
Immune response characteristics and tiered treatment for secondary immune thrombocytopenia with different types of infection
Immune response and tiered treatment for SITP with infections
Authors
Abstract
Aim Secondary immune thrombocytopenia (SITP) is characterized by a low platelet count in peripheral blood. Pathogen infections are common secondary causes of SITP. This study aimed to characterize the destruction of megakaryocytes and platelets induced by humoral or cellular immune responses to infections caused by various types of pathogens in SITP patients, and to explore the treatment strategies for SITP.
Methods This study included 153 SITP patients and 30 non-SITP patients. Serological tests, bacteria and fungi tests, mycoplasma and virus tests, Wright-Giemsa staining, fluorescence-activated cell sorting (FACS), and immunofluorescence staining were conducted to examine the infection types, activation state of immune cells, and expression levels of specific antigens on megakaryocytes.
Results Laboratory examination results showed that 96 SITP patients were infected with Escherichia coli (E. coli), which activated a humoral immune response. The left 57 SITP patients were accompanied by chronic Hepatitis B Virus (HBV) infection, which activated cellular immunity. Pathological damage to megakaryocytes and platelets by different immune responses activated by different types of pathogens may explain the complex clinical symptoms of SITP.
Conclusion Tiered diagnosis and treatment based on clinical symptoms and laboratory diagnostic data can improve the efficacy of SITP treatment.
Keywords
Introduction
Secondary immune thrombocytopenia (SITP) is an autoimmune hemorrhagic disease with complex and varied clinical manifestations.1,2 Mild cases have no bleeding phenotype, whereas serious cases may suffer severe bleeding, which leads to high mortality. Although some SITP patients may have detectable underlying causes such as pathogen infection and vaccination, SITP is still a diagnosis of exclusion even today.3,4 It is believed that SITP is related to loss of immune tolerance to platelet autoantigen, resulting in premature platelet destruction and a relative inadequacy of platelet production.5 Recently, T-cell-mediated apoptosis of megakaryocytes and T-cell destruction of platelets have been recognized as pathogenic mechanisms of SITP.6,7
Historically, the treatment of SITP mainly relies on immune-suppressive drugs, which may bring down patients’ quality of life.8 With growing knowledge about the pathogenesis of SITP, new treatment strategies, including the thrombopoietin receptor agonist (TPO-RA), syk inhibitor, Fcγ receptor (FcγR) inhibition, and Bruton tyrosine kinase inhibitors, have been developed.9,10,11 Considering the complexity of the causes of SITP, although great progress has been made in SITP treatment, further researches regarding the pathogenesis and treatment of SITP are still needed in the paradigm shift from immune suppression to new, more targeted therapies. As pointed out in the latest expert consensus of the Thrombosis and Hemostasis Group of the Chinese Medical Association in 2023, long-term use of glucocorticoids, intravenous immunoglobulin (IVIG), TPO, TPO-RA, and splenectomy is a high-risk factor for inducing SITP complicating thrombosis/embolism.
Infection is a significant contributor to the development of SITP. Our previous studies have shown that SITP patients are usually accompanied by infections that activate the innate immune response.12 Galgano et al. also suggested that infections might play a role in SITP pathogenesis, and infections were associated with an exacerbation of thrombocytopenia.13 However, the relationship between platelet destruction and pathogen infection in SITP patients remains unclarified. In addition, there are few studies focusing on the treatment strategies for SITP patients with infections by different types of pathogens.
Our clinical observations indicate that patients with SITP frequently present with concurrent infections from E. coli and Hepatitis B Virus (HBV). Notably, when these infections are effectively managed, platelet counts in SITP patients tend to normalize. Therefore, this study aims to elucidate the immune response characteristics of SITP patients infected with E. coli or HBV and to offer evidence-based suggestions for pharmacological interventions tailored to infectious cases of SITP.
Materials and Methods
Patient SelectionThis study focused on SITP patients whose platelet counts were below 30×109/L and who exhibited laboratory-confirmed infections. The inclusion criteria: I) At least two consecutive blood routine examinations indicating platelet counts lower than 30×109/L and with symptoms of active hemorrhage; II) No significant abnormalities observed in blood cell morphology through peripheral blood smear microscopy; III) Presence of infection; IV) Adults aged 18 and older. The exclusion criteria: I) Patients with multiple types of infections; II) Patients diagnosed with other diseases in addition to thrombocytopenia and infection; III) Patients who have taken medication prior to the test or have undergone splenectomy; IV) Patients who refuse to give informed consent.
Clinical DataThis study encompasses 153 confirmed cases of SITP diagnosed in Zibo 148 Hospital from 2010 to 2022, with ages ranging from 29 to 76 years. Among the included patients, there were 136 females and 17 males. The platelet count of the 153 SITP patients at initial diagnosis ranged from 4×109/L to 30×109/L. Thirty patients diagnosed solely with iron deficiency anemia in the hematology department of Zibo 148 Hospital during the same period were selected as controls. These patients exhibited platelet counts ranging from 230 to 490×109/L and did not present any signs of bacterial, viral, or parasitic infections. Additionally, there was no significant difference in other clinical data between the two groups.
Bacteria and Fungi TestingFor SITP patients with suspected infections, specimens were collected from throat swabs, outer ear secretions, sputum, midstream urine, vaginal secretions, and other relevant sources. The samples were inoculated onto solid culture media for bacteria and fungi separately and incubated under both aerobic and anaerobic conditions at 37℃ (for bacteria) or 28℃ (for fungi). The suspected pathogens were identified using a mass spectrometer (MALDI-8020, Shimadzu).
Mycoplasma and Virus TestingMycoplasma Pneumoniae was detected using a PCR Detection Kit (catalog No: PC3540) purchased from Beijing Solarbio Science & Technology Co., Ltd., Beijing, China. The ELISA kits for detection of HBV (catalog No: BY-EH119578), Epstein Barr Virus (EBV) (catalog No: BY-EH112251), Cytomegalovirus (CMV) (catalog No: BY-EH113011), and Herpes Simplex Virus (HSV-I/II) (catalog No: BY-EH119549), were obtained Byabscience, Nanjing, China. The testing was conducted in accordance with the manufacturer’s instructions.
Serum Antibody TestingTo evaluate the status of humoral immune activation, the levels of different types of platelet antibodies in the serum were tested. The ELISA kits for platelet antibody IgG (PA-IgG), PA-IgA, and PA-IgM detection (catalog No: SEKH-0209, SEKH-0207, and SEKH-0218) were purchased from Beijing Solarbio Science & Technology Co., Ltd., Beijing, China. The ELISA kits were operated as instructed by the manufacturer.
Flow CytometryThe proportion of lymphocyte subsets in peripheral blood was detected by FACS. The following lymphocyte subsets were analyzed: CD3, CD4, CD8, CD16, CD19, CD45, and CD56. Immunofluorescence monoclonal antibodies targeting human peripheral blood lymphocyte subgroups were purchased from BD Biosciences (catalog No: 340182). We followed the experimental procedure outlined by Sun et al.14 Data were obtained using LSR Fortessa X-20 instruments (BD Biosciences) and analyzed by FlowJo (version 10.8).
Observation of Cell Morphology and Activation StatusTo identify the morphological changes of megakaryocytes in bone marrow, bone marrow smears were prepared and stained with the Wright-Giemsa stain solution according to the technical procedure of the manufacturer, and the morphology of megakaryocytes was observed under a fluorescence microscope (SBX51, Olympus). To analyze the activation status of megakaryocytes and macrophages (Mφ), the expression of IgG and FcγRI on these cells was analyzed by immunofluorescence. The mouse anti-human IgG monoclonal antibody (catalog No: ab239260) and mouse anti-human FcγRI monoclonal antibody (catalog No: ab119828) were acquired from Abcam.
Ethical ApprovalThis study was approved by the Ethics Committee of Qilu Medical University (Date: 2023-03-06, No: YXLL2023019).
Statistical AnalysisStatistical analysis was carried out using SPSS 21.0 for Windows (SPSS, Chicago, IL). Measurement data were presented as the mean ± standard deviation. The means of the two groups were compared by t-test, while the differences between three or more group means were analyzed using ANOVA. For multiple comparisons, Bonferroni’s correction was followed. Comparisons of rates were performed by chi-square test.
P < 0.05 was considered statistically significant.
Reporting GuidelinesThis study was reported in accordance with the STROBE guidelines.
Results
Infection Status of the SITP Patients InvestigatedResults of serological tests showed that levels of IgM against pathogens such as CMV, HSV I/II, and Mycoplasma pneumoniae in the 153 SITP patients were in the normal range, levels of IgG were normal or increased to varying degrees, and no EBV was detected. There were 96 patients infected by pathogenic E. coli which could be isolated from midstream urine or vaginal secretions, but these cases were negative for fungal infection. The left 57 patients were positive for HBV infection but negative for bacterial infection.
E. Coli Infection Leads to Activation of the Humoral Immune Response in SITP PatientsFor SITP patients with E. coli infection, levels of PA-IgG rose to 80.72 ± 12.50 μg/L, but levels of PA-IgA and PA-IgM were in the normal range (Table 1), and the proportion of CD3+CD8+T cells in peripheral blood decreased to 10.35 ± 2.26%, but the proportion of CD19+B cells increased to 34.19 ± 2.28% (Table 2, Figure 1C and D). The CD4/CD8 ratio varies among patients infected with different kinds of pathogens (Table 2, Figure 1A, C, and E). In ITP patients infected by E. coli, the CD4/CD8 ratio was observed to be 38.52/10.35, whereas in HBV-infected ITP patients, the CD4/CD8 ratio was recorded at 37.49/42.16.
Activation of the Humoral Immune Response Leads to Damage to Megakaryocytes and Platelets
For SITP patients with E. coli infection, proliferation of megakaryocytes was active in the bone marrow, but the proportion of platelet-producing megakaryocytes was reduced, and naked megakaryocytes could be commonly observed (Figure 2A). Damaged megakaryocytes were positive for anti-human IgG (Figure 2B). Moreover, expression of FcγRI on Mφ membrane was up-regulated, and many platelets could be seen attached to the surface of Mφ (Figure 2C).
According to our clinical treatment experience, for SITP patients with E. coli infection, anti-infection combined with saturated glucocorticoid pulse treatment is effective. The dose of glucocorticoid can be reduced after one week. For patients with severe SITP, the administration of IVIG pulse therapy, in conjunction with the aforementioned treatments, can yield enhanced therapeutic efficacy.
HBV Infection Activates Cellular Immune Responses in SITP PatientsLevels of PA-IgG/M/A in the 57 SITP patients with HBV infection were in the normal range (Table 1). Compared with both the non-SITP control patients and the SITP patients infected by E. coli, the proportion of CD3+CD8+T cells in peripheral lymphocyte subsets of SITP patients with HBV infection was significantly increased, but the proportion of CD16+/56+NK cells was significantly decreased (Table 2, Figure 1E and F). HBV infection resulted in abnormal growth and development of megakaryocytes, which exhibited uneven shape and size, and lymphocytes attacking megakaryocytes could be observed in the bone marrow (Figure 3A), which explained the damage to megakaryocytes. For SITP patients with HBV infection, megakaryocytes in the bone marrow were negative for anti-human IgG (Figure 3B), and FcγRI was sparsely expressed on Mφ membrane (Figure 3C).
Based on our clinical experience, the effect of glucocorticoid therapy is poor on SITP patients with HBV infection. Long-term or large doses of glucocorticoids can lead to increased HBV viral load and aggravated liver function damage. Anti-HBV drugs such as Entecavir combined with Cyclosporin A (CsA) can inhibit the destruction of megakaryocytes and platelets by T lymphocytes, thereby increasing the number of platelets.
Discussion
Initially, it was recognized that the pathogenesis of SITP was due to the destruction of megakaryocytes and platelets by abnormal activation of humoral immunity. Therefore, the treatment strategy with saturated glucocorticoid was adopted.15 If the saturated glucocorticoid treatment was effective, then the dose of glucocorticoid would be gradually reduced.16 For steroid-refractory SITP patients, sequential treatment with immunosuppressive drugs (CsA, decitabine, etc.) combined with targeted drugs (anti-CD19 or anti-CD20 antibodies), and even splenectomy, would be applied.17 All these therapies focus on suppressing immune responses or removing the primary site of platelet clearance and auto-antibody production, rather than eliminating the causes of immune activation.
The CD4/CD8 ratio is a measure of the strength of the immune system. The impact of different pathogens on the CD4/CD8 ratio among SITP patients has not been previously reported. We observed that the CD4/CD8 ratio in SITP patients infected with E. coli was significantly higher than that of the control group, whereas the CD4/CD8 ratio in HBV-infected SITP patients was notably lower than that of the control group. The findings suggest a marked difference in immune responses induced by various pathogens. Additionally, Malik et al. 7 found that chronic ITP patients had significantly lower CD4/CD8 ratios compared with age-matched controls. This discrepancy also highlights the difference in immune responses between ITP and SITP patients.
The SITP patients with E. coli infection are characterized by increased proportion of CD19+B cells, decreased proportion of CD3+CD8+T cells, increased level of platelet-specific PA-IgG in peripheral blood, anti-human IgG positive for bone marrow megakaryocytes, and high expression of FcγRI on Mφ membrane, suggesting activation of humoral immune response.
Humoral immune responses are crucial for protection against extracellular bacterial infection. Gram-negative bacteria express at their surface various amphiphilic molecules, including the lipopolysaccharide, which is a ligand of toll-like receptor 4 on the surface of platelets.18 The binding of platelets and bacteria then activates Mφ and neutrophils to mediate inflammation and inhibits the spread of pathogens.17,19,20 If the infection is not effectively controlled, the aggregates of platelets and pathogenic bacteria may affect the structure and function of glycoprotein IIb/IIIa on the platelet membrane, making the damaged glycoprotein IIb/IIIa become an autoantigen, thus activating a specific humoral immune response against glycoprotein IIb/IIIa.15,21 Antibodies against glycoprotein IIb/IIIa bind with megakaryocytes and platelets, inducing opsonization of Mφ, which upregulates expression of FcγRI as observed in SITP patients with E. coli infection (Figure 2C).
High doses of glucocorticoids can suppress the proliferation of proB-progenitors and inhibit transcription of B cell activating factor, thus inhibiting B cell maturation and plasma cell transformation to produce antibodies.21,22 For SITP patients infected with extracellular bacteria, effective anti-infection treatment combined with a short course of high-dose dexamethasone can achieve a better curative effect. For severe SITP patients, the addition of IVIG pulse treatment helps block the FcγRI on Mφ membrane, blocking the damage of Mφ to platelets, thus enhancing the efficacy of glucocorticoid treatment.
Cellular immunity responds very specifically to intracellular pathogens like viruses. We found that, in peripheral blood of SITP patients with HBV infection, the levels of platelet antibodies were normal, but the proportion of CD3+CD8+T cells increased significantly, indicating that HBV infection may lead to changes of antigen structure on megakaryocyte membrane which activate CD3+CD8+ cytotoxic T lymphocytes (CTL), then CTLs attack the abnormal megakaryocytes, affecting megakaryocyte development and platelet generation. Glucocorticoids can bind to T cell receptor (TCR), inhibiting the phosphorylation of multiple molecules in the T cell signaling pathway, and down-regulating the expression of interleukin 2.23 CsA can restrain the secretion of interleukin 2 by T helper 1 cells and suppress the activation of CTL.24 Therefore, on the basis of effective anti-HBV therapy, the combination of low-dose glucocorticoids and CsA has a good effect on the treatment of SITP patients with HBV infection.
Limitations
It should be noted that this study is subject to certain limitations. Firstly, patients with iron deficiency anemia were selected as controls. Use of iron deficiency anemia patients instead of healthy controls may have influenced immunological comparisons. Although the immune characteristics of individuals with iron deficiency anemia are comparable to those of healthy individuals, variations in other indicators may influence the results. Secondly, there exists a wide range of pathogens that can lead to SITP; however, only E. coli and HBV were investigated in this research. While this study provides significant insights for the treatment of SITP resulting from bacterial and viral infections, further research is necessary to explore the immune response characteristics and treatment strategies for SITP associated with infections caused by other types of pathogens. Moreover, our findings are primarily based on laboratory tests and clinical treatment experiences, lacking functional studies that could clarify the mechanisms underlying the immune responses.
Conclusion
Pathological damage to megakaryocytes and platelets by pathogen infection activated immune system may be an important factor in the pathogenesis of SITP. Different types of pathogens activate different kinds of effector cells and result in distinct patterns of damage to megakaryocytes and platelets. Therefore, SITP patients need to be checked for bacterial or viral infection; if infection is diagnosed, treatment strategies depending on infection types are suggested. Anti-infection treatments help eliminate the source of antibody production, while immunosuppressive drugs are beneficial to suppress the remaining infection-activated immune cells. In conclusion, classification of SITP according to pathogen types and laboratory diagnostic data helps enhance the efficacy of SITP treatment.
Declarations
Ethics Declarations
Ethical approval was obtained from the Ethics Committee of Qilu Medical University (Approval No: YXLL2023019).
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Written informed consent was obtained from all participants.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the General Programs of Qilu Medical University (grant number X24ZKZD01, JCYXKFFC202401, X24ZKMS06, JCYXKFFC202404, and JCYXKFPY202407).
Author Contributions (CRediT Taxonomy)
Conceptualization: L.S., W.C.
Investigation: W.C., Y.L., L.Z., J.W.
Data Curation: W.C., Y.L.
Writing – Original Draft Preparation: W.C.
Writing – Review & Editing: L.S., L.W., S.L.
Visualization: H.X.
Supervision: L.S.
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of this manuscript, including study design, data collection, analysis and interpretation of data, drafting and revising the manuscript, and approval of the final version.
Abbreviations
ANOVA: Analysis of Variance
CMV: Cytomegalovirus
CsA: Cyclosporin A
CTL: Cytotoxic T Lymphocyte
E. coli: Escherichia coli
EBV: Epstein–Barr Virus
FACS: Fluorescence-Activated Cell Sorting
FcγRI: Fc Gamma Receptor I
HBV: Hepatitis B Virus
HSV: Herpes Simplex Virus
ITP: Immune Thrombocytopenia
IVIG: Intravenous Immunoglobulin
Mφ: Macrophage
PA-IgG: Platelet-Associated Immunoglobulin G
SITP: Secondary Immune Thrombocytopenia
SPSS: Statistical Package for the Social Sciences
TCR: T Cell Receptor
TPO-RA: Thrombopoietin Receptor Agonist
References
-
Mititelu A, Onisai MC, Rosca A, Vladareanu AM. Current understanding of immune thrombocytopenia: a review of pathogenesis and treatment options. Int J Mol Sci. 2024;25(4):2163. doi:10.3390/ijms25042163
-
Goncalves I, Lewis C, Grainger B, Dring R, Lee N, Pasricha SR, et al. Thrombosis in patients with immune thrombocytopenia: incidence, risk, and clinical outcomes. Res Pract Thromb Haemost. 2024;8(1):102342.
-
Provan D, Arnold DM, Bussel JB, Chong BH, Cooper N, Gernsheimer T, et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019;3(22):3780-3817. doi:10.1182/bloodadvances.2019000812
-
Delshad M, Davoodi-Moghaddam Z, Pourbagheri-Sigaroodi A, Faranoush M, Abolghasemi H, Bashash D. Translating mechanisms into therapeutic strategies for immune thrombocytopenia (ITP): lessons from clinical trials. Thromb Res. 2024;235:125-147.
-
Gonzalez-Lopez TJ, Provan D, Barez A, et al. Primary and secondary immune thrombocytopenia (ITP): time for a rethink. Blood Rev. 2023;61:101112.
-
Yazdanbakhsh K, Provan D, Semple JW. The role of T cells and myeloid-derived suppressor cells in refractory immune thrombocytopenia. Br J Haematol. 2023;203(1):54-61.
-
Malik A, Sayed AA, Han P, et al. The role of CD8+ T-cell clones in immune thrombocytopenia. Blood. 2023;141(20):2417-2429.
-
Provan D, Semple JW. Recent advances in the mechanisms and treatment of immune thrombocytopenia. EBioMedicine. 2022;76:103820.
-
Ghanima W, Cooper N, Rodeghiero F, Godeau B, Bussel JB. Thrombopoietin receptor agonists: ten years later. Haematologica. 2019;104(6):1112-1123. doi:10.3324/haematol.2018.212845
-
Bussel JB, Arnold DM, Boxer MA, et al. Long-term fostamatinib treatment of adults with immune thrombocytopenia during the phase 3 clinical trial program. Am J Hematol. 2019;94(5):546-553.
-
Langrish CL, Bradshaw JM, Francesco MR, et al. Preclinical efficacy and anti-inflammatory mechanisms of action of the Bruton tyrosine kinase inhibitor rilzabrutinib for immune-mediated disease. J Immunol. 2021;206(7):1454-1468.
-
Sun L, Han B, Wu Q, et al. Immune mechanism and clinical significance of macrophage to medullary hematopoietic injury of immune-related hematocytopenia patients. Chin Med J (Engl). 2013;126(24):4696-4702.
-
Galgano L, Guidetti GF, Torti M, Canobbio I. The controversial role of LPS in platelet activation in vitro. Int J Mol Sci. 2022;23(18):10900. doi:10.3390/ijms231810900
-
Sun YX, Feng Q, Wang SW, Li X, Sheng Z, Peng J. HLA-G-ILT2 interaction contributes to suppression of bone marrow B cell proliferation in acquired aplastic anemia. Ann Hematol. 2022;101(4):739-748.
-
Cuker A, Neunert CE. How I treat refractory immune thrombocytopenia. Blood. 2016;128(12):1547-1554.
-
Cooper N, Ghanima W. Immune thrombocytopenia. N Engl J Med. 2019;381(10):945-955. doi:10.1056/NEJMcp1810479
-
Sun L, Wu Q, Han B, et al. Mechanisms of immune injury and heterogeneity of bone marrow hematopoietic cells island in patients with auto-immuno-related hematocytopenia. J Immunoassay Immunochem. 2014;35(4):378-387.
-
Ezzeroug Ezzraimi A, Hannachi N, Mariotti A, Rolain JM, Camoin-Jau L. Platelets and Escherichia coli: a complex interaction. Biomedicines. 2022;10(7):1636. doi:10.3390/biomedicines10071636
-
Siggins MK, Sriskandan S. Bacterial lymphatic metastasis in infection and immunity. Cells. 2021;11(1):33. doi:10.3390/cells11010033
-
Crickx E, Chappert P, Sokal A, et al. Rituximab-resistant splenic memory B cells and newly engaged naive B cells fuel relapses in patients with immune thrombocytopenia. Sci Transl Med. 2021;13(589):eabc3961. doi:10.1126/scitranslmed.abc3961
-
Porcelijn L, Huiskes E, Oldert G, Schipperus M, Zwaginga JJ, de Haas M. Detection of platelet autoantibodies to identify immune thrombocytopenia: state of the art. Br J Haematol. 2018;182(3):423-436.
-
Kamhieh-Milz J, Ghosoun N, Sterzer V, Salama A. Effect of glucocorticoid treatment on BAFF and APRIL expression in patients with immune thrombocytopenia (ITP). Clin Immunol. 2018;188:74-80.
-
Liu Z, Hu X, Liang Y, et al. Glucocorticoid signaling and regulatory T cells cooperate to maintain the hair-follicle stem-cell niche. Nat Immunol. 2022;23(7):1086-1097.
-
. Kaye J. Integrating T cell activation signals to regulate gene expression through cyclosporin-sensitive NFAT. J Immunol. 2023;211(3):323-324.
Figures
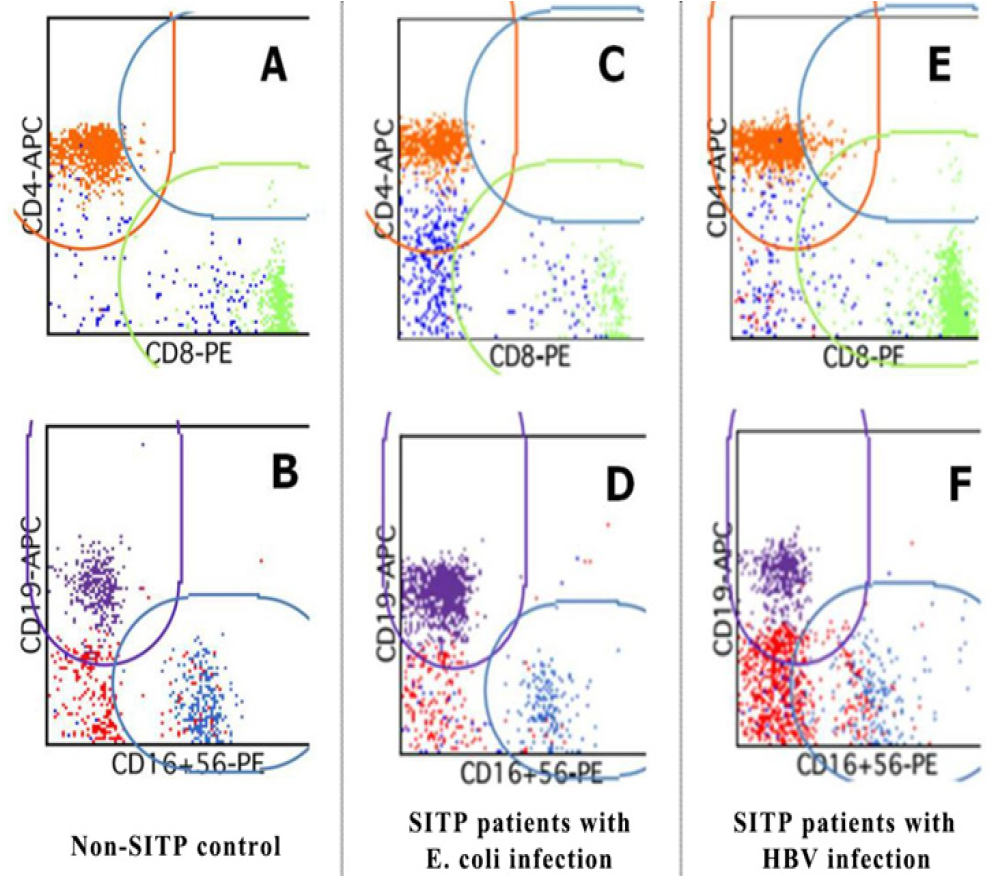
Figure 1. Lymphocyte subsets in peripheral blood among non-SITP patients and SITP patients were analyzed by FACS. In dot plots (A), (C), and (E), lymphocytes are gated by their CD4 and CD8 expression to separate CD4 single positive (gated by an orange line), CD8 single positive (gated by a green line), and CD4/CD8 double positive (gated by a blue line) T cells. Similarly, in dot plots (B), (D), and (F), lymphocytes are gated on the basis of CD19 and CD16/CD56 expression to separate B cells (gated by a purple line) and NK T cells (gated by a blue line). Cell
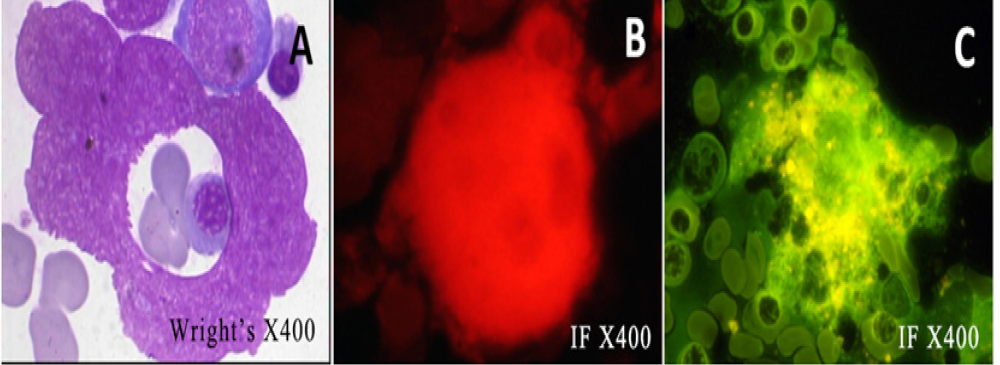
Figure 2. Destruction of bone marrow megakaryocytes and platelets by activation of humoral immune response in SITP patients with E. coli infection. (A) Wright’s staining of bone marrow showing naked megakaryocytes. Immunofluorescence staining showing anti-human IgG positive megakaryocyte (B) and activated Mφ with high expression of Fc gamma receptor I (FcγRI) (C)
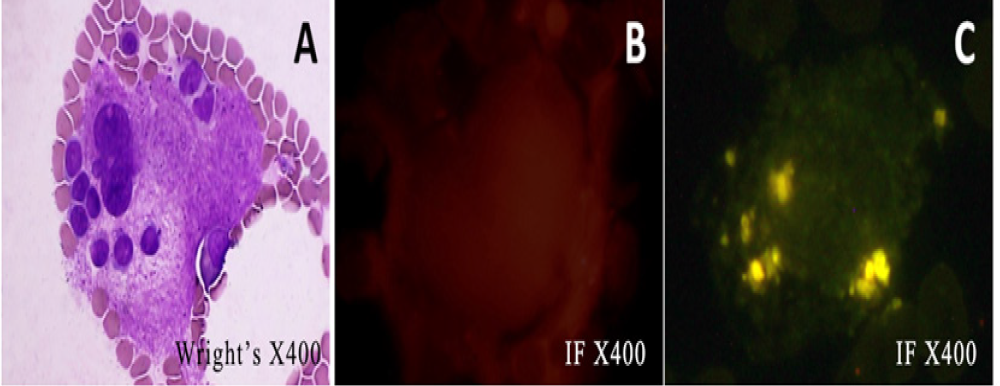
Figure 3. Destruction of bone marrow megakaryocytes and platelets by activation of cellular immune response in SITP patients with HBV infection. (A) Wright’s staining of bone marrow shows megakaryocytes being attacked by lymphocytes. Immunofluorescence staining showing anti-human IgG negative megakaryocyte (B) and activated Mφ with sparse expression of Fc gamma receptor I (FcγRI) (C)
Tables
Table 1. Effect of pathogen infections on the concentration of platelet antibodies in SITP patients

Table 2. Effect of pathogen infections on the percentage of peripheral lymphocyte subsets in SITP patients

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Weitong Cui, Yajun Liang, Lifei Sun, Lei Wei, Shuai Li, Linlin Zhang, Junwei Wang, Huaru Xue, Jinbiao Zhang, Qiangqiang Wu. Immune response characteristics and tiered treatment for secondary immune thrombocytopenia with different types of infection. Ann Clin Anal Med 2026;17(3):190-195
- Received:
- March 30, 2025
- Accepted:
- June 2, 2025
- Published Online:
- July 7, 2025
- Printed:
- March 1, 2026