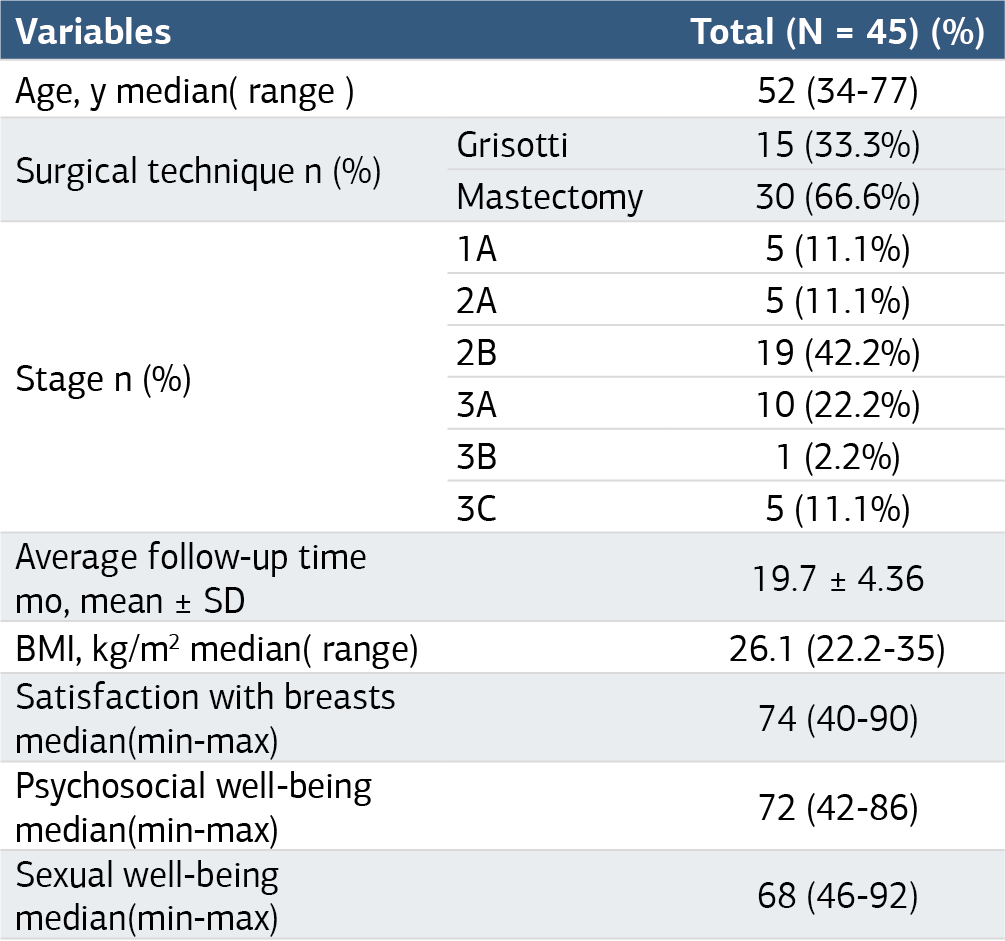
BMI: body mass index.
Table 2. Comparison of Demographic and Surgical Data Between Grissotti and Mastectomy Groups

DCIS: ductal carcinoma in situ.
Table 3. Comparison of BREAST-Q score data between Grisotti and mastectomy

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Halit Özgül, Ömer Çelik, Burak Şakar, Ali Çelik, Osman Zekai Öner. Postoperative patient satisfaction and oncological outcomes of grisotti flapvs. total mastectomy: a retrospective analysis. Ann Clin Anal Med 2025;16(3):227-231. doi:10.4328/ACAM.22578
- Received:
- January 22, 2025
- Accepted:
- February 23, 2025
- Published Online:
- February 28, 2025
- Printed:
- March 1, 2025