
Illuminating inflammation in parkinson’s disease: an innovative approach to the relationship between serum calprotectin and C-reactive protein
Illuminating inflammation in parkinson’s disease
Authors
Abstract
Aim Parkinson’s disease (PD) is a disorder that affects 3.7% of people over the age of 65 and encompasses several neurodegenerative changes. Calprotectin is an inflammatory response-associated protein, while C-reactive protein (CRP) serves as a marker of inflammation. The aim of this study is to investigate the inflammatory aspect of PD by comparing serum calprotectin levels and CRP/albumin ratio (CAR) between patients and healthy subjects.
Methods This study was conducted on 78 participants, including PD patients and a healthy control group. Venous blood samples were taken for molecular analysis and the levels of serum calprotectin, CRP and albumin were assessed.
Results Serum levels of CRP and CAR were significantly higher in PD patients compared to controls, while albumin levels were low. However, there was no significant difference in serum calprotectin levels between the groups. Moderate to low linear relationships were observed between CRP and CAR with disease stage. The sensitivity of CAR in PD was found to be 44.7% with a specificity of 100%.
Conclusion The results of this study demonstrate that inflammatory markers (especially CRP and CAR) are elevated in PD and suggest their possible prognostic importance in the course of the disease. A negative association was found between albumin levels and disease duration, whereas no significant difference in serum calprotectin levels was found between PD patients and controls. Overall, the role of inflammation in PD and the prognostic value of calprotectin suggest the need for further research.
Keywords
Introduction
Parkinson’s disease (PD) is characterised by the misfolding of alpha-synuclein, followed by the formation and accumulation of intraneuronal amyloid, low-grade neuroinflammatory changes and selective neurodegeneration, and affects 3.7% of the population over the age of 65 1,2. Multiple factors contribute to the development of PD, resulting in heterogeneous clinical presentations and disease courses. PD is now considered a multisystem disease, affecting both the central and peripheral nervous systems (CNS, PNS) and causing both motor and non-motor symptoms. In addition to genetic predisposition, environmental triggers such as inflammation, abnormal protein aggregation, autophagolysosomal dysfunction and mitochondrial dysfunction contribute to neuronal degeneration 3,4.
Due to the early involvement of the gastrointestinal system in the pathophysiology, changes in the composition of the gut microbiota have been studied in relation to the pathophysiology of PD, often occurring years before the onset of motor symptoms. Communication between the gastrointestinal tract (GIT) and the CNS is bidirectional, and it is hypothesised that PD originates in the gut and spreads to the brain via the vagus nerve, targeting alpha-synuclein. The potential role of the gut microbiota in PD and other neurodegenerative diseases is supported by animal studies showing that the microbiota can influence α-synucleinopathy and neuroinflammation 1,4,5,6. Furthermore, gut inflammation and barrier dysfunction, along with gut microbiota products (which can induce “leaky gut” and/or local inflammation and potentially trigger or enhance amyloidogenesis), are considered potential key players in the aetiology of PD 4,7.
Calprotectin is a pleiotropic cytokine-like protein primarily involved in the accumulation of inflammatory cells; it also has bacteriostatic effects mediated by zinc-dependent enzymes 8. It represents approximately 60% of the cytosolic protein in neutrophils and is secreted as part of the inflammatory response. This protein, which is associated with inflammatory cytokine activity, can be found in serum, urine, saliva, cerebrospinal fluid, synovial fluid, amniotic fluid and faecal samples. As increased intestinal permeability is associated with increased calprotectin secretion, faecal calprotectin levels have been shown to be an indirect marker of intestinal permeability 9,10,11.
C-reactive protein (CRP) is a protein produced by the liver that serves as a marker of inflammation in the body. Both CRP and albumin are commonly used indicators of inflammation, defined as positive and negative acute-phase reactants, respectively 12. Based on numerous studies in the literature over the years, the CRP/albumin ratio (CAR) is considered a more valuable indicator of inflammation than either CRP or albumin alone 13. The aim of this study is to investigate the inflammatory aspect of PD by comparing serum calprotectin levels and CAR with healthy controls and to investigate their relationship with disease severity.
Materials and Methods
The research was designed as a cross-sectional study involving idiopathic PD patients and a control group between 17 December 2024 and 1 February 2025. Participants signed an informed consent form prior to enrolment.
Study ParticipantsInclusion criteria for patients were a diagnosis of PD according to the Movement Disorder Society (MDS) Clinical Diagnostic Criteria. The control group consisted of healthy adults. Exclusion criteria for patients included active infections, inflammatory, malignant or autoimmune diseases and treatment with antibiotics, non-steroidal anti-inflammatory drugs or proton pump inhibitors in the previous month. In addition, patients with organic brain damage, dementia according to MDS diagnostic criteria, and Hoehn and Yahr (H&Y) stage V, immobilized patients were excluded due to the difficulty of adequate clinical assessment. The exclusion criteria for the control group were the same as for the patients. Disease stage was assessed using the H&Y scale, and motor symptom severity was assessed using the Unified PD Rating Scale III (UPDRS III). Duration of PD (in years), levodopa equivalent daily dose (LEDD), H&Y stage and UPDRS III score were recorded.
Laboratory InvestigationsVenous blood samples were taken under outpatient conditions from all patients included in the study. EDTA tubes were used for complete blood count (CBC) and non-anticoagulated tubes for serum biochemistry. CBC samples were analysed immediately upon arrival at the biochemistry laboratory. For other tests, venous blood samples collected in non-anticoagulated tubes were centrifuged at 1500×g for 10 minutes after clotting. Serum CRP and albumin parameters were analysed. Samples were then aliquoted and stored at -80°C until further analysis. Calprotectin kits were stored at 2-8°C until the day of testing and brought to room temperature before use. Frozen serum samples were thawed, vortexed and centrifuged. Serum calprotectin levels were determined using the Elabscience Calprotectin kit (lot numbers: WX04000H2952 and WX09HB4V2777) by the sandwich enzyme-linked immunosorbent assay (ELISA) method according to the kit instructions. Measurements were made at 450 ± 10 nm using a microplate reader (BioTek Synergy HT). Calprotectin levels in serum samples were determined from the optical densities read against the calibration curve generated with the calibrators.
Ethical ApprovalThis study was approved by the Ethics Committee of Adana City Training and Research Hospital (Date: 2024-12-07, No: 241).
Statistical AnalysesData collected from patients in the study were analysed using IBM Statistical Package for the Social Sciences (SPSS) for macOSMacos 30.0 (IBM Corp., Armonk, NY). Frequency and percentage were used for categorical data, while mean, standard deviation, median, minimum and maximum were used as descriptive statistics for continuous data. Normality of variables was assessed using the Kolmogorov-Smirnov test. For group comparisons, the Mann-Whitney U test was used for two groups, and the chi-square test was used for comparisons of categorical variables. The relationship between continuous variables was examined using “Spearman’s Correlation Analysis.” Results were considered statistically significant when the p-value was less than 0.05.
Reporting GuidelinesThis observational cross-sectional study was reported in accordance with the STROBE reporting guidelines for observational studies.
Results
A total of 78 cases were analysed, including 48.7% (n=38) patients and 51.3% (n=40) controls. The mean age of the participants was 60 (35-81) years, 35.9% (n=28) were female and 64.1% (n=50) were male. In the patient group, disease duration was ≤4 years in 52.6% (n=20), 5-8 years in 28.9% (n=11) and >9 years in 18.4% (n=7), with a mean LEDD of 662.5 mg (100-1625) and H&Y stages <2 in 63.2% of patients and >3 in 36.8%. The UPDRS III score was 17 (range: 4-33).
The distribution of serum calprotectin, CRP, albumin and CAR levels in the patient and control groups was examined; statistically significant differences were found between the groups for CRP, albumin and CAR (p<0.001, p=0.046, p<0.001). CRP and CAR levels were found to be higher in PD patients compared to the control group, whereas albumin levels were lower in the PD group (Table 1).
No statistically significant difference was found in serum calprotectin levels between the patient and control groups. When examining the relationship of serum calprotectin, CRP, albumin and CAR with clinical variables in PD, no significant characteristics were found between serum calprotectin and H&Y, UPDRS III or LEDD scores. However, a moderate linear relationship was observed between CRP and H&Y, and a low linear relationship between UPDRS III and H&Y. In addition, a low-level negative association was found between albumin levels and disease duration (Table 2). The area under the curve for CAR in PD was found to be 79.6% with a cut-off value of 0.058. Consequently, CAR had a sensitivity of 44.7% and a specificity of 100% in PD (Table 3).
Discussion
In our study, CRP and CAR levels were found to be higher in PD than in healthy controls, whereas albumin levels were low. A moderate linear relationship was found between CAR and H&Y, and a low linear relationship was found between CAR and UPDRS III scores. A low-level negative association was found between albumin levels and disease duration. However, no statistically significant differences in serum calprotectin levels were found between PD patients and healthy controls.
The literature indicates that PD patients with high CAR levels have higher all-cause mortality, suggesting that overall survival in PD patients is related to the increase in CAR. The debate continues as to whether the use of nonsteroidal anti- inflammatory drugs (NSAIDs) can reduce the incidence and progression of PD; however, one study found no association between CAR levels and NSAIDs 14. In contrast, an analysis combining the results of several epidemiological studies by Gagne et al. suggested that the use of non-aspirin NSAIDs was associated with a 15% reduction in the risk of PD 15. In addition, another prospective study showed that users of ibuprofen had a lower risk of developing PD, which is consistent with previous findings and suggests that ibuprofen may have potential neuroprotective effects not shared by aspirin or other commonly used analgesics 16.
Recent clinical studies have shown that high CAR levels are associated with survival in other diseases and that CAR is a better prognostic marker than single inflammatory markers such as CRP 14,17,18. CAR is not simply an adjunct to CRP or albumin; research has shown that CAR can reflect dynamic changes in systemic inflammation and identify subtle differences between patients, suggesting a higher sensitivity for predicting inflammation 19,20.
Albumin is the most abundant plasma protein in the body and is a major component of cerebrospinal fluid. It has also been reported that serum albumin can disrupt the catalytic cycles that promote the self-assembly of α-synuclein and the remodelling of α-synuclein oligomers and high molecular weight fibrils into chimeric intermediates, potentially reducing toxicity and inhibiting interactions with N-terminal and central α-synuclein domains. Albumin levels have been proposed as an effective mortality marker in diseases characterised by neurodegeneration and inflammation, such as PD and Alzheimer’s disease 21.
Interestingly, while the CRP response increases in the acute phase, albumin decreases in both acute and chronic inflammatory conditions. This suggests that CAR may be advantageous in identifying both acute and chronic inflammation 14.
In the literature, calprotectin, which reflects intestinal inflammation and damage to the intestinal barrier, has been shown to be elevated in PD. One review suggested that early elevations in faecal calprotectin may indicate the development of gut dysbiosis and/or gut barrier damage that may occur decades before the onset of motor symptoms; therefore, faecal calprotectin may serve as a diagnostic and prognostic biomarker in PD 22. Calprotectin has been extensively studied as a faecal biomarker in PD, but it should be noted that results may be influenced by any condition that may alter intestinal permeability. For example, in our planned study, while integrating parameters such as serum calprotectin, CRP, albumin and CAR, we did not find statistically significant differences in serum calprotectin levels between PD and control groups, nor were any significant features identified in the relationships between serum calprotectin and H&Y, UPDRS III and LEDD levels 2,23,24.
The search for biomarkers in PD is important because it could facilitate accurate and early diagnosis of the disease, monitoring and the development of targeted treatment strategies. In our study, we identified high levels of CAR as an inflammatory marker in PD that correlates with disease severity.
Limitations
Our study has some limitations. One of them is that it was a single-center study with a small cohort of patients. In addition, commercial calprotectin assays have variable performance and there is currently a lack of assay standardization and universally accepted cut-off values.
Conclusion
In conclusion, our study showed that high CAR levels in PD serve as an inflammatory marker and correlate with disease severity. CAR may be a reliable prognostic biomarker for PD patients; however, it is suggested that its reliability could be improved by combining it with other molecules involved in inflammation.
Declarations
Ethics Declarations
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Adana City Training and Research Hospital (Date: 2024-12-07, No: 241). Participant confidentiality was maintained throughout the study.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: M.E., E.B.S.
Methodology: M.E., D.O.
Formal Analysis: M.E.
Investigation: M.E., E.B.S., D.O.
Data Curation: M.E.
Writing – Original Draft Preparation: M.E.
Writing – Review & Editing: E.B.S., D.O.
Supervision: E.B.S.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
AUC: Area Under the Curve
CAR: C-reactive Protein/Albumin Ratio
CBC: Complete Blood Count
CRP: C-reactive Protein
ELISA: Enzyme-Linked Immunosorbent Assay
H&Y: Hoehn and Yahr Scale
LEDD: Levodopa Equivalent Daily Dose
MDS: Movement Disorder Society
PD: Parkinson’s Disease
SPSS: Statistical Package for the Social Sciences
UPDRS III: Unified Parkinson’s Disease Rating Scale Part III
References
-
Sharma S, Awasthi A, Singh S. Altered gut microbiota and intestinal permeability in Parkinson’s disease: pathological highlight to management. Neurosci Lett. 2019;712:134516. doi:10.1016/j.neulet.2019.134516
-
Dumitrescu L, Marta D, Dănău A, et al. Serum and fecal markers of intestinal inflammation and intestinal barrier permeability are elevated in Parkinson’s disease. Front Neurosci. 2021;15:689723. doi:10.3389/fnins.2021.689723
-
Chen SJ, Lin CH. Gut microenvironmental changes as a potential trigger in Parkinson’s disease through the gut-brain axis. J Biomed Sci. 2022;29(1):54. doi:10.1186/s12929-022-00839-6
-
Romano S, Savva GM, Bedarf JR, Charles IG, Hildebrand F, Narbad A. Meta- analysis of the Parkinson’s disease gut microbiome suggests alterations linked to intestinal inflammation. NPJ Parkinsons Dis. 2021;7(1):27. doi:10.1038/s41531- 021-00156-z
-
Keshavarzian A, Engen P, Bonvegna S, Cilia R. The gut microbiome in Parkinson’s disease: a culprit or a bystander? Prog Brain Res. 2020;252:357-450. doi:10.1016/bs.pbr.2020.01.004
-
Sampson TR, Debelius JW, Thron T, et al. Gut microbiota regulate motor deficits and neuroinflammation in a model of Parkinson’s disease. Cell. 2016;167(6):1469-1480.e12. doi:10.1016/j.cell.2016.11.018
-
Rolli-Derkinderen M, Leclair-Visonneau L, Bourreille A, Coron E, Neunlist M, Derkinderen P. Is Parkinson’s disease a chronic low-grade inflammatory bowel disease? J Neurol. 2020;267(8):2207-2213. doi:10.1007/s00415-019-09321-0
-
Kowalski K, Mulak A. Brain-Gut-Microbiota axis in Alzheimer’s disease. J Neurogastroenterol Motil. 2019;25(1):48-60. doi:10.5056/jnm18087
-
Pathirana WGW, Chubb SP, Gillett MJ, Vasikaran SD. Faecal calprotectin. Clin Biochem Rev. 2018;39(3):77-90.
-
Lężyk-Ciemniak E, Tworkiewicz M, Wilczyńska D, Szaflarska-Popławska A, Krogulska A. Usefulness of testing for fecal calprotectin in pediatric gastroenterology clinical practice. Med Princ Pract. 2021;30(4):311-319. doi:10.1159/000512631
-
von Martels JZH, Bourgonje AR, Harmsen HJM, Faber KN, Dijkstra G. Assessing intestinal permeability in Crohn’s disease patients using orally administered 52Cr- EDTA. PLoS One. 2019;14(2):e0211973. doi:10.1371/journal.pone.0211973
-
de Liyis BG, Ardhaputra GYB, Liyis S, Wihandani DM, Siahaan YMT, Pinatih KJP. High C-Reactive Protein/ Albumin ratio predicts mortality and hemorrhage in stroke patients undergoing mechanical thrombectomy: a systematic review and meta-analysis. World Neurosurg. 2024;188:211-219.e1. doi:10.1016/j.wneu.2024.05.139
-
Kurniawan RB, Oktafia P, Saputra PBT, et al. The roles of C-reactive protein-albumin ratio as a novel prognostic biomarker in heart failure patients: a systematic review. Curr Probl Cardiol. 2024;49(5):102475. doi:10.1016/j.cpcardiol.2024.102475
-
Gao M, Zhang C, Gao L, Sun S, Song L, Liu S. Association between C-reactive protein-albumin ratio and overall survival in Parkinson’s disease using publicly available data: a retrospective cohort study. Heliyon. 2023;9(2):e12671. doi:10.1016/j.heliyon.2022.e12671
-
Gagne JJ, Power MC. Anti-inflammatory drugs and risk of Parkinson disease: a meta-analysis. Neurology. 2010;74(12):995-1002. doi:10.1212/ WNL.0b013e3181d5a4a3.
-
Gao X, Chen H, Schwarzschild MA, Ascherio A. Use of ibuprofen and risk of Parkinson disease. Neurology. 2011;76(10):863-869. doi:10.1212/ WNL.0b013e31820f2d79
-
Yu Y, Wu W, Dong Y, Li J. C-reactive protein-to-albumin ratio predicts sepsis and prognosis in patients with severe burn injury. Mediators Inflamm. 2021;2021:6621101. doi:10.1155/2021/6621101
-
Yuan J, Cheng Y, Han X, et al. Association between C-reactive protein/albumin ratio and all-cause mortality in patients with stroke: evidence from NHANES cohort study. Nutr Metab Cardiovasc Dis. 2024;34(10):2305-2314. doi:10.1016/j.numecd.2024.05.024
-
Liao CK, Yu YL, Lin YC, et al. Prognostic value of the C-reactive protein to albumin ratio in colorectal cancer: an updated systematic review and meta- analysis. World J Surg Oncol. 2021;19(1):139. doi:10.1186/s12957-021-02253-y
-
Sun P, Chen C, Xia Y, et al. The ratio of C-reactive protein/albumin is a novel inflammatory predictor of overall survival in cisplatin-based treated patients with metastatic nasopharyngeal carcinoma. Dis Markers. 2017;2017:6570808. doi:10.1155/2017/6570808
-
Sun S, Wen Y, Li Y. Serum albumin, cognitive function, motor impairment, and survival prognosis in Parkinson disease. Medicine (Baltimore). 2022;101(37):e30324. doi:10.1097/MD.0000000000030324
-
Al-Kuraishy HM, Al-Gareeb AI, Zaidalkiani AT, et al. Calprotectin in Parkinsonian disease: anticipation and dedication. Ageing Res Rev. 2024;93:102143. doi:10.1016/j.arr.2023.102143
-
Schwiertz A, Spiegel J, Dillmann U, et al. Fecal markers of intestinal inflammation and intestinal permeability are elevated in Parkinson’s disease. Parkinsonism Relat Disord. 2018;50:104-107. doi:10.1016/j.parkreldis.2018.02.022
-
Mulak A, Koszewicz M, Panek-Jeziorna M, Koziorowska-Gawron E, Budrewicz S. Fecal calprotectin as a marker of the gut immune system activation is elevated in Parkinson’s disease. Front Neurosci. 2019;13:992. doi:10.3389/ fnins.2019.00992
Tables
Table 1. Distribution of serum calprotectin, CRP, albumin and CAR in the patient and control groups
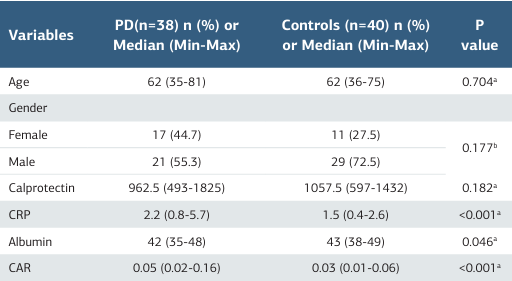
a Mann-Whitney U test b Chi-square test CRP: C- reactive protein, CAR: CRP/Albumin ratio
Table 2. Examination of the relationship between serum calprotectin, CRP, albumin, CAR and clinical variables in the patient group
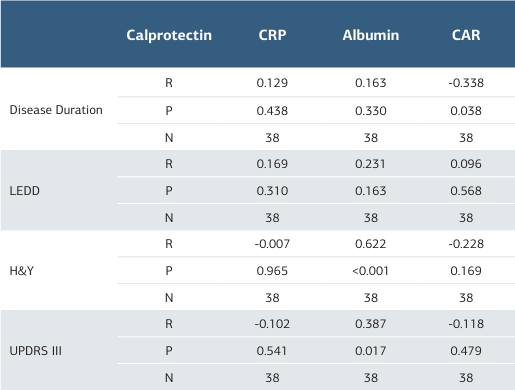
CAR: CRP/Albumin ratio, CRP:C-reactive protein, LEDD: Levodopa equivalent daily dose, H&Y: Hoehn&Yahr, UPDRS III: Unified Parkinson’s disease Rating Scale
Table 3. CAR ROC analysis

CAR: CRP/Albumin Ratio, AUC: Area Under Curve, PPV: Positive Predictive Value, NPV: Negative Predictive Value
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Miray Erdem, Elif Banu Soker, Derya Ozdogru. Illuminating inflammation in parkinson’s disease: an innovative approach to the relationship between serum calprotectin and C-reactive protein. Ann Clin Anal Med 2026;17(1):28-32
- Received:
- March 18, 2025
- Accepted:
- May 5, 2025
- Published Online:
- May 26, 2025
- Printed:
- January 1, 2026