
Research of the effect of SSRI use on dental implant osseointegration: animal experiment in rabbit model
Effect of SSRI use on dental implant osseointegration
Authors
Abstract
Aim The aim of the study is to investigate the effect of SSRI use on titanium implant osseointegration in the rabbit model.
Methods Eight adult male New Zealand white rabbits were used in this study. 16 dental implants were inserted into each tibia of the rabbit’s leg. Rabbits were randomly divided into two groups: the drug group and the control group. After eight weeks, the groups were compared by resonance frequency analysis, immunohistochemistry, and histologically. In the immunohistochemical examination, Osteopontin (OPN) measurements during the osseointegration period of the implants were compared between the experimental group and the control group. Numbers of bone implant surface osteocytes, osteoclasts, and osteoblasts were observed between groups. In histological examination, sections were evaluated for bone formation, inflammation, fibrosis, and necrosis. The presence of each finding was given a value of 1, and its absence was given a value of 0. Immediately after the surgical procedure, and before the subjects were sacrificed at week 8. The osseointegration level of the implant was evaluated by the Resonance Frequency Analysis (RFA) method using the Ostell device. As a result of histological, immunohistochemical, and resonance frequency analysis examinations.
Results The number of osteocytes, osteoclasts, and osteoblasts in the Control group was numerically higher than in the Experimental group, and this difference was not found to be statistically significant. (p>0.05) Although the degree of fibrosis was lower in the control group, the difference between it and the experimental group was not found to be statistically significant. The Implant Stability Quotient (ISQ) values were taken daily with the Ostell device in the 8th week; The values of the Control group were higher than the values obtained from the experimental group, but the increase was not statistically significant. (p>0.05)
Conclusion Our study, which showed negative effects of SSR use on bone healing, although not statistically significant, revealed that the use of antidepressants should be taken into consideration in patients who will receive dental implants.
Keywords
Introduction
An implant is considered to be successfully osseointegrated due to the lack of movement at the connection between the implant and bone. Implant characteristics such as material type, surface topography, and chemical composition can greatly influence this process. Other factors, such as host physical quality or pharmacological agents, greatly contribute to the performance of this process.1,2
The function of SSRIs is to transport extracellular serotonin from synaptic gaps to presynaptic neurons. SSRIs have a high affinity for the serotonin transporter gene (5-HTT). It inhibits 5-HTT controls and prolongs the duration of serotonergic activity. This action will allow the presence of higher serotonin levels and strengthen signal transmission from presynaptic to postsynaptic neurons, thus treating depression. Although they are very effective in treating depression due to their high selectivity and potency for 5-HTT, which allows them to increase serotonin levels in the brain, SSRIs also increase systemic serotonin levels. High peripheral serotonin concentrations may affect other cells in the body, such as bone cells. Increasing evidence links SSRI use to decreased bone mineral density, increased risk of fractures, and dental implant failure.3
Although poorly understood, increasing evidence suggests that 5-hydroxytryptamine (5-HT) is an important factor in the regulation of bone quality and metabolism. 5-HT mediates its effects through membrane-bound receptors within the 5-HTR1 and 5-HTR2 family, some of which are found on all major bone cell types, including osteoblasts, osteoclasts, and osteocytes. In addition, direct serotonin synthesis by bone cells via tryptophan hydroxylase 1 (TPH1) has been documented.4,5 In this study, we aimed to investigate the effect of SSRI use on dental implant osseointegration based on various parameters.
Materials and Methods
Study Material and Design Ethics and AnimalsIn our study, 8 New Zealand (Oryctolagus cuniculus L) adult male rabbits, 6 months old and weighing an average of 2.5-3 kg, obtained from Dicle Unıversity Experimental Research Center, were used. During the study period, the experimental animals were placed in stainless steel cages of 50x80x50 cm, with a single rabbit in each cage. The feed and water needs of all animals are met indefinitely. The animals were given standard rabbit chow. Standard conditions were applied in the animal room (22-24 °C, 55-70% humidity, 1 atm, 12 hours light/dark room). Before surgery, all animals were placed in the laboratory and subjected to care and preliminary monitoring for one month to ensure optimal health conditions, protection from infection, and adaptation to their new place.
Study DesignThe 8 New Zealand (Oryctolagus cuniculus L) adult male rabbits were randomly divided into 2 groups of 8:1
1. Control group (group 1): The animals received a placebo solution after dental implant insertion until the day of sacrifice (n = 8).
2. SSRI group (group 2): The animals received an SSRI after dental implant insertion until the day of sacrifice (n = 8). All rabbits were sacrificed on week 8 after dental implant insertion by intraperitoneal administration of sodium pentobarbital 50 mg/kg (Pentothal; Abbott, Chicago, IL).
Surgical ProcedureAll surgical procedures were performed by a single operator using the blind technique. The legs were flexed, and the area was prepared with a sterile surgical drape. A skin, subcutaneous, and periosteal incision was made in the soft tissue on the proximal side of the corpus tibia, approximately 3 cm towards the distal condyle of the femur. With blunt dissection, soft tissue was excluded, and the medial surface of the tibia was exposed. Each implant cavity was prepared for the tibiae of each animal’s right and left legs. Implant cavities were prepared at 700 rpm, and the implants were inserted into the cavities with a maximum torque of 45 Ncm. 1st and 2nd groups; Dental implants with a diameter of 3.4 mm and a length of 8 mm were placed in the created slots by providing primary stability with the help of a ratchet. The operation was completed by suturing the periosteum, subcutaneous tissues, and skin with 3.0 polyglycolide-co-lactide absorbable sutures (Pegelak PGLA) and closing them primarily. Postoperatively, 50 mg/kg Ceftriaxone (CephaxonToprak) was given intramuscularly, and 4 mg/kg Carprofen (Rimadyl-Pfizer) was given subcutaneously in a 20 cc vial to the experimental animals for 3 days.
The subjects were taken to an 8-week rest period under suitable environmental conditions prepared in advance. While 4 mg/kg/day Lustral (Sertraline HCL) was administered to 4 rabbits in the first experimental group via gavage for 8 weeks, 4 rabbits in the control group were not given any medication and were monitored. No complications were observed in the animals until the time of sacrifice. At the end of the 8-week follow-up period, the rabbits were sacrificed using Sodium Pentothal under general anesthesia. All samples were collected using double-blind methodology.
Stability MeasurementsImmediately after the surgical procedure, and before the subjects were sacrificed at week 8. The osseointegration level of the implant was evaluated by the RFA method using the Ostell device. For RFA, the SmartPeg was placed on the implant with the Ostell Beacon device (Osstell AB, Göteborg, Sweden) in the direction recommended by the company and compressed (3-5 N). The tip of the device was approached to the SmartPeg at a 90° angle and a distance of 2-3 mm, and two measurements were made in the mesio-distal and bucco-lingual directions. (Figure 1) The measurements were repeated five times, and the most frequently repeated result was recorded. The arithmetic mean of the measurements was taken, and a single RFA score was recorded in ISQ for each implant.
Histological AnalysisTibia samples were fixed in 10% buffered formalin for 24 hours after the implants were removed. It was then decalcified with a slow decalcification solution (approximately 10% formic acid). The decalcification process lasted 4 days, and the tissue was checked every day. Tissues that were soft enough to be sectioned were subjected to routine tissue monitoring by making a macroscopic incision through the implant cavities. Then, paraffin blocks were prepared. 4 micrometer-thick sections were taken from each paraffin block for hematoxylin-eosin, rust, Masson trichrome, and immunohistochemical staining (Osteopontin (OPN/SPP1 Antibody (AKm2A1): sc-21742 200 µg/mL mouse monoclonal IgG1)). The sections were evaluated histomorphologically and histochemically in terms of bone formation, inflammation, fibrosis, and necrosis. The presence of each finding was given a value of 1, and its absence was given a value of 0.
During the examination, sections were obtained from all groups at the 8th week: Inflammation, Necrosis, and fibrosis.
Evaluation of these findings is based on the percentage of the area in Hematoksilen eozin boyama they cover in a high magnification field (×400); If it covers 0-5% of the area (0), If it covers 5-30% of the area (1), If it covers 30%-60% of the area (2), If it covers more than 60% of the area, it is scored as (3). Unfortunately, the facilities in our laboratory were not suitable for histomorphometric measurements. Therefore, assessment of bone implant contact could not be performed.
Immunohistochemical MethodDeparaffinization process: 4-micrometer-thick sections of tissues fixed with 10% buffered formaldehyde were taken on positively charged slides. The sections were kept in an oven at 70°C for 2 hours. The deparaffinization process was completed after being kept in 3 different xylenes and 3 different alcohols for 3 minutes each.
After deparaffinization, the sections were placed on the Ventana immunohistochemistry device. The osteopontin protocol was selected, and the device was operated semi-automatically with appropriate dab kits. When the device reached the antibody-dripping stage, 100 μL was withdrawn, and the antibody solution we had previously prepared was manually dropped directly onto the slide with a micropipette. (Osteopontin (OPN/ SPP1 Antibody (AKm2A1): sc-21742).
Antibody used (Osteopontin 200uq/ml mouse monoclonal IgG1) Osteopontin study protocol: Cell recovery 30 min, antibody incubation time 44 min.
Antibody preparation: Antibody dilution was made, delivered in concentrated form (1 µg/mL Osteopontin antibody + 200 µg/mL antibody solution).
Kit Used: (Ultrawiev Redkit) Total Run Time 4:30 Hours Osteopontin study protocol (cell conditioning 30 min, antibody incubation time 44 min).
Ethical ApprovalThis study was approved by the Ethics Committee of Dicle University, Experimental Animals were obtained (Date: 2022- 04-24, No: 8).
Statistical Analysis8 animals, 4 experimental and 4 control, were included in the study. Subject material was increased by using both tibiae of each rabbit. The compliance check of the numerical variables obtained from these animals with normal distribution was evaluated with the Shapiro-Wilk statistic. Summary statistics of the variables are given as mean and standard deviation. Categorical variables are summarized in numbers and percentages.
Pairwise group comparisons for numerical variables were evaluated with two independent group Student t tests. Variance homogeneity was checked with the Levene test. These variables are also summarized with error-bar graphs. Chi-square statistics were used to check the relationship between categorical variables. Statistical significance level was taken as p<0.05.
Reporting GuidelinesThis animal experimental study was reported in accordance with the ARRIVE (Animal Research: Reporting of In Vivo Experiments) guidelines.
Results
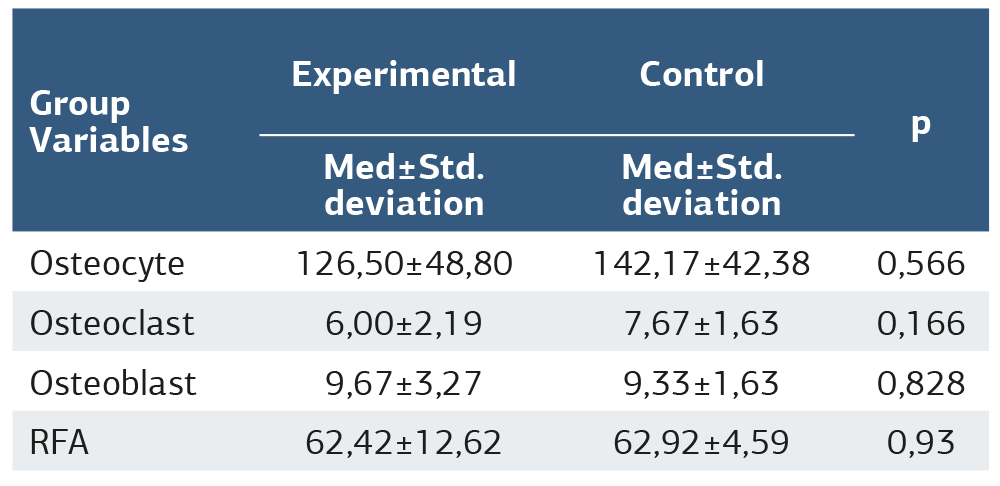
The number of osteocytes, osteoclasts, and osteoblasts in the Control group was numerically higher than in the Experimental group, and this difference was not found to be statistically significant. (Table 1)
No necrosis formation is observed during the experiment. Although the degree of fibrosis was lower in the control group, the difference between it and the experimental group was not found to be statistically significant. No difference was observed regarding the occurrence of inflammation depending on the use of SSRIs (Figure 2a, 2b, 2c, 2d).
Looking at the ISQ values taken daily with the Ostell device in the 8th week, the values obtained from the experimental and the Control group were higher than the values obtained from the experimental group, but the increase was not statistically significant (Table 1).
Discussion
Recent studies suggest that serotonin is an important regulator involved in the physiological control of bone mass, and such effects are thought to be linked to serotonergic signaling in bone. Considering the SSRI effect on peripheral serotonin concentrations, chronic use may seriously affect bone remodeling and quality and ultimately reduce the success of implanted biomaterials. Although dental implants have been very successful in establishing a solid connection with the host bone, implant failures continue to be evident in patients compromised by disease, old age, or chronic prescription use. The success of the implant depends not only on safe stabilization but also on the quality of the recipient bone surrounding the implanted material. Implant prognosis associates SSRI use with decreased bone mineral density, increased fracture risk, and dental implant failure compared to non-users.3 For this reason, we preferred the SSRI sertraline in our study.
Rabbits are often used to test dental implants and the biological and biomechanical aspects of osseointegration. In this context, extraoral bone regions offer a satisfactory amount of usable bone volume and a more comfortable surgical approach than the jaws. The anatomical dimensions of the rabbit tibia and femur allow the placement of implants with an average length of approximately 8-10 mm and an average diameter of 4 mm.6
Testing of dental implants in the tibia and femur allows a reasonable statistical comparison of the sample because the procedures are easily standardized and the anatomical and physiological conditions of the bony test sites are roughly equivalent. The number, size, and possible randomization of implants provide the necessary prerequisites for preliminary screening studies. However, the pattern in rabbit long bones exhibits some striking inherent biological and biomechanical limitations. Individual structural differences in tibial and femoral bone composition and the spatially expanded medullary cavity in the tibia limit the informative value of the latter results, since new bone formation originates primarily from the endosteum.7 Although the endochondral ossification process of the tibia bone differs from that of alveolar bone, we chose the rabbit model. The “ideal model” does not exist. No single animal, aside from humans, can perfectly exhibit human responses.8
The New Zealand White Rabbit is the most popular research breed. Furthermore, rabbits are phylogenetically closer to primates than rodents. They reach skeletal maturity between 20 and 30 weeks of age (females earlier).9 Adults display some Haversian remodeling, and their bone metabolism is somewhat Similar to humans. However, surgical castration is not enough to mimic satisfactory bone loss, and other techniques must be associated.10,11
In their retrospective review in 2014, Misch et al. showed that SSRI use caused failure between the first 4 and 18 months after implantation.12
In 2017, Chrcanovic and colleagues also compared implant failure rates between SSRI users and non-users. They identified 18 SSRI users with 48 implants and 282 controls with 883 implants (total, 300 patients and 931 implants) with at least 7 years of follow-up. They concluded that SSRI intake may not be associated with an increased risk of dental implant failure. In particular, Chrcanovic et al. and Wuetal studies reported different implant failure rates for case and control patients, but the difference between groups was reported by Chrcanovic et al. in their study (9.2% and 6.9%, respectively).12
More recently, Chrcanovic et al. (2017) reported in a retrospective study that SSRIs were associated with a 12.5% implant failure rate and 3.3% in non-users. They also stated that SSRI use was higher in older age groups and women. However, after adjusting for confounding variables in a multivariable model, no significant association was found between SSRI use and implant failure, and the authors concluded that SSRI intake did not influence implant failure. As noted in these two studies, implant surface characteristics, length, diameter, anatomical location, and smoking influence the risk of failure.12
In their study in 2021, Hakam and colleagues found that TCA users exhibited a significantly higher frequency of implant failure (33.3%) and had an approximately 12-fold higher risk of implant loss compared to non-antidepressant users (3.9%).13 Preclinical and clinical evidence suggests that antidepressant intake may compromise bone metabolism and interfere with implant osseointegration. As a result of this study, it was observed that the frequency of implant failure was significantly higher in those who used antidepressants (13.9%) than in those who did not use them (3.9%).9 The risk of implant failure in experimental animals using antidepressants was approximately 4.3 times higher than in animals not taking antidepressants. Pre-clinical and clinical evidence suggest that antidepressant intake may compromise bone metabolism and interfere with implant osseointegration.14
Several pre-clinical and clinical investigations have reported the detrimental impact of SNRIs on bone metabolism.15
This is in all clinical studies; Many confounding factors such as age, systemic conditions, medication use, oral hygiene, and smoking may affect the experimental results. In our study, other systemic and local conditions that would affect healing were excluded by providing standardization among the subjects (age, weight, gender, etc.). As a result, when bone healing markers were monitored in subjects administered SSRIs, although bone healing appeared worse in the experimental group, there was no statistical difference in osseointegration between the two groups. No difference was found.
Limitations
The bone structure, metabolism, and healing processes of animals differ from those of humans; therefore, the generalizability of the results to human subjects is limited. Additionally, osseointegration is a prolonged process, and short- term follow-ups may not provide comprehensive information regarding implant success.
Conclusion
In our study investigating the effect of SSRI use on osseointegration, we can state that although positive effects were observed in fibrosis, inflammation formation, necrosis formation, OPN expression, and biomechanical evaluation tests, which can be considered as early parameters of implant osseointegration, it was not statistically significant.
Declarations
Ethics Declarations
This study was conducted in accordance with internationally accepted principles for the care and use of laboratory animals. All procedures were performed following institutional and ethical standards, and efforts were made to minimize animal suffering and reduce the number of animals used. Ethical approval for the study was granted by the Ethics Committee of Dicle University (Date: April 24, 2022; Decision No: 8).
Animal and Human Rights Statement
All experimental procedures involving animals were conducted in accordance with institutional guidelines for the care and use of laboratory animals and approved by the Dicle University Animal Ethics Committee.
Informed Consent
Not applicable. This study was conducted using an animal experimental model and did not involve human participants.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
This investigation was supported by Dicle University Scientific Research Projects Coordination Office with project number Diş.22.008.
Author Contributions (CRediT Taxonomy)
Conceptualization: O.E., B.K.
Methodology: O.E., P.E.
Investigation: O.E., B.K., P.E.
Data curation: B.K., N.B.
Formal analysis: O.E., A.F.B.
Writing – original draft: O.E.
Writing – review & editing: B.K., P.E., A.F.B.
Supervision: O.E.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
5-HT: 5-Hydroxytryptamine
5-HTT: Serotonin Transporter
H&E: Hematoxylin and Eosin
ISQ: Implant Stability Quotient
OPN: Osteopontin
RFA: Resonance Frequency Analysis
SNRI: Serotonin–Norepinephrine Reuptake Inhibitor
SSRI: Selective Serotonin Reuptake Inhibitor
TCA: Tricyclic Antidepressant
References
-
Wu X, Al-Abedalla K, Rastikerdar E, et al. Selective Serotonin Reuptake Inhibitors and the Risk of Osseointegrated Implant Failure A Cohort Study. J Dent Res. 2014;93(11):1054-1061. doi:10.1177/0022034514549378
-
Guler R, Agacayak KS. The evaluation of the effect of long-term antihypertensive drug usage on bone density with dental volumetric tomography. J Clin Exp Dent. 2024;16(2):172–177. doi:10.4317/jced.61240
-
Hodge JM, Wang, Y, Berk M, et al. Selective serotonin reuptake inhibitors inhibit human osteoclast and osteoblast formation and function. Biol Psychiatry. 2013;74(1):32-39. doi:10.1016/j.biopsych.2012.11.003
-
Rizzoli R, Cooper C, Reginster JY, et al. Antidepressant medications and osteoporosis. Bone. 2012;51(3):606-613. doi:10.1016/j.bone.2012.05.018
-
Galli C, Macaluso G, Passeri G. Serotonin: a novel bone mass controller may have implications for alveolar bone. J Negat Results Biomed. 2013;12:12. doi: 10.1186/1477-5751-12-12
-
Oliveira NT, Guastaldi FP, Perrotti V. Biomedical TiMo alloys with surface machined and modified by laser beam: biomechanical, histological, and histometric analysis in rabbits. Clin Implant Dent Relat Res. 2013;15(3):427-437.
-
Slaets E, Naert I, Carmeliet G, Duyck J. Early cortical bone healing around loaded titanium implants: a histological study in the rabbit. Clin Oral Implants Res. 2009;20(2):126-134. doi:10.1111/j.1600-0501.2008.01623.x
-
Schindeler A, Mills RJ, Bobyn JD, Little DG. Preclinical models for orthopedic research and bone tissue engineering. J Orthop Res. 2018;36(3):832-840.
-
Naff, Katherine A, Suzanne C. “Chapter 6 - The Domestic Rabbit, Oryctolagus Cuniculus: Origins and History.” The Laboratory Rabbit, Guinea Pig, Hamster, and Other Rodents: Elsevier Inc; 2012, pp. 157–163
-
Pearce AI, Richards RG, Milz S, Schneider E, Pearce SG. Animal models for implant biomaterial research in bone: a review. Eur Cells Mater. 2007;2(13):1-10.
-
Castañeda S, Largo R, Calvo E, et al. Bone mineral measurements of subchondral and trabecular bone in healthy and osteoporotic rabbits. Skeletal Radiol. 2006;35(1):34-41. doi:10.1007/s00256-005-0022-z
-
Chrcanovic BR, Kisch J, Albrektsson T, Wennerberg A. Is the intake of selective serotonin reuptake inhibitors associated with an increased risk of dental implant failure?. Int J Oral Maxillofac Surg. 2017;46(6):782-788.
-
Hakam, AE, Vila, G, Duarte, PM. Effects of different antidepressant classes on dental implant failure: A retrospective clinical study. J Periodontol. 2021;92(2):196-204.
-
Yadav VK, Ryu JH, Suda N, et al. Lrp5 controls bone formation by inhibiting serotonin synthesis in the duodenum. Cell. 2008;135(5):825-837.
-
Shea ML, Garfield LD, Teitelbaum S, et al. Serotonin-norepinephrine reuptake inhibitor therapy in late-life depression is associated with increased marker of bone resorption. Osteoporos Int. 2013;24:1741-1749.
Figures

Figure 1. View of the smart peg in the implant cavity
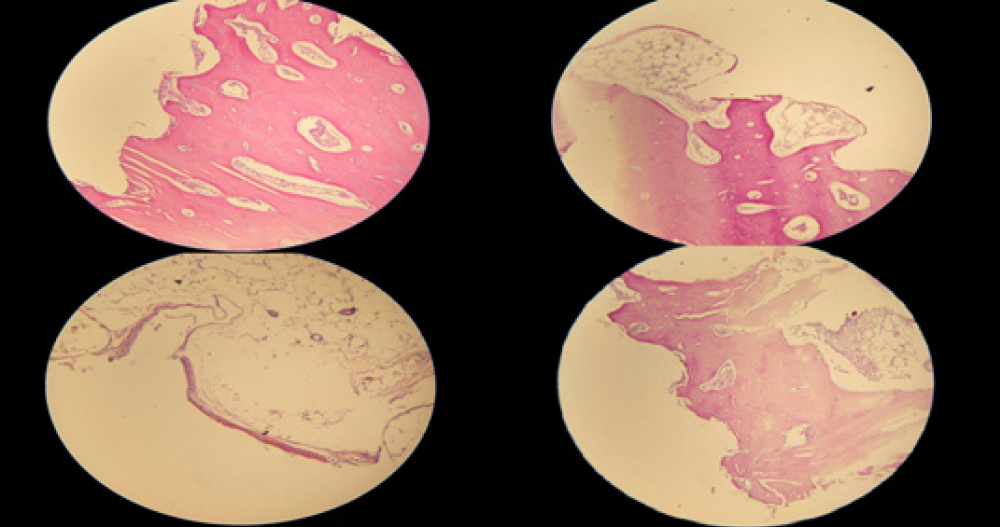
Figure 2. a: Bone-implant junction observed in the cortical bone in the experimental group, H&E, 40X, b: Lamellar bone remodeling on the bone-implant surface advancing towards the medullary area in the experimental group, H&E, 100X, c: Lamellar bone remodeling on the bone-implant surface advancing towards the medullary area in the experimental group, H&E, 200X, d: Bone marrow distance on the right side in the experimental group, bone remodeling in the implant threads on the left side, H&E, 100X (8th week)
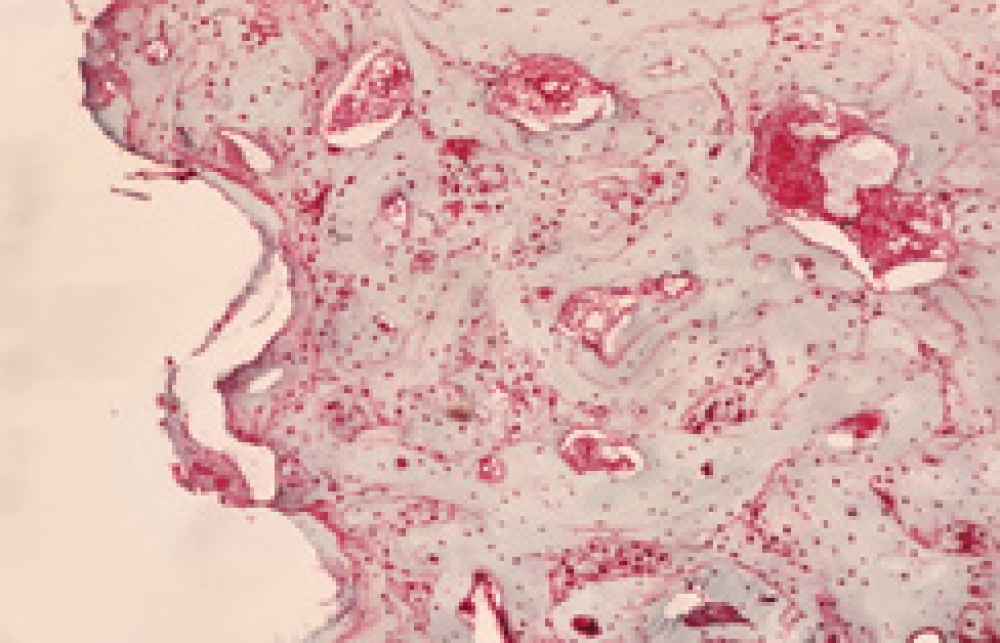
Figure 3. Cytoplasmic and nuclear granular staining was observed in osteoclasts, osteoblasts, and osteocytes. osteopontin, 200x
Tables
Table 1. Summary statistics for relevant variables are shown. Comparisons between the two groups were examined. According to the results obtained, there was no statistically significant difference between the experimental and control groups in terms of all variables (p>0.05)
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ozan Ergen, Beyza Kaya, Pınar Ergen, Nazan Baksi, Ahmet Ferhat Büyükdeniz. Research of the effect of SSRI use on dental implant osseointegration: Animal experiment in rabbit model. Ann Clin Anal Med 2026;17(Suppl 2):S104-108. doi: 10.4328/ACAM.22585
- Received:
- March 6, 2025
- Accepted:
- June 23, 2025
- Published Online:
- July 26, 2025
- Printed:
- March 20, 2026