
Valentino’s syndrome with two different clinical phenotypes in adolescents and adults: a case series
Valentino’s alive; duodenal perforation mimicking acute appendicitis
- Received:
- March 8, 2025
- Accepted:
- April 15, 2025
- Published Online:
- May 29, 2025
- Printed:
- October 1, 2025
Authors
Abstract
AimValentino’s Syndrome is a very rare condition and basically can be described as duodenal ulcer perforation mimicking the clinical findings of acute appendicitis. It is named after the actor Rudolph Valentino, who had undergone surgery for assumed acute appendicitis and turned out to have a perforated ulcer. The actor died in 1926 days after the surgery. We present a case series of adult and adolescent patients with Valentino’s Syndrome with two different clinical presentations.
MethodsMedical records of 6 patients who had Valentino’s Syndrome were retrospectively evaluated.
ResultsAll of the patients were males with a median age of 16,65 years (range: 13-27 years). Clinical and radiological findings suggested acute appendicitis in all of them. On surgical exploration, all had duodenal perforation with a grossly normal appearing appendix. Duodenal wall was intact in 3 (50%), suggesting recovered perforation, and all underwent appendectomy without an attempt for duodenal repair. The other 3 received duodenal repair for obvious perforation.
ConclusionAlthough Valentino’s is regarded as a myth by many, we present the most satisfactory and well-documented series. Differential diagnosis of patients with acute abdomen has become more prominent recently as the popularity of nonoperative management of acute appendicitis is increasing. Although rare, Valentino’s should be kept in mind in patients with unexpected operative findings or in patients with inconsistent clinical findings.
Keywords
Introduction
Acute appendicitis is one of the most common abdominal surgical emergencies in children and adults. Although it is assumed to be as old as human existence, its etiology remains contentious, and management has not become available until the last centuries due to a lack of anesthesia, a crucial ingredient for the existence of surgery 1,2. As the art of medicine evolves, the successful management of acute appendicitis has improved significantly such that studies advocating nonoperative management increased dramatically during the last 2 decades (3). However, the accurate diagnosis of acute appendicitis remains challenging, and many attempts have been made to create scoring systems to increase the accuracy of the diagnosis of acute appendicitis (Alvarado, Pediatric Appendicitis Score, AIRS, etc). Another issue is the lack of consensus about the definitive diagnosis of acute appendicitis. Although consensus dictates surgical exploration and histological evaluation, we think there is a shortage of data in the literature about the definitive diagnosis of acute appendicitis. Similarly, although the term ‘negative appendectomy’ is commonly used, there is no clear or agreed definition of the term. In uncomplicated cases, definitive diagnosis may remain unclear as the appendix is already a lymphoid tissue that accommodates inflammatory cells without the presence of acute appendicitis, and apparently, such specimens are diagnosed as lymphoid hyperplasia.
Valentino’s Syndrome is a very rare condition that describes the clinical condition characterized by duodenal ulcer perforation mimicking the clinical findings of acute appendicitis. It is named after the American actor Rudolph Valentino, who underwent surgery for assumed acute appendicitis but was found to have a perforated duodenal ulcer and deceased during the process after surgery. The proposed mechanism for Valentino’s Syndrome is that the leaked duodenal content travels through the right paracolic gutter, reaching to right lower quadrant and pelvis, causing the clinical picture mimicking acute appendicitis. Despite the advanced medical technology and widespread availability of medical services, the definitive diagnosis of acute appendicitis is still challenging, and Valentino’s Syndrome stands as a rare, mysterious condition that needs to be considered in the differential diagnosis while dealing with patients with abdominal pain for possible acute appendicitis. In this study, our aim is to present our case series of Valentino’s Syndrome in children and adults and describe a different clinical entity in adolescents, which we believe has not been reported before.
Materials and Methods
The patients who underwent surgery for suspected acute appendicitis but concluded to have Valentino’s syndrome between 2020 and 2024 are enrolled in the study. The cause of admittance, preoperative radiological and clinical findings, intraoperative surgical findings, and postoperative results were retrospectively evaluated. The patients without sufficient data are excluded from the study, and a total of 6 patients are enrolled.
Ethical Approval
This study was approved by the Ethics Committee of Ondokuz Mayıs University (Date: 2024-04-24, No: 2024-211).
Results
A total of 6 patients are enrolled in the study. All patients were males, and the median age of the patients was 16,65 years (range: 13-27 years ). All patients were admitted with abdominal pain lasting for no more than 4 days. Clinically, physical examination findings suggested acute appendicitis (tenderness/guarding/ rebound at the right lower quadrant) in all of the patients, and all underwent abdominal exploration for suspected acute appendicitis, but were finally concluded as Valentino’s Syndrome. In 1 patient with free air on plain X-ray examination (Figure 1), Valentino’s Syndrome was suspected before the operation and confirmed with laparoscopic exploration (Patient no:5). The duodenal perforation was possibly healed as no leak was observed after freeing the para-duodenal adhesions and air leak test was performed through the nasogastric tube. All patients had turbulent fluid in the pelvis and right paracolic gutter, but appendix vermiformis appeared as ‘innocent’ and was not perforated or inflamed enough to be the cause of turbulent fluid (Figure 2a-2d). Therefore, the attending surgeon urged to find the primary cause in all patients. Exploration of the whole abdomen was possible in 5 patients who underwent laparoscopic exploration but not in 1 patient who underwent open surgery. Periduodenal inflammation and omental adhesions were noticed in these patients (Figure 3a, 3b, 3c). When these adhesions were bluntly dissected, obvious duodenal perforation was visible in 2 patients (Figure 3d). The procedure was converted to open in these patients to repair the duodenal ulcer perforation. However, the adhesions on the duodenal wall were dense and dissection was challenging and regarded as hazardous in 3 patients, suggesting a chronic process and a possible healed perforation (Figure 3a and 3b). In the first case of these 3 patients, a simultaneous gastroscopy was performed during the operation, which demonstrated multiple duodenal ulcers, and integrity of the duodenal wall was confirmed (by air leak test and endoscopic vision). In the other 2 patients, a leak test was performed under laparoscopic vision by applying air through the NG tube. Appendectomy was performed in all these 3 patients due to the mystic nature of the condition, and the appendiceal lumen was found intact on histological examinations. No further action was performed, but all received medical treatment for duodenal ulcer until they had an elective gastroscopy. In 2 of these patients, intraperitoneal fluid was sampled intraoperatively for amylase and lipase levels with concomitant blood samples to compare with serum levels, and was found significantly higher. Intraperitoneal/serum amylase levels were 596/88 u/L and 150/59 U/L, lipase levels were 1551/29 U/L and 91/20 U/L. These findings are regarded as evidence of the duodenal origin of the intraperitoneal fluid. These 3 patients were subgroupped as Type B (occult, recovered, or healed duodenal perforation), and others were subgrouped as Type A (non-patent, disrupted duodenal wall).
Another patient (patient no=3) was consulted intraoperatively, who underwent a laparotomy through a right transverse lower quadrant incision for suspected appendicitis. An unexpected turbulent fluid in the right lower quadrant was found, which was not correlated with the gross appearance of the appendix vermiformis, exploration of the whole intestine was performed, but no cause was observed. For possible upper gastrointestinal perforation, methylene blue dye was given through the nasogastric tube and seen to spread into the peritoneal cavity. Another separate midline incision was performed, and a duodenal perforation was found and repaired.
All patients, except 2, denied any previous history of dyspeptic symptoms. All patients underwent plain X-ray examination in an erect position and ultrasonographic examination, but only 2 underwent computerized tomography (CT) with IV contrast before the operation. Suggestive findings of acute appendicitis on US examination were double wall thickness > 6mm (n = 4), increased mesenteric echogenicity at the right lower quadrant (n = 5), and right paracolic and/or pelvic fluid (n = 6). Suggestive findings of acute appendicitis on CT were double wall thickness > 6 mm (n = 1) and right paracolic and pelvic fluid (n = 1). In 1 patient (patient 5), free air under the diaphragm was noted in plain x-ray in the erect position (Figure 1), but no obvious open perforation was found when periduodenal inflamed tissues were dissected and regarded as Type b (Figure 3a and 3b). No free air was demonstrated in any of the plain X-rays or CT images except for this patient. All patients had physical examination findings suggestive of acute appendicitis (tenderness, guarding, and/or rebound localized to the right lower quadrant), and inflammatory markers were elevated in all (white blood cell count and C-reactive protein). Laparoscopic approach was performed in 5 patients but converted to open surgery in 2, at the discretion of the attending surgeon. One patient underwent open surgery but needed an additional separate open incision for repair of an open duodenal perforation. Intraoperative gastroscopy was performed in 1 patient to confirm the patency of the duodenal wall (patient 2). All patients underwent gastroscopy after the recovery period of the operation, and findings of bulbar duodenitis were present in all. Helicobacter pylori was confirmed histologically in 4 patients.
The patency of the other intraperitoneal organs (the whole intestine, gallbladder) was confirmed in all patients during the surgery to exclude and avoid overlooking any other co-existing.
Discussion
Although acute appendicitis is one of the most renowned and oldest surgical conditions of humans, it still remains a clinical challenge for both accurate diagnosis and differential diagnosis in adults and children 3,4. Actually, acute appendicitis is a final diagnosis that necessitates surgery and histological evaluation for confirmation of the diagnosis 5. Nevertheless, patients admitted with abdominal pain are individually challenging closed books in terms of differential diagnosis. There are many common conditions for differential diagnosis in patients with acute abdomen.
Historically, surgical correction of acute appendicitis was as challenging as diagnosis of the disease 1. With improvements in anesthesia and medical technology, surgery became a simple step in the management of acute appendicitis. Although diagnostic accuracy has also been improved in parallel with technological advancements, it still remains a significant challenge and prominent issue when dealing with patients with acute abdominal pain. Contemporarily, management principles evolved from conventional surgery to laparoscopic, endoscopic, and nonoperative management 6,7. Especially nonoperative management became prominent for the management of uncomplicated appendicitis during the last 2 decades 3.
The incidence of peptic ulcer disease appears to be increasing in children in recent years. Although not uncommon in adults, complications of peptic ulcer disease (bleeding and mainly perforation) are significantly rare in children 8,9. Commonly, peptic ulcer disease is classified among the causes of upper abdominal pain 8. Less commonly, patients may be admitted with chest or back pain. However, patients may be admitted with atypical clinical presentation with symptoms and clinical findings located in the right lower quadrant, which is not commonly mentioned in the textbooks.
Valentino’s Syndrome appears as a medical myth describing perforated peptic ulcer disease mimicking acute appendicitis due to gastric/duodenal content that travels through the right paracolic gutter and is usually diagnosed during the operation intended for acute appendicitis removal or even after the operation secondary to missing the condition 10,11,12. A PubMed search returned 17 publications containing around 30 cases of Valentino’s Syndrome. Interestingly, all were published after the year 2005, and there is not much information about who named the syndrome or who published it first. This scarce data deepens the mystery of Valentino’s Syndrome. It was reported in children, in the elderly, and even in pregnant patients 10,11,13. Most of the patients were males and rarely recognised before the operation 14,15,16.
Classically, a perforated ulcer can easily be identified on surgical exploration, and free air in radiological studies may be encountered in some cases 9. However, there was no intraperitoneal free air in 5 of our 6 cases, and no obvious/visible perforation was identified in 3 of our patients (Type B). In these 3 cases with no obvious perforation on surgical exploration, Valentino’s syndrome was concluded due to periduodenal inflammatory changes/adhesions, turbulent fluid in the right lower quadrant and pelvis with a normal appearing appendix, and/or increased levels of amylase and lipase in this turbulent fluid (Table 1). All 3 had undergone laparoscopic exploration for assumed acute appendicitis, enabling exploration of the whole intraperitoneal space. However, care should be taken that evaluation of the intraperitoneal space may not be enough, as some cases were also reported with retroperitoneal perforation without any intraperitoneal fluid accumulation, which constitutes a diagnostic pitfall and warrants caution 12,17,18. Surgical confirmation of healed Valentino’s (Type B, as we called it) was not reported before and contradicts the common belief that spontaneous healing of a perforated peptic ulcer would hardly be possible. However, there are many studies indicating peptic ulcer perforations heal without surgery, even in the era before antibiotics and anti-secretory agents 17,19,20. The most likely mechanism is that the adhesive behavior of the periduodenal structures or omentum would enable the spontaneous healing of the perforated ulcer after the intraperitoneal spilling of the chymus. Additionally, widespread prescription of antibiotics and gastric secretion inhibitors (omeprazole, etc) may change the usual course of the peptic ulcer disease process, and spontaneous healing may be accelerated.
In the modern era of nonoperative management of acute appendicitis, many questions and potential drawbacks emerge. Despite stunning developments in medical technology in the last century, proper diagnosis of acute appendicitis remains challenging. Although data about the definitive diagnosis of acute appendicitis is vague, the most common agreement is that it can be best achieved by surgical exploration and histological evaluation of the removed appendix, and the decision to operate or not remains challenging6. Accordingly, this new trend of nonoperative management constitutes a new challenge for surgeons to properly diagnose patients who are admitted with abdominal pain without performing surgery and obtaining a specimen for histological evaluation. Accurate clinical and radiological diagnosis is challenging in females, children, and elderly people 21,22. Also, as physicians commonly focus on obtaining a diagnosis, the possibility of false positive results of diagnostic tools appears to be underestimated and stands as a significant pitfall 23. These factors lead to unexpected scenarios during nonoperative or operative management of patients with acute abdomen. Therefore, in cases of inconsistent radiological and/or clinical findings, unexpected findings during surgery, and unsatisfactory improvement during the clinical follow-up when nonoperative management is preferred, other rare causes of acute abdomen should be considered, and patients should be re-evaluated. Laparoscopy is a reliable ally and tool for surgeons for evaluation of the whole peritoneal space, unless the surgeon notices something is ‘not right’ and has an extended list of ‘other causes’ of acute abdomen in mind.
Limitations
Limitations of our study are a small number of cases and a retrospective design. However, due to the rare nature of the condition, current literature has limited data with a limited number of case reports, and our study is the largest and most well-documented study.
Conclusion
Although stunning advances in medicine and medical technology provided improved diagnostic accuracy, many pitfalls remain during the evaluation of patients with ‘acute abdomen’. Acute appendicitis is a diagnosis mostly confirmed after surgery and histological evaluation; therefore, it is advised to identify the patients as ‘acute abdomen’ before the surgery to keep the clinician alert. Although significantly rare, Valentino’s syndrome (with obvious or occult perforation) is rare but should be considered amongst the differential diagnosis of patients with acute abdomen, and an intact duodenal or bulbar wall does not necessarily exclude it.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Ondokuz Mayıs University (Date: 2024-04-24, No: 2024-211)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
References
-
Williams GR. Presidential Address: a history of appendicitis. With anecdotes illustrating its importance. Ann Surg. 1983;197(5):495-506.
-
Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132(5):910-25.
-
Wagner M, Tubre DJ, Asensio JA. Evolution and current trends in the management of acute appendicitis. Surg Clin North Am. 2018;98(5):1005-23.
-
Gorter RR, Eker HH, Gorter-Stam MA, et al. Diagnosis and management of acute appendicitis. EAES consensus development conference 2015. Surg Endosc. 2016;30(11):4668-90.
-
Elfaedy O, Benkhadoura M, Elshaikhy A, Elgazwi K. Impact of routine histopathological examination of appendectomy specimens on patient management: a study of 4012 appendectomy specimens. Turk J Surg. 2019;35(3):196-201.
-
Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg: WJES. 2020;15(1):27.
-
Ullah S, Ali FS, Shi M, Zhang JY, Liu BR. Is it time for global adoption of endoscopic retrograde appendicitis therapy of acute appendicitis? Clin Res Hepatol Gastroenterol. 2022;46(10):102049.
-
Gryboski JD. Peptic ulcer disease in children. Med Clin North Am. 1991;75(4):889-902.
-
Hua MC, Kong MS, Lai MW, Luo CC. Perforated peptic ulcer in children: a 20- year experience. J Pediatr Gastroenterol Nutr. 2007;45(1):71-4.
-
Hussain K, Munir A, Wahla MS, Masood J. Valentino’s Syndrome: perforated peptic ulcer mimicking acute appendicitis managed through rutherford morrison incision. J Coll Physicians Surg Pak: JCPSP. 2016;26(8):727-8.
-
Jaboury IA. Valentino’s Syndrome: case report and review of literature. ANZ J Sur. 2020;90(5):940-1.
-
Rodrigo V, de Silva G, Jayasinghe D, Thalagaspitiya SPB, Srishankar S, Wickramarathne D. Valentino’s syndrome: a rare and lethal differential diagnosis for acute appendicitis. SAGE Open Med Case Rep. 2022;10(1):2050313x221132069.
-
Hsu CC, Liu YP, Lien WC, Lai TI, Wang HP. A pregnant woman presenting to the ED with Valentino’s Syndrome. Am J Emerg Med. 2005;23(2):217-8.
-
Mahajan PS, Abdulmajeed H, Aljafari A, Kolleri JJ, Dawdi SA, Mohammed H. A cautionary tale: unveiling Valentino’s Syndrome. Cureus. 2022;14(2):e22667.
-
Mahajan PS, Abdalla MF, Purayil NK. First report of preoperative imaging diagnosis of a surgically confirmed case of Valentino’s Syndrome. J Clin Imaging Sci. 2014;4(2):28.
-
Machaku D, Suleman M, Mduma E, Nkoronko M. Valentino’s Syndrome: a bizarre clinical presentation. J Surg Case Rep. 2023;2023(2):rjad035.
-
Wang HP, Su WC. Images in clinical medicine. Veiled right kidney sign in a patient with Valentino’s Syndrome—New Engl J Med. 2006;354(10):e9.
-
Okumura K, Suganuma T, Nakatani K, Okada S, Kubota T, Lefor AT. Duodenal fistula associated with a peri-appendiceal abscess: a case report. Int J Surg Case Rep. 2013;4(12):1104-6.
-
Taylor H. Perforated peptic ulcer; treated without operation. Lancet (London, England). 1946;2(6422):441-4.
-
Donovan AJ, Berne TV, Donovan JA. Perforated duodenal ulcer: an alternative therapeutic plan. Arch Surg (Chicago, Ill: 1960). 1998;133(11):1166-71.
-
Patel NB, Wenzke DR. Evaluating the patient with right lower quadrant pain. Radiol Clin North Am. 2015;53(6):1159-70.
-
Stephen AE, Segev DL, Ryan DP, et al. The diagnosis of acute appendicitis in a pediatric population: to CT or not to CT. J Pediatr Surg. 2003;38(3):367-71.
-
Šuta Kimle K, Chrz K, Ulrych J, E Šimůnková, D Michalský. Congruence of histological diagnosis with imaging and operation diagnosis in acute appendicitis. Rozhl Chir. 2019;98(11):457-61.
Figures
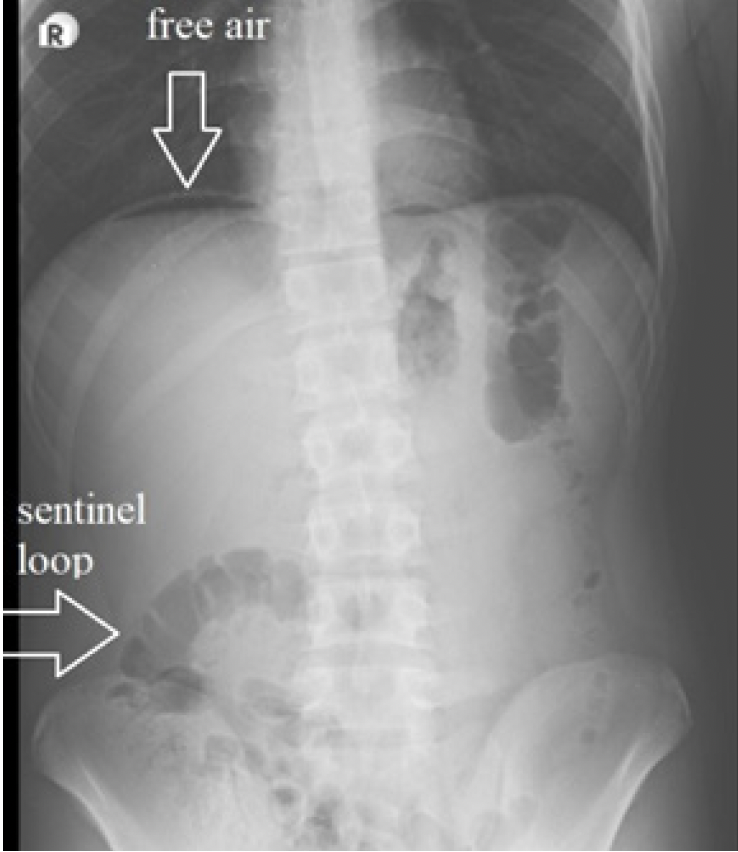
Figure 1. Subdiaphragmatic free air on the left side and sentinel loop in the right lower quadrant
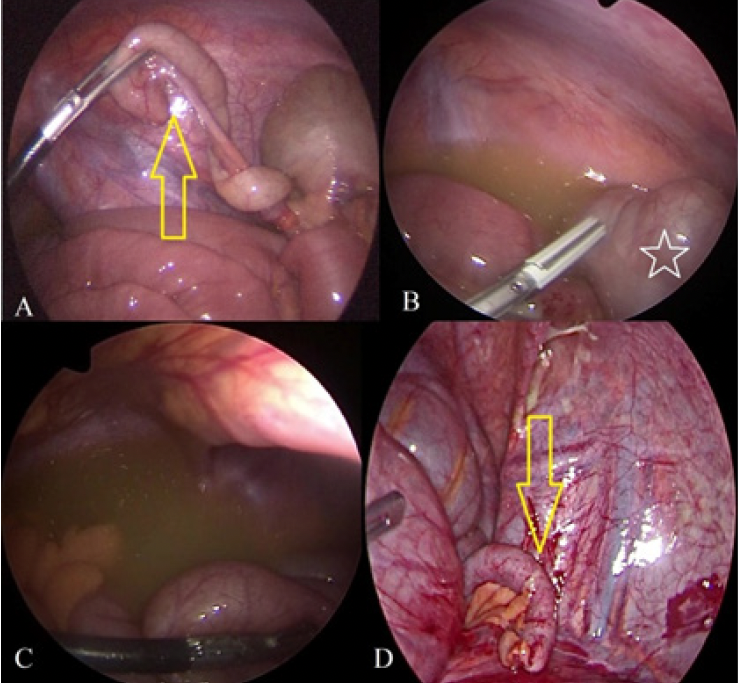
Figure 2. Intraoperative findings in patients with Type B Val- entino’s. Relatively normal appearing appendix (A and D, yellow arrow), pelvic and paracaecal turbulent fluid (b and c), caecum (White star sign)
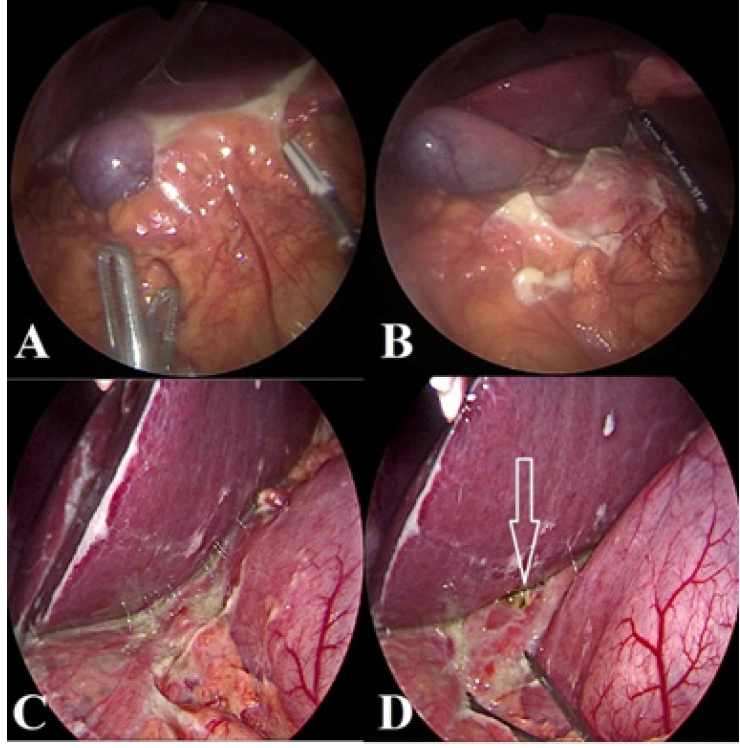
Figure 3. Paraduodenal adhesions and inflammatory changes in Type B (a) and Type A (c) Valentino’s Syndrome. After dissection of the adhesions, no opening was seen in Type B (b), but an obvious perforation in Type A (white arrow)(d)
Tables
Table 1. Details of radiological, clinical and laboratory findings of the patients

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Betul Keskinkılıç Yağız, Sertaç Hancıoğlu. Valentino’s Syndrome with two different clinical phenotypes in adolescents and adults; a case series. Ann Clin Anal Med 2025;16(10):710-714