
The impact of topographic localization of CIN 2-3 lesions in conization specimens on disease progression: A retrospective study
What is the importance of CIN 2-3 location?
Authors
Abstract
Aim To investigate the prognostic impact of the topographic localization of high-grade cervical intraepithelial neoplasia (CIN 2+) lesions within conization specimens on HPV persistence, cervical cytological abnormalities, and lesion recurrence.
Methods This retrospective study included 461 patients who underwent cold knife conization for CIN 2+ between October 2022 and July 2023. Patients were followed for 24 months with Hr-HPV testing and cervical cytology at 6-month intervals. The localization of CIN 2+ lesions was categorized into cervical quadrants based on clock-face orientation. Associations with HPV persistence, abnormal cytology, and CIN 2+ recurrence were analyzed.
Results At 24 months post-conization, Hr-HPV persistence was observed in 15.2%, abnormal cytology in 25.2%, and CIN 2+ recurrence in 2.8% of patients. While focal localization of primary CIN 2+ lesions in the upper quadrant of cone specimens was significantly more frequent (p<0.001), there was no significant association between lesion location (in either cone specimens or surgical margins) and Hr-HPV persistence (p=0.233 and 0.726), abnormal cytology (p =0.124 and 0.354), or recurrence (p = 1.000 for both comparisons).
Conclusion The topographic location of CIN 2+ lesions in conization specimens is not associated with Hr-HPV persistence, abnormal cervical cytology, or recurrence during follow-up. This is the first study to examine the prognostic relevance of lesion localization in cone specimens. Further large-scale prospective studies are needed to validate these findings.
Keywords
Introduction
Persistent infection with high-risk human papillomavirus (Hr-HPV) is associated with the development of cervical intraepithelial neoplasia (CIN) and cervical cancer.1 CIN is diagnosed through cytology, colposcopy, and histopathology and is classified as CIN 1, 2, or 3 based on the extent of epithelial involvement according to the Bethesda system.2
Ostör reported that the risk of progression to invasive cancer is approximately 1% for CIN 1, 5% for CIN 2, and 12% for CIN 3.3 In the treatment of high-grade cervical intraepithelial neoplasia (CIN 2 and CIN 3), ablative or excisional methods are preferred. Among excisional methods, cold knife conization, laser conization, and loop electrosurgical excision procedure (LEEP) are commonly used.4
Recurrent disease can be observed in 5–25% of patients after CIN treatment. Positive surgical margins following cervical excisional procedures are an important predictor of recurrence. In addition to margin status, factors such as lymphovascular space invasion, endocervical gland involvement, and Hr-HPV type are also associated with recurrence.5,6,7,8,9,10 Most studies on CIN recurrence are based on colposcopic biopsy results, and there is no consensus that has been reflected in clinical practice. More than half of high-grade cervical intraepithelial neoplasia cases after excisional procedures are detected within the first two years of follow-up.11 Therefore, close post-treatment monitoring of patients is crucial.
To date, no literature has examined whether the topographic location of high-grade cervical intraepithelial neoplasia within the conization specimen is associated with Hr-HPV persistence, cervical cytological abnormalities, or CIN recurrence. Clarifying this issue may influence the approach to the conization technique and postoperative follow-up strategies. In this study, we aimed to investigate the effect of the topographic location of high- grade cervical intraepithelial neoplasia within the conization specimen on disease progression following treatment.
Materials and Methods
The study protocol complied with the ethical principles of the Declaration of Helsinki, and all patients signed informed consent forms permitting the use of their clinical data. Patient data were obtained from the hospital’s electronic medical record database and individual patient files.
Between October 2022 and July 2023, 516 patients treated with cold knife conization in the gynecologic oncology clinic of Konya City Hospital were evaluated. Inclusion criteria were: presence of high-grade cervical intraepithelial neoplasia in the cone pathology, availability of Hr-HPV test and cytology results at 6, 12, and 24 months post-treatment, age over 24 years, and absence of any comorbid condition or medication history that could impair immune response. Patients with a diagnosis of malignancy or carcinoma in situ, a history of re- conization, irregular follow-up records for Hr-HPV or cytology, or an impaired immune response were excluded. Twenty-nine patients were excluded due to not meeting the inclusion criteria, 11 had discontinued treatment, and 15 were lost to follow-up. As a result, 461 patients were included in the final analysis.
The pathology and HPV DNA test results were evaluated in accordance with the 2019 guidelines of the American Society for Colposcopy and Cervical Pathology (ASCCP).12 The conization procedures were performed either using a scalpel (cold knife conization) or a needle-tip cautery, based on the surgeon’s preference, by a specialized gynecologic oncology surgical team. The excised specimens were marked at the noon position with a suture to orient the sample for topographical analysis.
Experienced pathologists evaluated the cytology and surgical specimens. The location of the lesion was determined according to the clock-face orientation described in pathology reports for topographical analysis. Lesions located between 10 and 1 o’clock were defined as the upper quadrant; between 1 and 4 o’clock as the left quadrant; between 4 and 7 o’clock as the lower quadrant; and between 7 and 10 o’clock as the right quadrant. Lesions falling on the borderlines at 1, 4, 7, and 10 o’clock were assigned to both adjacent quadrants. All specimens were reviewed by expert pathologists.
Specimens demonstrating HPV-related changes or CIN 1 were classified as low-grade cervical intraepithelial neoplasia, whereas those with CIN 2 or CIN 3 were categorized as high- grade cervical intraepithelial neoplasia (CIN 2+). Positive surgical margins were defined as the presence of CIN 2+ at the endocervical and/or ectocervical margins of the specimen. Within 24 months after conization, HPV DNA results, cervical cytology, and CIN 2+ lesions detected through colposcopy were analyzed based on the clock-face localization of CIN 2+ lesions within the conization specimen and surgical margins. HPV DNA testing was performed using the Hybrid Capture 2 (hc2) assay (Qiagen, Hilden, Germany).
Cervical cytological abnormalities assessed included atypical squamous cells of undetermined significance (ASC-US), low- grade squamous intraepithelial lesion (LSIL), high-grade squamous intraepithelial lesion (HSIL), atypical squamous cells – cannot exclude HSIL (ASC-H), and atypical glandular cells (AGC). All patients were followed up for 2 years after conization, with co-testing (Hr-HPV DNA and Pap smear) performed at 6-month intervals. The presence of a CIN 2+ lesion detected through biopsy or endocervical curettage during colposcopy was considered a recurrence. Colposcopic evaluations were conducted based on the nomenclature proposed by the International Federation for Cervical Pathology and Colposcopy (IFCPC) in 2011.13
Ethical ApprovalThis study was approved by the Ethics Committee of Konya City Hospital (Date: 2025-05-12, No: 87).
Statistical AnalysisStatistical analyses were performed using SPSS version 22 (IBM Corp., Chicago, IL, USA). Descriptive statistics were presented as numbers and percentages for categorical variables, and as mean ± standard deviation (SD) for continuous variables. Differences between groups were analyzed using the Chi- square test and Fisher’s exact test as appropriate. A p-value of less than 0.05 was considered statistically significant.
Reporting GuidelinesThis study was reported in accordance with the STROBE reporting guideline.
Results
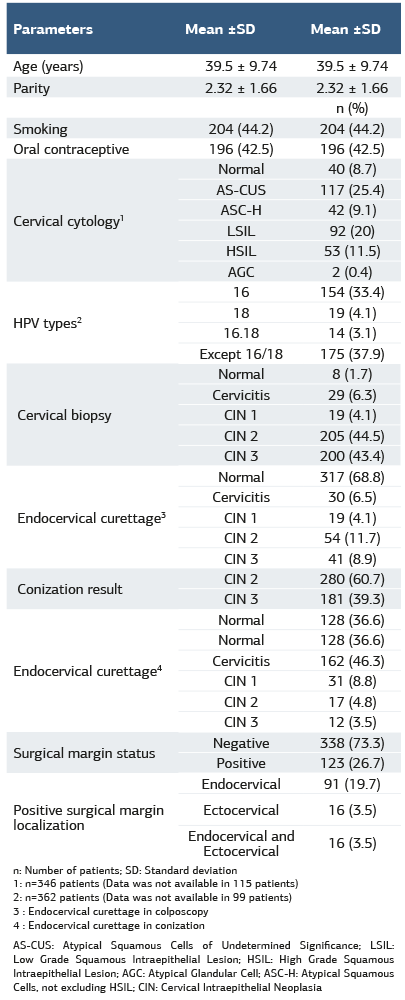
The mean age of the 461 patients included in the study was 39.5 ± 9.74 years, and the mean parity was 2.32 ± 1.66. Among the participants, 44.2% were smokers and 42.5% were using oral contraceptives. Cervical cytology results were as follows: ASC-H in 42 patients (9.1%), LSIL in 92 (20%), HSIL in 53 (11.5%), and AGC in 2 (0.4%). HPV type 16 was positive in 154 patients (33.4%), type 18 in 19 (4.1%), both types 16 and 18 in 14 (3.1%), and other high-risk HPV types (excluding 16 and 18) in 175 patients (37.9%). Histopathologic results from cervical biopsies showed CIN 1 in 19 patients (4.1%), CIN 2 in 205 (44.5%), and CIN 3 in 200 (43.4%). Endocervical curettage performed during colposcopy revealed CIN 1 in 19 patients (4.1%), CIN 2 in 54 (11.7%), and CIN 3 in 41 (8.9%). Conization pathology showed CIN 2 in 280 patients (60.7%) and CIN 3 in 181 (39.3%). Endocervical curettage results during conization revealed CIN 1 in 31 patients (8.8%), CIN 2 in 17 (4.8%), and CIN 3 in 12 (3.5%). Positive surgical margins were detected in 123 patients (26.7%), of whom 91 (19.7%) had endocervical margin positivity, 16 (3.5%) had ectocervical margin positivity, and 16 (3.5%) had both endocervical and ectocervical margin involvement (Table 1).
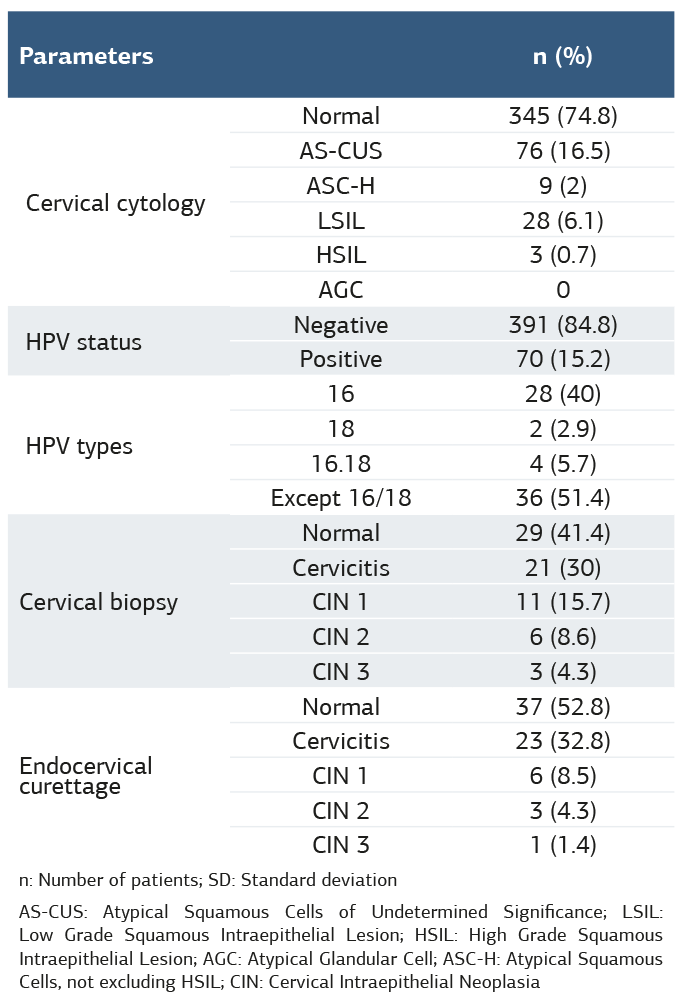
At the 12-month follow-up after conization, cervical cytology revealed ASC-US in 76 patients (16.5%), ASC-H in 9 (2%), LSIL in 28 (6.1%), and HSIL in 3 patients (0.7%). Hr-HPV was found to be positive in 70 patients (15.2%). Among these, HPV 16 was detected in 28 patients (40%), HPV 18 in 2 (2.9%), both HPV 16 and 18 in 4 (5.7%), and other high-risk HPV types (excluding 16 and 18) in 36 patients (51.4%). Cervical biopsy performed during colposcopy at follow-up revealed CIN 2 in 6 patients (8.6%) and CIN 3 in 3 patients (4.3%). Endocervical curettage results showed CIN 2 in 3 patients (4.3%) and CIN 3 in 1 patient (1.4%) (Table 2).
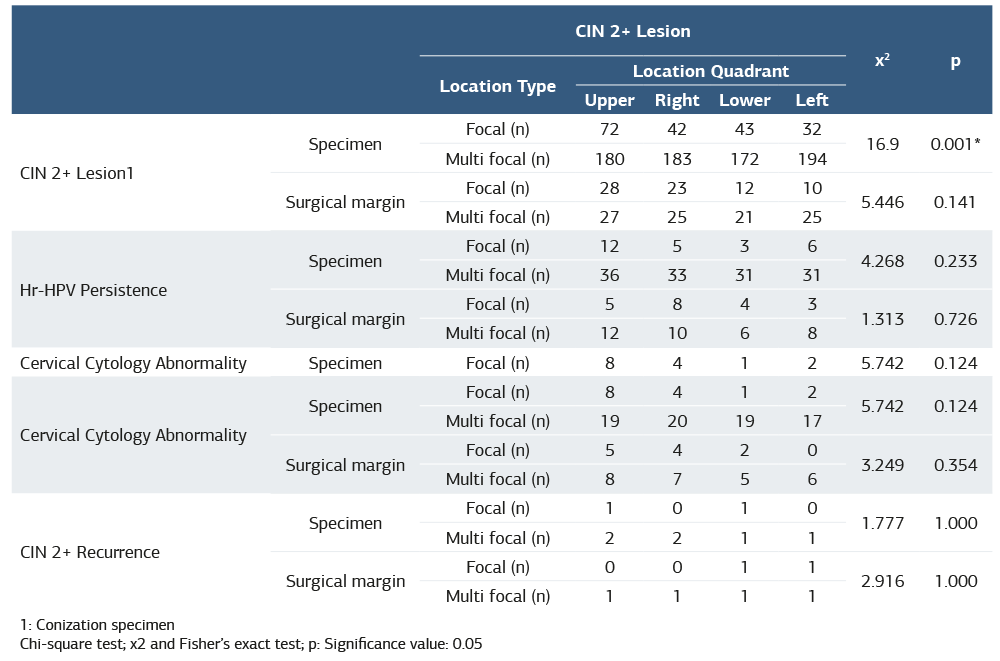
The number of CIN 2+ lesions in the cone specimens was 72 in the upper quadrant, 42 in the right quadrant, 43 in the lower quadrant, and 32 in the left quadrant. Focal localization of CIN 2+ lesions was significantly more frequent in the upper quadrant (p=0.001) (Table 3). The number of CIN 2+ lesions at the surgical margins was 28 in the upper quadrant, 23 in the right quadrant, 12 in the lower quadrant, and 10 in the left quadrant.
The distribution of CIN 2+ lesions in the surgical margins across cervical quadrants was not statistically significant (p =0.141). At the 24-month follow-up after conization, Hr-HPV persistence was detected in 70 patients (15.2%). The topographic distribution of CIN 2+ lesions in both the conization specimens and the surgical margins was not significantly associated with Hr-HPV persistence (p=0.233 and p=0.726, respectively). At the 24-month follow-up after conization, cervical cytological abnormalities were observed in 116 patients (25.2%). The topographic distribution of CIN 2+ lesions in both the cone specimens and the surgical margins showed no significant association with abnormal cervical cytology results (p=0.124 and p=0.354, respectively) (Table 3).
Discussion
At 24 months post-conization, Hr-HPV persistence was observed in 15.2% of patients, abnormal cervical cytology in 25.2%, and CIN 2+ recurrence in 2.8%. Among patients with recurrent CIN 2+ lesions, the initial CIN 2+ lesions were focal in 30.8% and multifocal in 69.2%. Focal localization of primary CIN 2+ lesions in the upper quadrant of the cone specimen was statistically significant (p=0.001). However, no association was found between the quadrant localization of CIN 2+ lesions in the cone specimen or surgical margins and Hr-HPV persistence, abnormal cytology, or CIN 2+ recurrence at 24-month follow-up. In a study by Baser et al., Hr-HPV persistence at 12 months post- conization was reported as 21.2%.14 In our study, this rate was 15.2% at 24 months. Similarly, a review by Hoffmann et al. demonstrated a decline in post-conization Hr-HPV persistence with longer follow-up periods.15
Fan et al. reported a recurrence rate of CIN between 7–25%, with most cases occurring within the first 2 years after conization.16 In the study by Santesso et al., the recurrence rate at 12 months was reported as 1.4%.17 In our study, the CIN 2+ recurrence rate at 24 months was 2.8%. Recurrence may result from incomplete treatment of initial lesions, ongoing Hr-HPV infection, or reinfection with a different Hr-HPV type.18,19 However, it remains uncertain whether CIN lesions detected during extended follow-up represent true recurrence of the primary disease or secondary lesions due to reinfection with a different Hr-HPV genotype.
In our study, 69.2% of patients with recurrent CIN 2+ lesions had multifocal primary lesions in either the cone specimen or surgical margin. The recurrence rate appeared higher in patients with multifocal primary CIN 2+ lesions. In a study by Allard et al., 56% of both low-grade and high-grade cervical lesions were located near the cervical os, particularly at the 6, 11, and 12 o’clock positions.20 In clinical practice, it may be challenging to apply the parameters colposcopists rely on to decide where to take biopsies. Lesions that are difficult to detect or sample during colposcopy may be missed, which is a major limitation of colposcopic biopsy in defining lesion localization.
Similarly, our study found a higher frequency of CIN 2+ lesions in the upper quadrant of the cervix, corresponding to the 11, 12, and 1 o’clock positions, in cone specimens. Since the entire cone specimen was evaluated as a whole, the localization of cervical lesions could be objectively determined. Given the cervix’s continuous microbial exposure from the vagina and the histo- physiological and immunological interplay between the cervix, vagina, and uterine cavity, lesion localization may theoretically influence disease progression in HPV-related pathologies. However, in our study, the quadrant location of high-grade lesions in the cone specimen had no prognostic impact on Hr- HPV persistence, abnormal smear results, or CIN 2+ recurrence during follow-up.
The relatively small sample size is a key limitation of our study. Guido and Schiffman previously reported no correlation between the localization of cervical preinvasive lesions detected by colposcopic biopsy and CIN grade.21 Other studies have also suggested that the distribution of high-grade lesions within the cervix has no clinical significance.22,23 These studies primarily relied on biopsy locations, which are influenced by the colposcopist’s experience and subjective assessment, introducing potential bias. In contrast, our study examined the entire cervix through cone specimens, allowing detection of lesions that might be missed by biopsy. Thus, our results are more objective and reliable. Nevertheless, the relatively small sample size and limited follow-up period remain notable limitations.
Limitations
The relatively small sample size and limited follow-up period remain notable limitations of the study.
Conclusion
In our study, no significant association was found between the quadrant localization of CIN 2+ lesions in the cone specimen and postoperative outcomes, including Hr-HPV persistence, abnormal cervical cytology, and CIN 2+ recurrence.
To the best of our knowledge, this is the first study in the literature to specifically evaluate the prognostic significance of the topographic location of primary CIN 2+ lesions. Further comprehensive studies are needed to clarify this issue and may contribute to guiding clinical practice in terms of conization technique and patient follow-up strategies.
Declarations
Ethics Declarations
The authors declare that the study was conducted in accordance with ethical principles and approved by the relevant institutional ethics committee.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all patients prior to the procedure, allowing the use of anonymized clinical data for research purposes.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: M.Ş.
Methodology: M.Ş., A.D.
Investigation: M.Ş., Ş.B.A., T.B., A.E.T.
Data curation: Ş.B.A., T.B.
Formal analysis: A.D.
Writing – original draft: M.Ş.
Writing – review & editing: M.Ş., İ.K.
Supervision: M.Ş.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing,
and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
AGC: Atypical Glandular Cells
ASC-H: Atypical Squamous Cells – cannot exclude HSIL
ASC-US: Atypical Squamous Cells of Undetermined Significance
CIN: Cervical Intraepithelial Neoplasia
Hr-HPV: High-risk Human Papillomavirus
HSIL: High-grade Squamous Intraepithelial Lesion
IFCPC: International Federation for Cervical Pathology and Colposcopy
LEEP: Loop Electrosurgical Excision Procedure
LSIL: Low-grade Squamous Intraepithelial Lesion
SD: Standard Deviation
References
-
Dalstein V, Riethmuller D, Prétet JL, et al. Persistence and load of high-risk HPV are predictors for development of high-grade cervical lesions: a longitudinal French cohort study. Int J Cancer. 2003;106(3):396-403. doi: 10.1002/ijc.11222
-
Solomon D, Davey D, Kurman R, et al. The 2001 Bethesda System: terminology for reporting results of cervical cytology. JAMA. 2002;287(16):2114–2119. doi: 10.1001/jama.287.16.2114
-
Ostör AG. Natural history of cervical intraepithelial neoplasia: a critical review. Int J Gynecol Pathol. 1993;12(2):186-192.
-
Martin-Hirsch PP, Paraskevaidis E, Bryant A, Dickinson HO, Keep SL. Surgery for cervical intraepithelial neoplasia. Cochrane Database Syst Rev. 2010;6(6):CD001318. doi: 10.1002/14651858.CD001318.pub2
-
Zielinski GD, Bais AG, Helmerhorst TJ, et al. HPV testing and monitoring of women after treatment of CIN 3: review of the literature and meta-analysis. Obstet Gynecol Surv. 2004;59(7):543–553.
-
Paraskevaidis E, Arbyn M, Sotiriadis A, et al. The role of HPV DNA testing in the follow-up period after treatment for CIN: a systematic review of the literature. Cancer Treat Rev. 2004;30(2):205–211.
-
Melnikow J, McGahan C, Sawaya GF, Ehlen T, Coldman A. Cervical intraepithelial neoplasia outcomes after treatment: long-term follow-up from the British Columbia Cohort Study. J Natl Cancer Inst. 2009;101(10):721–728. doi: 10.1093/jnci/djp089
-
Soutter WP, Sasieni P, Panoskaltsis T. Long-term risk of invasive cervical cancer after treatment of squamous cervical intraepithelial neoplasia. Int J Cancer. 2006;118(8):2048–2055.
-
Prato B, Ghelardi A, Gadducci A, et al. Correlation of recurrence rates and times with posttreatment human papillomavirus status in patients treated with loop electrosurgical excision procedure conization for cervical squamous intraepithelial lesions. Int J Gynecol Cancer. 2008;18(1):90–94. doi: 10.1111/j.1525-1438.2007.00965.x
-
Kreimer AR, Guido RS, Solomon D, et al. Human papillomavirus testing following loop electrosurgical excision procedure identifies women at risk for posttreatment cervical intraepithelial neoplasia grade 2 or 3 disease. Cancer Epidemiol Biomarkers Prev. 2006;15(5):908–914.
-
Kocken M, Helmerhorst TJ, Berkhof J, et al. Risk of recurrent high-grade cervical intraepithelial neoplasia after successful treatment: a long-term multi- cohort study. Lancet Oncol. 2011;12(5):441–450. doi: 10.1016/S1470-2045(11)70078-X
-
Perkins RB, Guido RS, Castle PE, et al. 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors. J Low Genit Tract Dis. 2020;24(2):102-31.
-
Bornstein J, Bentley J, Bösze P, et al. 2011 colposcopic terminology of the International Federation for Cervical Pathology and Colposcopy. Obstet Gynecol. 2012;120(1):166-172.
-
Baser E, Ozgu E, Erkilinc S, Togrul C, Caglar M, Güngör T. Risk factors for human papillomavirus persistence among women undergoing cold-knife conization for treatment of high-grade cervical intraepithelial neoplasia. Int J Gynecol Obstet. 2014;125(3):275–278.
-
Hoffman SR, Le T, Lockhart A, Sanusi A, Dal Santo L, Davis M. Patterns of persistent HPV infection after treatment for cervical intraepithelial neoplasia (CIN): A systematic review. Int J Cancer. 2017;141(1):8-23.
-
Fan A, Wang C, Han C, Wang Y, Xue F, Zhang L. Factors affecting residual/ recurrent cervical intraepithelial neoplasia after cervical conization with negative margins. J Med Virol. 2018;90(9):1541-1548.
-
Santesso N, Mustafa RA, Wiercioch W, Kehar R, Gandhi S, Chen Y. Systematic reviews and meta-analyses of benefits and harms of cryotherapy, LEEP, and cold knife conization to treat cervical intraepithelial neoplasia. Int J Gynaecol Obstet. 2016;132(3):266-271.
-
Tachezy R, Mikysková I, Ludvíková V, Rob L, Kucera T, Slavik V. Longitudinal study of patients after surgical treatment for cervical lesions: detection of HPV DNA and prevalence of HPV-specific antibodies. Eur J Clin Microbiol Infect Dis. 2006;25(8):492–500.
-
Bollen LJ, Tjong-A-Hung SP, van der Velden J, Mol BW, ten Kate FW. Prediction of recurrent and residual cervical dysplasia by human papillomavirus detection among patients with abnormal cytology. Gynecol Oncol. 1999;72(2):199–201.
-
Allard, J. E., Rodriguez, M., Rocca, M., Parker, M. F. Biopsy site selection during colposcopy and distribution of cervical intraepithelial neoplasia. J Low Genit Tract Dis. 2005;9(1):36–39.
-
Guido RS, Jeronimo J, Schiffman M, Solomon D; ALTS Group. The distribution of neoplasia arising on the cervix: results from the ALTS trial. Am J Obstet Gynecol. 2005;193(4):1331-1337.
-
Reid R, Greenberg M, Jenson AB, Husain M, Willett J, Daoud Y. Sexually transmitted papillomaviral infections. I. The anatomic distribution and pathologic grade of neoplastic lesions associated with different viral types. Am J Obstet Gynecol. 1987;156(1):212–222.
-
Autier P, Coibion M, Huet F, Grivegnee AR. Transformation zone location and intraepithelial neoplasia of the cervix uteri. Br J Cancer. 1996;74(3):488–490.
Tables
Table 1. Demographic and clinicopathological characteristics of the patients
n: Number of patients; SD: Standard deviation 1: n=346 patients (Data was not available in 115 patients) 2: n=362 patients (Data was not available in 99 patients) 3 : Endocervical curettage in colposcopy 4 : Endocervical curettage in conization AS-CUS: Atypical Squamous Cells of Undetermined Significance; LSIL: Low Grade Squamous Intraepithelial Lesion; HSIL: High Grade Squamous Intraepithelial Lesion; AGC: Atypical Glandular Cell; ASC-H: Atypical Squamous Cells, not excluding HSIL; CIN: Cervical Intraepithelial Neoplasia
Table 2. Histopathological findings 12 months after conization
n: Number of patients; SD: Standard deviation AS-CUS: Atypical Squamous Cells of Undetermined Significance; LSIL: Low Grade Squamous Intraepithelial Lesion; HSIL: High Grade Squamous Intraepithelial Lesion; AGC: Atypical Glandular Cell; ASC-H: Atypical Squamous Cells, not excluding HSIL; CIN: Cervical Intraepithelial Neoplasia
Table 3. Localization patterns and cervical quadrant distribution of CIN 2+ lesions in cone specimens and surgical margins in patients with Hr-HPV persistence, abnormal cervical cytology, and CIN 2+ lesion recurrence after conization
1: Conization specimen Chi-square test; x2 and Fisher’s exact test; p: Significance value: 0.05
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mustafa Şahin, Şeyma Banu Arslanca, Adem Doğaner, Tuba Bıyık, Arife Ebru Taşçı, İlknur Küçükosmanoğlu. The Impact of Topographic Localization of CIN 2-3 Lesions in Conization Specimens on Disease Progression: A Retrospective Study. Ann Clin Anal Med 2026;17(Suppl 2):S124-129. doi: 10.4328/ACAM.22688
- Received:
- April 7, 2025
- Accepted:
- May 19, 2025
- Published Online:
- June 26, 2025