
Comparison of maternal influence on children’s pain frequency, area, and coping behaviors according to pediatric age and gender
Pediatric pain and the relationship between parents
Authors
Abstract
Aim Pain is a complex and often overlooked issue in pediatric medical practice. Evaluating pain with the information received from the family is one of the most common mistakes made in clinical routine. By emphasizing the importance of the mother, we aim to offer a different perspective in understanding the evolution of the definition of pain.
Methods This cross-sectional study was conducted with children over eight years old admitted to the inpatient pediatric ward and their accompanying mothers. A total of 128 children were visited in the patient room with their parents. The questionnaires were completed in separate rooms, with one of the researchers reading and explaining each question.
Results The study included a total of 128 children, of whom 68 were girls (53.1%) and 60 were boys (46.9%), and their mothers. It was observed that as the frequency of pain in the mothers increased, the frequency of pain in the children also increased, and this was at a statistically significant level (p = 0.004). There was a statistically significant relationship between the mothers’ and children’s behavior of taking analgesics during pain (p = 0.006).
Conclusion The main implication of our findings was that mothers’ pain frequency, area of pain, and pain-related behaviors were likely to affect their children. Our study may help to prevent chronic pain that may develop in later life in vulnerable children by guiding interventions that focus on maternal pain management and behaviors early.
Keywords
Introduction
The International Association for the Study of Pain defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”.1 Although pain is seen in every society and age group, perceptions, expressions, and coping behaviors related to pain are extremely subjective. Pain perception varies from one person to another, depending on experiences, especially with the influence of age and culture.2 Pain is a difficult and often overlooked issue in pediatric medical practice. Evaluating pain with the information received from the family is one of the most common mistakes made in clinical routine. Children can describe the severity of pain after the age of five years, explain why and how they feel pain after the age of eight, and provide reliable information about the nature of pain after the age of 11.3 Children aged above eight can adequately and consistently express and communicate concepts related to pain and illnesses.4 Children are in constant communication with their environment starting at the moment they are born, and they acquire behaviors by observing their environment, especially from family members. Children create subjective pain experiences by processing all the data they have obtained and developing coping methods.5 Parents constitute the closest source of such data. The biopsychosocial model accepts that the interaction of biological, psychological, and social factors plays a role in the persistence and chronicity of pain.6,7 Pubertal onset is considered to be a period in which children may be particularly vulnerable to the development of chronic pain.8,9,10 Literature data suggest that chronic and recurrent pain most often increases in the pubertal period.11 Parental influences in the pre-adolescent period may provide a possible basis for the development of chronic pain in an individual, and understanding the importance of the family factor in pediatric pain can prevent it from developing into chronic pain in adulthood.12,13 The literature lacks evidence about children regarding the comparison of pain frequency between children and their parents. Therefore, we aimed to investigate the relationship between the mothers’ and children’s pain perceptions, areas, frequencies, and coping behaviors. Thus, we attempt to present a different perspective on understanding the evolution of experience in pain description, emphasizing the importance of the mother.
Materials and Methods
This cross-sectional study was conducted with children aged over eight years and their accompanying parents who were admitted to the general inpatient pediatric ward for one month beginning from February 2022. While creating the study protocol, it was assumed that there would be a similar number of pediatric patients during the data collection period, since 355 patients were hospitalized in the ward during this time period. A total of 128 children were targeted to be recruited voluntarily, with approximately half of the children between the ages of eight to 12 years and the other half between the ages of 13-18 years. All the participating parents in the study were mothers since all inpatients in the ward were accompanied by their mothers. Children aged over eight years, who had completed the expected mental development, without a chronic disease, and lived with their parents, were included in the study. A history of non-chronic pain in both the child and the accompanying parents was also questioned in the study. Each child was visited in the patient’s room with their parents present and informed about the study. Written consent was obtained from the parents, and verbal consent was obtained from the children. Questionnaires were completed in separate rooms, with each question being read and explained by one of the researchers, and responses were recorded without directing the children in any way.
Sociodemographic data were collected using a survey administered to the parents. In addition, the children and their parents were separately asked questions to obtain data on the frequency of pain, the area of pain, what they do when they experience pain, whether they exhibit social avoidance behavior in the presence of pain, the attitude of the family when they have pain, and how the child copes with this attitude. To determine social avoidance behavior, the mother was asked whether she avoided communication with family members and the social environment when she had pain, and the child was asked whether she wanted to stay in the school or play environment in the presence of pain. To evaluate the family’s attitude toward the child experiencing pain, the children were asked, “Do they ignore you?”, “Do they think you are not telling the truth?”, and “Do they do anything to relieve your pain?”. To determine how the mothers reacted when their children had pain, they were asked, “Do you intervene to relieve the pain experienced by your child?, “Do you ignore it?”, and “Do you think s/he is not telling the truth?”. The dependent variables of the study were children’s pain frequency, pain area, and pain-related behaviors. Independent variables were maternal pain frequency, maternal pain area, and maternal pain behaviors.
Ethical ApprovalThe study was approved by the ethics committee of Mersin University (Date: 2022-01-12, No: 15).
Statistical AnalysisDescriptive statistics for variables such as place of residence, gender, frequency of pain, and area of pain were expressed as numbers (n) and percentages (%). The comparison of categorical variables, such as maternal and child pain frequencies, was performed using the chi-square test. Differences in pain areas between groups were analyzed using the two-sample z-test. Statistical significance was defined as p < 0.05. All statistical analyses were performed using SPSS software (IBM Corp., Armonk, NY, USA).
Reporting GuidelinesThe study was reported in accordance with STROBE.
Results
The study included a total of 128 children, of whom 68 were girls (53.1%) and 60 were boys (46.9%), and their mothers. Table 1 presents the sociodemographic characteristics of the participants.
Maternal CharacteristicsThe characteristics of maternal pain are shown in Table 2.
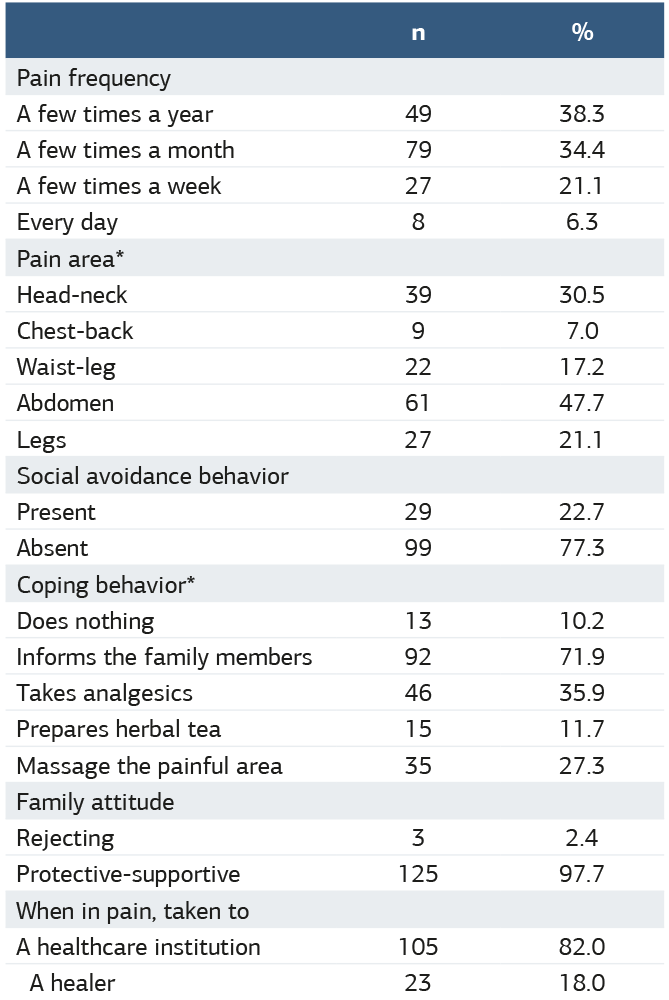
Multiple Options Could be Selected Children’s CharacteristicsOf the children participating in the study, 49.2% (n = 63) were aged eight to 12 years, and 50.8% (n = 65) were aged 13-18 years. Thirteen children (10.22%) were singletons, 21 (16.4%) had one sibling, 43 (33.6%) had two siblings, 31 (24.2%) had three siblings, and 20 (14.6%) had four or more siblings. While 114 children (89.1%) lived in a nuclear family, 14 children (10.9%) lived in an extended family. The children’s pain characteristics are presented in Table 3.
Multiple Options Could be SelectedIt was observed that as the frequency of pain in the mothers increased, the frequency of pain in the children also increased, and this was at a statistically significant level (p = 0.004). When the relationship between maternal and child pain frequency was evaluated according to age and gender, no statistically significant relationship was found (p > 0.05). The frequency of pain in children also did not significantly differ according to age or gender (p > 0.05).
While the frequency of mother-child pain was similar in those with a mother’s education of secondary school or below, the frequency of mother-child pain was found to be statistically different in those with a mother’s education of high school or above (p < 0.05).
When the pain areas were evaluated, the children of mothers with pain in the head and neck also had a significantly higher rate of pain in the same area (p < 0.001). However, there was no significant difference between the girls and boys concerning the frequency of head and neck pain in the mother or the child (p > 0.05). The analysis performed according to pediatric age groups revealed that the frequencies of head and neck pain in both the mother and the child were significantly higher for the children aged 13-18 years (p < 0.05).
The children of the mothers with waist-leg pain also had a significantly higher incidence of waist-leg pain (p < 0.05). However, no significant difference was found when the rate of waist-leg pain in the children was evaluated according to age or gender (p > 0.05). Abdominal pain was also found to be significantly higher among the children whose mothers also had abdominal pain (p < 0.05). When this was analyzed according to gender and age, no significant difference was found (p > 0.05). In addition, there was no statistically significant relationship between the maternal and child’s incidence of chest-back pain, shoulder-arm pain, or leg pain (p > 0.05).
A statistically significant relationship was observed between the massage behavior of the children whose mothers also exhibited this behavior when in pain (p < 0.001). When this behavior was evaluated according to gender and age, no statistically significant difference was detected (p > 0.05). There was a statistically significant relationship between the mothers’ and children’s behavior of taking analgesics during pain (p = 0.006). When this behavior was evaluated according to age and gender, no statistically significant difference was found (p > 0.05). However, the rate of children who took analgesics significantly differed between the pediatric age groups (p < 0.05). Children in the 13-18 age group used more analgesics.
Also, a significant relationship was observed between the mothers’ and children’s behaviors of preparing herbal tea at home when in pain (p < 0.001). When this was compared between the gender and age groups, no statistically significant difference was found (p > 0.05). There was a statistically significant relationship between the mothers’ and children’s social avoidance behavior in the presence of pain (p = 0.001). However, no difference was found when this behavior was evaluated according to gender or age (p > 0.05). Only 13 of the children (18%) stated that they were taken to a healer rather than a doctor when they had pain, and 12 (17.2%) of the mothers stated that they referred to a healer instead of a doctor.
Discussion
In this study, we compared pain frequency, areas, and behaviors between 128 children and their mothers, where we detected a statistically significant relationship. In the literature, studies on pain in children have mostly examined the sensory aspect of pain experience based on the measurement of pain levels. While investigating the parent-child relationship regarding pain, we evaluated the influence of psychosocial factors, such as pain frequency, pain area, and coping behaviors, rather than intensity of pain. We also investigated the potential role of gender differences in parental influence on children’s pain behaviors, and finally, it was determined that the frequency of pain in the children increased as the frequency of pain of their mothers increased. To the best of our knowledge, there is no study in the literature on the comparison of pain frequency between children and their parents. Parent-child pain relationship studies are often based on the observation of reactions to painful stimuli. In a study by Tsao et al., in which 133 children and mothers participated, a relationship was found between maternal pain tolerance and child pain tolerance.13 In a similar study, when 15 children with juvenile idiopathic arthritis, 25 healthy children, and their parents were examined in terms of pain tolerance, parental and children’s pain tolerance were correlated only in the healthy children group.14 In a study conducted in the Netherlands with children aged 12- 18 years, the most common area of pain was found to be the limbs (34%), followed by the head (26%), abdomen (16%), and back (15%).15 In the current study, abdominal pain was most commonly detected (32%), followed by head-neck pain (18.8%) and leg pain (14.8%) among 128 children. The different rates reported may be related to the differences in the ages of the samples. In our study, abdominal pain was significantly more common among the children of mothers who also had abdominal pain. We found similar results for head and neck pain, which was the second most common type of pain among children. It was observed that the incidence of head and neck pain increased among the children of mothers with head and neck pain, and this frequency increased for both the children aged 13-18 years and their mothers. We also detected a correlation between the mothers’ and children’s waist-leg back frequency. In a study, gender was found not to affect the relationship between child and mother pain.13 In the literature, some studies have reported findings indicating gender differences in parent-child pain relationships.16,17 Some studies have shown that girls have a stronger relationship with their parents’ laboratory pain responses than boys.18,19,20,21 In our study, there was no relationship with gender regarding pain area, frequency, and behaviors of children. The behaviors of the mothers and children during pain were significantly similar. It was found that the children whose mothers massaged the painful area also exhibited an increased frequency of massaging behavior when in pain. The frequency of preparing herbal tea at home to relieve pain was similarly higher among the children whose mothers also did this. The social avoidance behavior of the children was also found to be significantly related to their mothers’ social avoidance behavior in the presence of pain. Studies are showing that the expression of pain and pain-related behaviors vary depending on various factors, including age, culture, gender, socioeconomic status, number of siblings, education of parents, and experience.1,22,23 Therefore, in the environment where pain experience is shaped, parents constitute the most important source of data on children’s pain behaviors. The relationship between parents’ responses to their children’s pain and functional outcomes may be more complex than previously thought. Negligent and hostile behaviors of parents in adolescents have been associated with the continuation of pain into adulthood.24 In our study, 97.7% (n = 125) of the children stated that their families behaved protectively and supportively when they were in pain, while 2.3% (n = 3) pointed to a rejecting attitude. In addition, 3/4 of the children informed their family members when in pain, which can be considered a positive finding. In our study, when the children had pain, 72% informed the family, 36% took painkillers, and 27% massaged the painful area. There was an evident similarity between the analgesic intake and massage behaviors of the children and those of their mothers. Eighty-two percent of the children and 82.8% of the mothers considered that they should refer to a healthcare institution rather than a healer when in pain. Pain in children and adolescents is not only related to an impaired quality of life but also increases the risk of developing chronic pain syndrome in adulthood.12 Our findings can help prevent chronic pain that may develop at later ages in vulnerable children by guiding interventions that focus on the pain management and behaviors of their mothers in the early period.
Limitations
Current findings may not be generalizable to all children with pain, and additional studies with a larger sample are required. In addition, in our study, the data obtained from only the mother may be considered a limitation. Fathers were not included in the study because none of them accompanied their children to the hospital. However, our results can serve as a guide for future studies that will better reveal the parental influence on the risk of chronic pain development and reduced quality of life in children.
Conclusion
The main clinical implication of our findings is that mothers’ pain frequency, pain area, and behaviors when in pain were likely to affect those of their children. In this process, children whose cognitive abilities are still developing may be influenced by others’ observable pain frequency, area, and behaviors, as well as unobservable internal experiences, such as anxiety, which all shape their own subjective pain experiences.
Declarations
Ethics Declarations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and its subsequent amendments. All procedures involving human participants were performed in compliance with institutional and national research committee standards.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from the parents of all participating children, and verbal assent was obtained from the children prior to participation.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: A.T., G.T.
Methodology: A.T., G.T.
Investigation: A.T., C.Y.
Data curation: A.T., C.Y.
Formal analysis: A.T.
Writing – original draft: A.T.
Writing – review & editing: G.T., C.Y.
Supervision: G.T.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
IASP: International Association for the Study of Pain
SPSS: Statistical Package for the Social Sciences
STROBE: Strengthening the Reporting of Observational Studies in Epidemiology
References
-
Loeser JD, Treede RD. The Kyoto Protocol of IASP basic pain terminology. Pain. 2008;137(3):473-477. doi: 10.1016/j.pain.2008.04.025
-
Perquin CW, Hazebroek-Kampschreur AAJM, Hunfeld JAM, et al. Pain in children and adolescents: a common experience. Pain. 87(2000):51-58. doi: 10.1016/S0304-3959(00)00269-4
-
Piaget J. Cognitive Development in children: Piaget’s development and learning. J Res in Sci Teaching. 1964;2:176-186.
-
Bakır E. Çocuklarda Ağrı Değerlendirme ve Ölçekleri: Kültür ve Yaşın Ağrı Değerlendirmesine Etkileri [Pain Assessment and Scales in Children: Effects of Culture and Age on Pain Assessment]. Turkiye Klinikleri J Nurs Sci. 2017;9(4):299-314. doi: 10.5336/nurses.2016-52467
-
Palermo TM, Valrie CR, Karlson CW. Family and parent influences on pediatric chronic pain: a developmental perspective. Am Psychol. 2014;69(2):142-152.
-
Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol Bull. 2007;133(4):581-624.
-
Hirsch C, Hoffmann J, Turp JC. Are temporomandibular disorder symptoms and diagnoses associated with pubertal development in adolescents? An epidemiological study. J Orofac Orthop. 2012;73(1):6-18.
-
Janssens KA, Rosmalen JG, Ormel J, et al. Pubertal status predicts back pain, overtiredness, and dizziness in American and Dutch adolescents. Pain. 2011;128(3):553-559.
-
Leresche L, Mancl LA, Drangsholt MT, Saunders K, Von Korff M. Relationship of pain and symptoms to pubertal development in adolescents. Pain. 2005;118(1- 2):201-209.
-
King S, Chambers CT, Huguet A, et al. The epidemiology of chronic pain in children and adolescents revisited: a systematic review. Pain. 2011;152(12):2729- 2738.
-
Fearon P, HotopfM. Relation between headache in childhood and physical and psychiatric symptoms in adulthood: national birth cohort study. Br Med J. 2001;322(7295):1145.
-
Brattberg G. The incidence of back pain and headache among Swedish school children. Qual Life Res. 1994;3(Suppl 1):S27-31.
-
Tsao CJ, Li N, Parker D, Seidman LC, Zeltzer LK. Pubertal status moderates the association between mother and child laboratory pain tolerance. Pain Res Manag. 2014;19(1):23-29.
-
Thastum M, Zachariae R, Scholer M, Herlin T. Cold pressor pain: Comparing responses of juvenile arthritis patients and their parents. Scand J Rheumatol. 1997;26(4):272-279.
-
Hunfeld JA, Perquin CW, Duivenvoorden HJ, et al. Chronic pain and its impact on quality of life in adolescents and their families. J Pediatr Psychol. 2001;26(3):145-153.
-
Moon EC, Chambers CT, McGrath PJ. ‘’ He says, she says’’: a comparison of fathers’ and mothers’ verbal behavior during child cold pressor pain. J Pain. 2011;12(11):1174-1181.
-
Moon EC, Chambers CT, Larochette AC, Hayton K, Craig KD, McGrath PJ. Sex differences in parent and child pain ratings during an experimental child pain task. Pain Res Manag. 2008;13(3):225-230.
-
Chambers CT, Craig KD, Bennett SM. The impact of maternal behavior on children’s pain experiences: an experimental analysis. J Pediatr Psychol. 2002;27(3):293-301.
-
Walker LS, Williams SE, Smith CA, Garber J, Van Slyke DA, Lipani TA. Parent attention versus distraction: impact on symptom complaints by children with and without chronic functional abdominal pain. Pain. 2006;122(1-2):43-52.
-
Tsao JC, Lu Q, Myers CD, Kim SC, Turk N, Zeltzer LK. Parent and child anxiety sensitivity: relationship to children’s experimental pain responsibility. J Pain. 2006;7(5):319-326.
-
Evans S, Tsao JC, Lu Q, et al. Sex differences in the relationship between maternal negative life events and children’s laboratory pain responsibility. J Dev Behav Pediatr. 2009;30(4):279-288.
-
Neuman B, Fawcett J. The Neuman Systems Model. 5th ed. Columbus, OH: Prentice Hall; 2010. p.428.
-
Milani B, Magrini N, Gray A, Wiffen P, Scholten W. WHO calls for targeted research on the pharmacological treatment of persisting pain in children with medical illnesses. Evid. Based Child Health. 2011;6(3):1017-1020.
-
Wickrama KA, Conger RD, Wallace LE, Elder GH Jr. Linking early social risk to impaired physical health during the transition to adulthood. J HealthSoc Behav. 2003;44(1):61-74.
Tables
Table 1. Sociodemographic characteristics of the participants
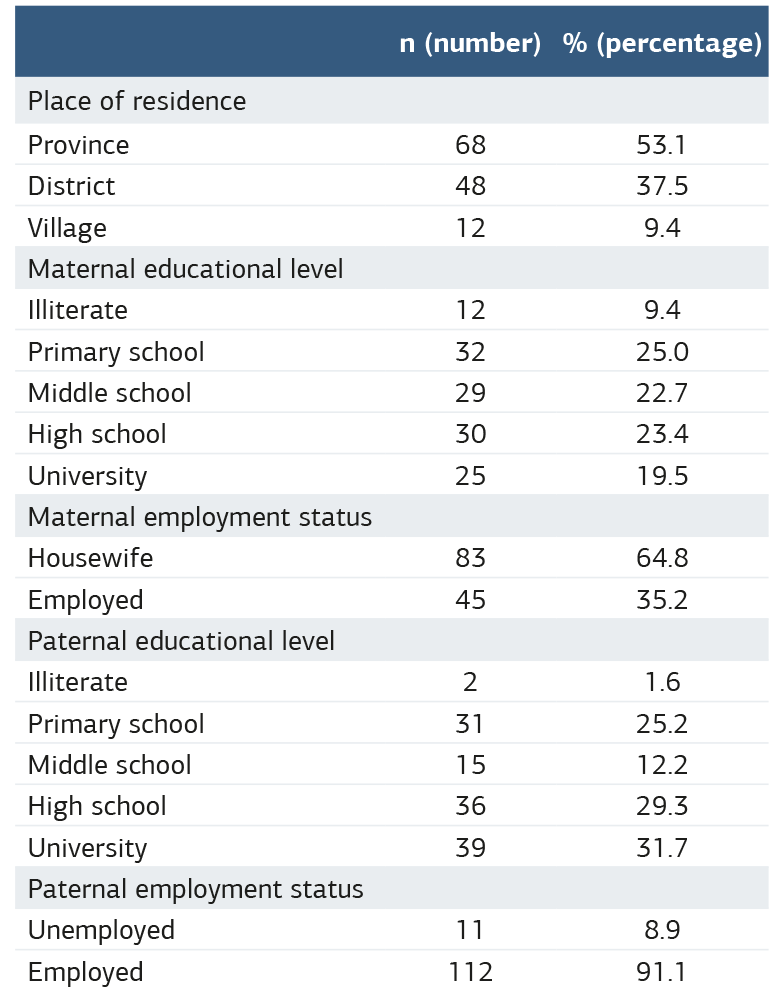
Table 2. Pain characteristics of the mothers included in the study
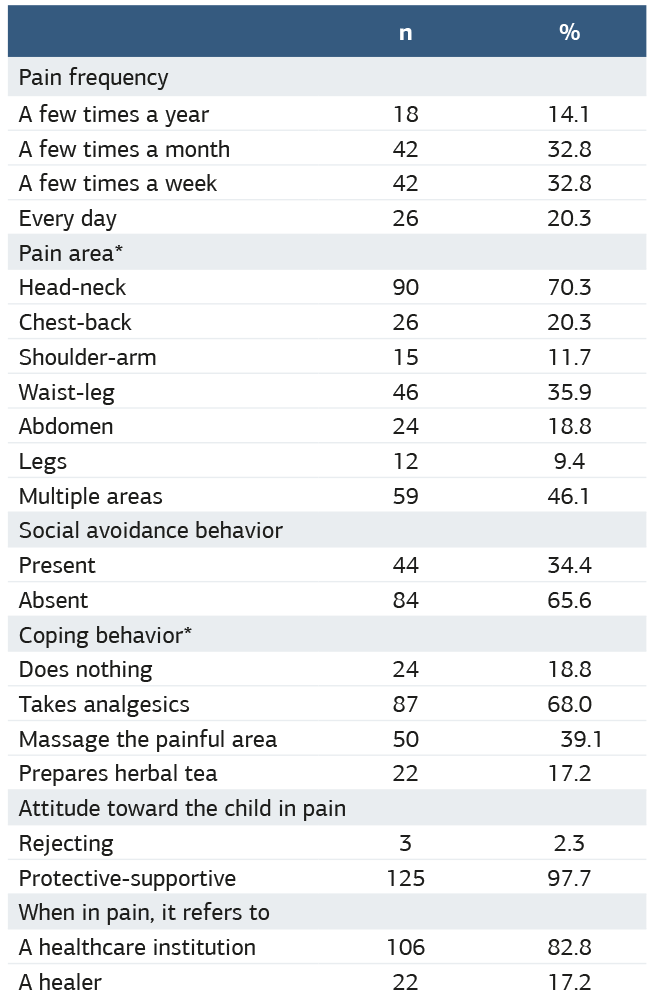
Table 3. Pain characteristics of the children included in the study
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ali Tunç, Güldane Turhan, Çiğdem Yalçın. Comparison of maternal influence on children’s pain frequency, area, and coping behaviors according to pediatric age and gender. Ann Clin Anal Med 2026;17(Suppl 2):S114-118. doi: 10.4328/ACAM.22666
- Received:
- March 22, 2025
- Accepted:
- May 12, 2025
- Published Online:
- June 11, 2025
- Printed:
- March 20, 2026