
Loss of cervical lordosis and association of fibromyalgia syndrome
Cervical lordosis in fibromyalgia
Authors
Abstract
Aim The causes of chronic and widespread pain in fibromyalgia (FMS) have not been elucidated yet. Previous reports determined that posture control changed, muscle strength decreased, body posture was misaligned (maladaptive posture), and functional capacity decreased in FMS patients. The aim of this study was to investigate the relationship between loss of cervical lordosis, pain, quality of life (QOL), and neck disability in patients with FMS.
Methods A total of 107 FMS (88 females and 20 males; age range of age: 18-65) were included in the study. Patients were divided into two groups according to the angle of cervical lordosis measured by the Cobb method, group 1 with a Cobb angle of ≤10°, and group 2 with an angle greater than >10°. Visual Analog Scale (VAS), QOL (36-Item Short Form Survey (SF-36)), and Neck Disability Index (NDI) were used to assess pain, overall quality of life, and functional disability, respectively.
Results The scores of VAS and NDI were significantly higher in group 1 than in group 2, indicating worse pain, impaired functional disability, and QOL in FMS patients with loss of cervical lordosis. All SF-36 subgroups but energy/fatigue, scores were also lower in group 1 than in group 2, indicating more impairment in patients with loss of cervical lordosis.
Conclusion Our results indicated that loss of cervical lordosis adversely affected the widespread pain, neck disability, and healthy related QOL in patients with FMS.
Keywords
Introduction
Fibromyalgia syndrome (FMS) is a chronic pain condition characterized by widespread pain all over the body and the presence of tender points at specific anatomic areas in, and its etiology is still unknown. This chronic pain may also be accompanied by reduced pain threshold, morning stiffness, sleep disorders, congenital disorders, fatigue, and psychological problems.1,2
Studies assert that neuroendocrine, autonomic, and immunologic mechanisms play a role in FMS and that some stressors such as insufficient nutrition, stress factors, changes in sleep routine, and poor body posture cause disease development in genetically predisposed individuals.3,4
A physiological curvature of the cervical spine is called cervical lordosis. Loss of cervical lordosis can occur in various conditions such as neuromuscular disease, congenital deformities, infection, tumor, trauma, and rheumatic disease. Although the mechanism of loss of cervical lordosis is not exactly known, some triggering factors have been reported.5 The loss of cervical lordosis is associated with a variety of musculoskeletal health problems, including neck pain, headaches, temporomandibular joint dysfunction, and poor quality of life.6,7
In previous studies comparing patients with fibromyalgia and healthy controls, it was observed that postural control changed, muscle strength decreased, body posture misaligned (maladaptive posture), and functional capacity decreased in FMS patients. Moreover, posture and gait deteriorate commonly due to pain and physical inactivity, and a vicious circle occurs.8,9,10
It is predicted in the literature that the loss of physiological lordosis may be a cause of pain depending on muscle imbalance. It has been emphasized in some recent studies that excessive stimulation of neurons at spinal and supraspinal levels has an important role in the formation and maintenance of widespread pain in FMS, and a relationship between pain and posture has previously been put forward.11
The intensity of widespread pain, QOL, and body posture in patients with fibromyalgia have previously been investigated in different studies in comparison with patients having rheumatic diseases or healthy controls.12,13,14 However, the impact of loss of cervical lordosis on FMS has not been assessed. The aim of this study was to investigate the relationship between loss of cervical lordosis, pain, quality of life (QOL), and neck disability in patients with FMS.
Materials and Methods
This cross-sectional study was conducted with FMS patients who were recruited from the outpatient clinic of Physical Medicine and Rehabilitation between March 2018 and August 2018. The study was performed in accordance with the Helsinki Declaration. Written informed consent was obtained from all patients.
ParticipantsA total of 107 patients who applied to the outpatient physical therapy and rehabilitation outpatient clinic for 3-6 months were included in this prospective and cross-sectional study. The study flowchart is shown in Figure 1.
Inclusion criteria were as follows: 1. Age range between 18-65 2. Patients diagnosed with fibromyalgia according to the American College of Rheumatology 1990 criteria.2 Exclusion criteria were as follows: Patients diagnosed with a known systemic(e.g. inflammatory rheumatic diseases, diabetes mellitus and systemic arterial hypertension), metabolic or endocrine disease as well as tumoral, neurologic or infectious diseases, patients with a history of trauma and surgery affecting neck area, patients who received trigger point injection therapy for neck pain within the last 6 months, patients with cervical disc herniation or myelopathy, spondylolisthesis, spondylolysis, cervicothoracic kyphoscoliosis, patients who had been receiving therapy for any psychiatric diagnosis for the last 3 months and antidepressant drug use, patients with history of neuropathic diseases, patients with a condition affecting neck muscles such as dystonia, inflammatory muscle disease and myopathy, pregnant patients were not included to the study.
Baseline AssessmentParticipants who met the inclusion criteria were examined in detail by a specialist physician, and their sociodemographic data comprising age, gender, occupation, marital status, education, and smoking were recorded. Routine blood laboratory values of all patients were checked, and also investigations like rheumatoid factor, anti CCP, ANA, vitamin D, calcium and DEXA scan to see for osteoporosis have been done.
Patients were divided into two groups. Those with a Cobb angle of 10°and below were classified as “Group 1” patients with loss of cervical lordosis, and those with Cobb angle above 10o were classified as “Group 2” patients’ control.
Radiological AssessmentAll the patients underwent lateral cervical spine radiography in neutral position. Cervical radiographs were taken while patients were standing and looking directly forward, their heads were in a neutral position, both upper extremities were maintained straight in a relaxed position on both sides of the body, and the X-RAYS were fixed to C4 vertebra. The distance between the X-RAY tube and film plate was stabilized at 150 cm. Patients whose inferior endplate of C7 vertebra was not included in the imaging area on lateral cervical spine radiography and whose head positions were in extension or flexion position were excluded from the study. Hard palate, lowest point of occiput, and all cervical vertebras to T1 were precisely and carefully selected for all radiographs.
All direct radiography examinations were performed with the digital imaging unit of Siemens Multix digital radiography (Siemens, Germany and Konica Minolta, Japan). Direct radiographs were stored in the Picture Archiving and Communications System (Extreme PACS, Türkiye) of the hospital.
Measurement MethodCervical lordosis was assessed according to C2 and C7. Cobb angles were measured by the anteroposterior radiograph of the cervical spine. The Cobb angle was measured with the four-line method, which includes drawing a line parallel to the inferior endplate of C2 that extends to the posterior margin of the spinous process, and another line parallel to the inferior endplate of C7. Sagittal spinal curvature in the neck and lower back was assessed with the Cobb angle on lateral radiography. A Cobb angle of 10o and below is accepted as loss of cervical lordosis. Those with a Cobb angle of 10o and below were classified “Group 1” and those with Cobb angle above 10o were called “Group 2”.
Primary OutcomeThe primary outcome of our study was the assessment of pain levels. A visual analogue scale (VAS) was used to measure the severity of pain (0-10 cm). Patients were asked to mark their subjective pain levels on a 10 cm scale. According to this scale, the value 0 means no pain, and the value 10 means very severe pain. The distance from the bottom of the scale to the marked point is recorded as centimeter.15
Secondary OutcomeThe secondary outcome of the study was the assessment of patients’ QOL and functional disability. Neck disability index (NDI) was used to measure the severity of neck disability in patients. This form has a total of 10 items, which include pain severity, personal care, lifting, reading, headache, concentration, work status, driving, sleep, and recreation. Scoring for each question ranges from 0 to 5 (0: the best health state and 5: the worst health state). High scores in patients mean serious disability. Total point was scored between 0 (no disability) and 100 (complete disability).16
Quality of Life Scale-Short Form (SF-36) was used to assess QOL. This scale assesses many aspects of health and consists of 36 questions with 8 subtitles (1). The 8 subscales are as follows: (1) Physical functioning; restriction of physical activities due to health problems, (2) social functioning; restriction of social activities due to physical and emotional reasons, (3) role functioning/physical; role restrictions due to physical health problems, (4) role functioning/emotional; role restrictions due to emotional problems, (5) mental health; general mental health related to psychological problem and wellness, (6) questions about objective assessment of wellness, energy and fatigue levels, (7) pain, and (8) sense of general health (feeling about own health). While the first four subscales assess the QOL related to physical health, the last four subscales assess the QOL related to mental health. The assessment is performed considering the last 4 weeks of the patient, and the scale is assessed between 0 point and 100 points in which score 100 shows good health state, the score 0 shows poor health state.17
We used G* Power version 3.1.2 (Heinrich Heine-Universität Düsseldorf, Düsseldorf, Germany) to calculate the sample size. Power analysis revealed that 54 patients were needed for group 1 and at least 53 patients were required for group 2 in 80% statistical power.
Ethical ApprovalThis study was approved by the Ethics Committee of Istanbul Health Sciences University Umraniye Training and Research Hospital (Date: 2011-11-21, No: B.10.1.TKH.4.34.H.GP.0.01/146).
Statistical AnalysisStatistical analysis was assessed using the IBM SPSS computer program (Statistical Package for the Social Sciences; IBM Corp, Armonk, NY, USA), release 22 for Microsoft Windows. The normality of distribution was assessed with the Shapiro-Wilk’s test. Student t test was used in two group comparisons of normally distributed parameters, and Mann Whitney U test was used in two group comparisons of non-normally distributed parameters as well as descriptive statistical methods (Mean, Standard deviation, and frequency). The chi-square test, Fisher Freeman Halton test, and Yates Continuity Correction were used in the comparison of qualitative data. The significance level was accepted as P < 0.05.
Reporting GuidelinesThis study was reported in accordance with the STROBE guidelines for cross-sectional studies.
Results
A total of 107 FMS patients (20 males and 87 females; median age: 44 years, range of age: 18–65 years) were included in the study (figure 1). After the evaluation of loss of cervical spine, the patients were recruited to group 1 or group 2. There were 54 and 53 patients in group 1 and 2, respectively. There was no statistically significant difference between the two groups in terms of age, gender, marital status, education level, smoking history, employment status, and ratio of male to female (p > 0.05). The demographic and clinical characteristics of the patients are shown in Table 1.
The mean Cobb angle degree of patients was 14.51 ± 11.31. VAS and NDI values were statistically significantly higher in Group 1 than in Group 2 (P = 0.034; P < 0.05). The assessment of outcome measures regarding the groups is given in Table 2.
Physical functioning, role-functioning/physical, role-functioning/emotional, emotional well-being, social functioning, pain, and general health scores were significantly lower in Group 1 than in Group 2 (P < 0.05). There was no statistically significant difference between the groups in terms of SF-36 energy/fatigue values (p > 0.05). The scores of SF-36 regarding the groups are shown in Table 3.
Discussion
The results of our study have revealed that reduced cervical lordosis angle in patients with FMS was associated with pain, neck disability, and QOL. Several studies on FMS and postural disorders have been performed.6,9,10 However, none of these studies have investigated the effect of decreased cervical lordosis on pain, disability, and QOL in patients with FMS.
An important function of spinal muscles is to keep the spine in a neutral position and to ensure optimal distribution of the loading in this area to all supportive structures. In patients with loss of cervical lordosis, neck muscle strength has decreased, especially in extensors,5 and strengthening exercises for these muscles were reported to increase muscle functions and decrease neck pain and disability.18 Isolated postural disorders in lumbar and cervical regions may also be responsible for the initial symptoms of FMS.19
Assessment of widespread pain, which is the main symptom of FMS, is important for the determination and follow-up of disease severity. In our study, the mean widespread pain score of the FMS group with reduced cervical lordosis angle was significantly higher compared to the control group. However, Grob et al. revealed that neck pain was not associated with cervical lordosis angle in a group of 54 patients with neck pain.3
Neurophysiological studies stated that a good body posture was mostly dependent on head posture and normal afferent nerve stimulation. Joints in the upper cervical region have a great number of receptors in the cervical spine and therefore, this region may have the greatest potential in the neuroaxis of mechanoreceptor afferentation in the spine.20 There is also evidence revealing that upper cervical afferents reach directly into vestibular and other high order CNS nuclei. This allows a less modified information input from the upper cervical articulations into the brain stem nuclei as opposed to the lower segments of the spine.21 However, the pathophysiological mechanisms underlying these negative clinical results are still unknown. Our results may be helpful in the assessment of pathophysiological mechanisms underlying widespread pain in fibromyalgia and thereby may be critical for a better understanding of potential clinical implications.
There are limited studies about the relationships between cervical spine diseases, pain, functional limitation, disability, and QOL in the literature. The QOL has been defined by the World Health Organization as “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns”. Abnormalities of natural curvature, such as loss of cervical lordosis or cervical kyphosis, were associated with poor QOL related to pain, disability, and health.22 Although the clinical effect of the loss of cervical lordosis is not well known, some studies have revealed that this problem was associated with cervicodorsal pain, headache, and poor QOL.23,24
SF36 is a widely used generic instrument to assess QoL. But fibromyalgia-specific questionnaires like FIQ have previously been used in some studies to determine the impact of disease regarding function, overall health status, and symptoms. In our study, we used a comprehensive tool ‘SF-36’ to define QoL on several different aspects comprising general health, function, emotional, social, fatigue, and pain. In addition, previous studies indicated that several deficiencies might be apparent, and the cumbersome scoring algorithm might be a barrier to the widespread clinical use of FIQ.25 In our study, health-related quality of life, physical functioning, role functioning/physical, role functioning/emotional, emotional well-being, social functioning, pain, and general health values were impaired in the patients with reduced cervical lordosis angle than in the other group.
Limitations
This study was designed to evaluate the effects of loss of cervical lordosis in patients with FMS. The first limitation was the wide range of ages of patients included in the study in which degenerative changes that occur especially after 40-50 years of age may affect shortening in the anterior or posterior vertebral column, and may impair the cervical alignment. The lack of a healthy control group and the absence of long-term outcomes were the other limitations of the study. However, the larger size of the study group and the lack of a similar study in the literature strengthen our results. Therefore, further large-scale, prospective, long-term, and controlled studies are needed to confirm these findings.
Conclusion
Our study reveals that FMS patients with loss of neck cervical lordosis had higher pain, more neck disability, and worse QOL. We suggest the assessment of cervical posture during the routine examination of FMS patients, which may help the physicians to develop more useful therapeutic strategies in the management of pain, functionality, and QOL.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Istanbul Health Sciences University Umraniye Training and Research Hospital (Date: 2011-11-21, No: B.10.1.TKH.4.34.H.GP.0.01/146)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Author Contributions (CRediT Taxonomy)
Conceptualization: S.G.A., E.E.B.
Methodology: S.G.A., Ö.G.
Formal Analysis: Ö.G.
Investigation: S.G.A., E.E.B.
Data Curation: S.G.A.
Writing – Original Draft Preparation: S.G.A.
Writing – Review & Editing: Ö.G., E.E.B., A.G.
Supervision: E.E.B., A.G.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
ANA: Antinuclear Antibody
anti-CCP: Anti–Cyclic Citrullinated Peptide
CNS: Central Nervous System
DEXA: Dual-Energy X-ray Absorptiometry
FMS: Fibromyalgia Syndrome
NDI: Neck Disability Index
PACS: Picture Archiving and Communication System
PF: Physical Functioning
QOL: Quality of Life
RE: Role Functioning/Emotional
RP: Role Functioning/Physical
SF-36: 36-Item Short Form Health Survey
VAS: Visual Analog Scale
References
-
Rooks DS. Fibromyalgia treatment update. Curr Opin Rheumatol. 2007;19(2):111-117.
-
Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum.1990;33(2):160-172. doi:10.1002/art.1780330203
-
Hiemeyer K, Lutz R, Menninger H. Dependence of tender points upon posture: a key to the understanding of fibromyalgia syndrome. J Manual Med. 1990;5:169-174.
-
Müller A, Hartmann M, Eich W. Inanspruchnahme medizinischer Versorgungsleistungen bei Patienten mit Fibromyalgiesyndrom (FMS). Schmerz. 2000;14(2):77-83.
-
Alpayci M, Şenköy E, Delen V, et al. Decreased neck muscle strength in patients with the loss of cervical lordosis. Clin Biomech (Bristol, Avon). 2016;33:98-102.
-
Alpayci M, Ilter S. Isometric exercise for the cervical extensors can help restore physiological lordosis and reduce neck pain: a randomized controlled trial. Am J Phys Med Rehabil. 2017;96(9):621-626.
-
Lee MY, Jeon H, Choi JS, Park Y, Ryu JS. Efficacy of modified cervical and shoulder retraction exercise in patients with loss of cervical lordosis and neck pain. Ann Rehabil Med. 2020;44(3):210-217.
-
Núñez-Fuentes D, Obrero-Gaitán E, Zagalaz-Anula N, et al. Alteration of postural balance in patients with fibromyalgia syndrome: a systematic review and meta-analysis. Diagnostics (Basel). 2021;11(1):127. doi:10.3390/diagnostics11010127
-
Pérez-de-Heredia-Torres M, Huertas-Hoyas E, Martínez-Piédrola R, et al. Balance deficiencies in women with fibromyalgia assessed using computerised dynamic posturography: a cross-sectional study in Spain. BMJ Open. 2017;7(7):e016239. doi:10.1136/bmjopen-2017-016239
-
Sempere-Rubio N, López-Pascual J, Aguilar-Rodríguez M, et al. Characterization of postural control impairment in women with fibromyalgia. PLoS One. 2018;13(5):e0196575. doi:10.1371/journal.pone.0196575
-
Umay E, Ulas U, Unlu E, et al. Importance of cutaneous silent period in fibromyalgia and its relationship with disease characteristics, psychological disorders, and quality of life. Rev Bras Reumatol. 2013;53(3):288-295.
-
Macovei LA, Rezuş E. Cervical spine lesions in rheumatoid arthritis patients. Rev Med Chir Soc Med Nat Iasi. 2016;120(1):70-76.
-
Sempere-Rubio N, Aguilar-Rodríguez M, Inglés M, et al. Physical condition factors that predict a better quality of life in women with fibromyalgia. Int J Environ Res Public Health. 2019;16(17):3173. doi:10.3390/ijerph16173173
-
Toprak Celenay S, Mete O, Coban O, Oskay D, Erten S. Trunk position sense, postural stability, and spine posture in fibromyalgia. Rheumatol Int. 2019;39(12):2087-2094.
-
Turk DC, Melzack R, eds. Handbook of Pain Assessment. New York, NY: Guilford Press; 1992:1-11
-
Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther. 1991;14(7):409-415.
-
Ware JE Jr. SF-36 health survey update. Spine (Phila Pa 1976). 2000;25(24):3130-3139. doi:10.1097/00007632-200012150-00008
-
Borisut S, Vongsirinavarat M, Vachalathiti R, Sakulsriprasert P. Effects of strength and endurance training of superficial and deep neck muscles on muscle activities and pain levels of females with chronic neck pain. J Phys Ther Sci. 2013;25(9):1157-1162. doi:10.1589/jpts.25.1157
-
Müller W, Kelemen J, Stratz T. Spinal factors in the generation of fibromyalgia syndrome. Z Rheumatol. 1998;57(Suppl 2):36-42.
-
Karnath HO, Konczak J, Dichgans J. Effect of prolonged neck muscle vibration on lateral head tilt in severe spasmodic torticollis. J Neurol Neurosurg Psychiatry. 2000;69(5):658-660. doi:10.1136/jnnp.69.5.658
-
Bankoul S, Neuhuber WL. A cervical primary afferent input to vestibular nuclei as demonstrated by retrograde transport of wheat germ agglutinin-horseradish peroxidase in the rat. Exp Brain Res. 1990;79(2):405-411.
-
McAviney J, Schulz D, Bock R, Harrison DE, Holland B. Determining the relationship between cervical lordosis and neck complaints. J Manipulative Physiol Ther. 2005;28(3):187-193. doi:10.1016/j.jmpt.2005.02.015
-
Tan LA, Straus DC, Traynelis VC. Cervical interfacet spacers and maintenance of cervical lordosis. J Neurosurg Spine. 2015;22(5):466-469.
-
Korovessis P, Mpountogianni E, Syrimpeis V, et al. Quality of life in adult patients receiving cervical fusion for fresh subaxial cervical injury: the role of associated spinal cord injury. Biomed Res Int. 2021;2021:9931535. doi:10.1155/2021/9931535
-
Bennett RM, Friend R, Jones KD, et al. The revised Fibromyalgia Impact Questionnaire (FIQR): validation and psychometric properties. Arthritis Res Ther. 2009;11(4):R120. doi:10.1186/ar2783
Figures
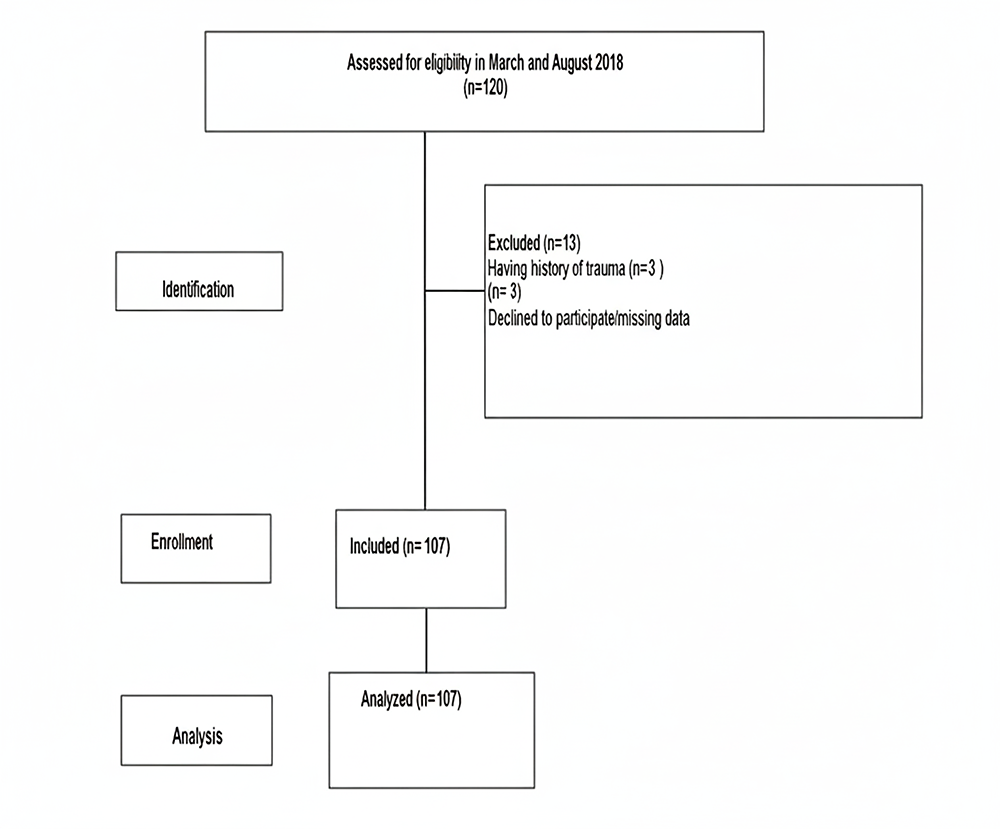
Figure 1. STROBE flow chart. STROBE, strengthening the reporting of observational studies in epidemiology
Tables
Table 1. Basic clinical characteristics of all patients
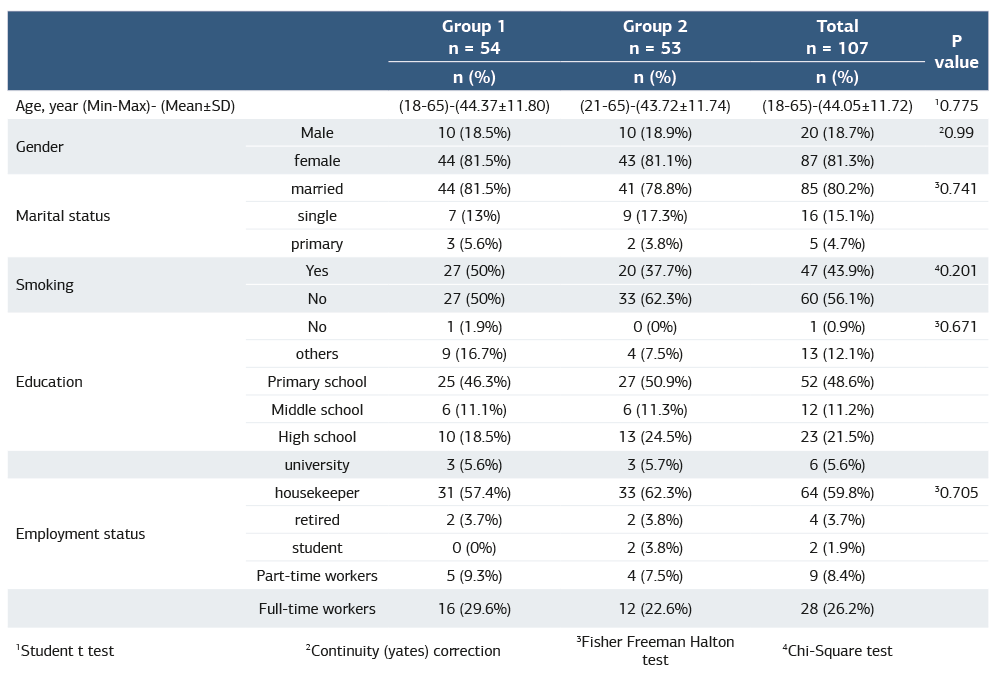
Table 2. Assessment of other scale values between the groups
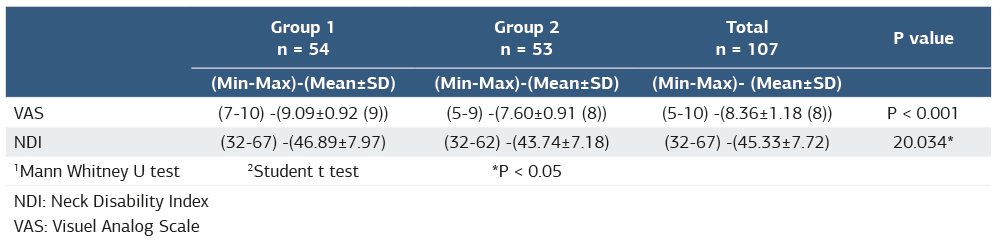
NDI: Neck Disability Index VAS: Visuel Analog Scale
Table 3. Assessment of SF-36 values between group 1 and group 2
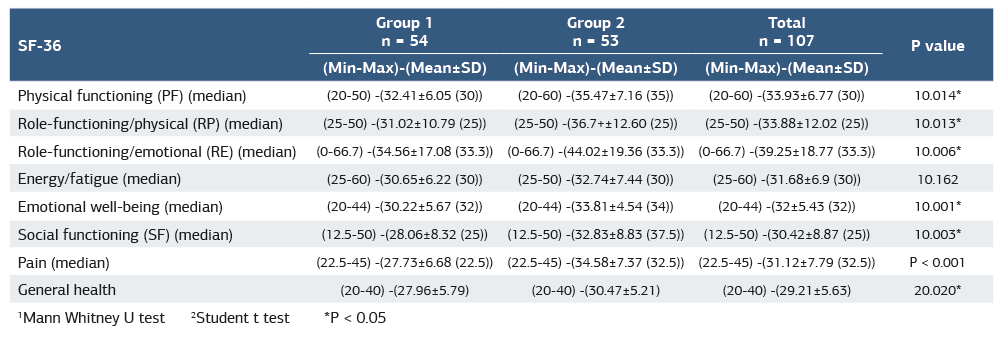
1 Mann Whitney U test 2 Student t test *P < 0.05
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Sevgi Gümüş Atalay, Ömer Gezginaslan, Emine Esra Bilir, Ali Gür. Loss of cervical lordosis and association of fibromyalgia syndrome. Ann Clin Anal Med 2026;17(Suppl 1):S28-33
- Received:
- March 23, 2025
- Accepted:
- July 3, 2025
- Published Online:
- July 15, 2025
- Printed:
- February 20, 2026