
Diaphragmatic hernias requiring emergency surgery: a retrospective analysis
Emergency repair of diaphragmatic hernias
Authors
Abstract
Aim Diaphragmatic hernias can originate from the esophageal hiatus, congenital defects, or traumatic defects of the diaphragm caused by penetrating or blunt trauma of the thoracoabdominal region. This retrospective analysis aims to examine cases of diaphragmatic hernia that were operated on as surgical emergencies in our hospital.
Methods Medical records of all the patients who underwent diaphragmatic hernia repair in the General Surgery Clinic of Istanbul Training and Research Hospital between 2005 and 2019 were examined. Cases operated under emergency conditions were selected for detailed analysis.
Results Cases requiring urgent intervention constituted 25% of all diaphragmatic hernia repairs. The mean age of the patients was 54.1 (18-93) years. Ten patients (52.6%) were male and 9 (47.4%) were female; 1 patient was a male infant. Among hernias requiring emergency intervention, 8 patients (42.1%) were operated on because of obstructive symptoms, while 6 (31.6%) others were operated on because of signs of strangulation. Organ perforation was present in 4 patients (21.1%). One patient (5.3%) was operated on for severe respiratory distress. One male infant was operated on for sliding hernia of the stomach into the mediastinum and causing respiratory distress.
The mean hospital stay was 14.7 days in the adult group, while the duration of hospitalization of the infant was 21 days.
In the postoperative period, wound dehiscence in 2 patients, subcutaneous hemorrhage in 2 patients, and ileoileal intussusception in an infant patient developed. One patient was re-hospitalized for respiratory distress after discharge. The patient failed to respond to treatment and died on postoperative day 21.
Conclusion Diaphragmatic hernias in all ages can be true surgical emergencies that require immediate action, especially in the presence of respiratory distress, strangulation, and perforation.
Keywords
Introduction
Diaphragmatic hernias can originate from the esophageal hiatus (sliding and paraesophageal hernias), congenital defects (Bochdalek hernias originating from the posterolateral area of the diaphragm and Morgagni-Larrey hernias located parasternally on both sides). Moreover, penetrating thoracoabdominal injuries can cause traumatic defects that might eventually progress to diaphragmatic hernias.1,2
The incidence of hiatal hernias in the population has been reported to be 10 to 50%.3 In sliding type hernia, surgical intervention is reserved for symptomatic cases and those with Barrett’s metaplasia. Emergency intervention for sliding type hernia is rarely needed. In paraesophageal hernias, however, surgery is indicated as soon as the diagnosis is made because of the risk of strangulation.
Congenital hernias are extremely rare in the adult population, as they are usually diagnosed in the neonatal period.4, 5 Congenital diaphragmatic hernias are usually asymptomatic in adulthood, while symptomatic cases usually present with dyspeptic complaints. This type of disease, which is managed mostly in elective conditions, can also present as emergency situations more frequently than anticipated. Serious complications that require urgent intervention, such as strangulation and obstruction, are likely to develop. In such emergency cases, unusual and life-threatening scenarios might unfold.
With diaphragmatic defects secondary to trauma, the patient can remain asymptomatic for years. The risks for complications such as strangulation or perforation of hollow viscera due to herniation over the course of the lifetime are well established, and therefore, when detected, surgical repair of the defect is mandatory. Thus, evaluation of the diaphragm is required, especially if penetrating trauma involves the thoracoabdominal region.
This retrospective analysis aims to examine cases of diaphragmatic hernia that were operated on as surgical emergencies in our hospital.
Materials and Methods
Medical records of all the patients who underwent diaphragmatic hernia repair in the General Surgery Clinic of Istanbul Training and Research Hospital between 2005 and 2019 were examined. Cases operated under emergency conditions were selected for detailed analysis. Data regarding age, gender, presenting symptoms, type of hernia, surgical procedures, length of hospital stay, postoperative complications, and mortality were recorded. An emergency case of pediatric diaphragmatic hernia operated on by the pediatric surgeon in our hospital was also included in the analysis.
This study was approved by the Ethics Committee of İstanbul Training and Research Hospital (Date: 2020-05-15, No: 2310)
Ethics ApprovalThis retrospective study was approved by the Ethics Committee of İstanbul Training and Research Hospital (Date: 2020-05-15, No: 2310). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Statistical AnalysisDescriptive statistical analysis was performed. Continuous variables were expressed as mean (range), and categorical variables as numbers and percentages.
Reporting GuidelinesThis study was reported in accordance with the STROBE guidelines.
Results
Between 2005 and 2017, 80 patients were operated on for various types of diaphragmatic hernia in our institution’s general surgery clinic. 20 of these patients had emergency surgery because of acute symptoms and complications caused by diaphragmatic hernia. Cases requiring urgent intervention constituted 25% of all diaphragmatic hernia repairs.
The mean age of the patients was 54.1 (18-93) years (the newborn patient is not included in the mean). Ten patients (52.6%) were male and 9 (47.4%) were female; 1 patient was a male infant.
Seven patients (35%) had diaphragmatic hernia secondary to trauma, 6 patients (30%) had congenital hernia (Morgagni’s hernia in 5 patients and Bochdalek hernia in 1 patient) and 7 patients (35%) had hiatus hernia (paraesophageal hernia in 6 patients and sliding hernia in 1 patient) (Figure 1). Two patients had a history of prior diaphragmatic hernia repair surgery but had relapsed. One of these patients had been operated on for hiatus hernia and was re-operated because of a paraesophageal hernia in the same location, causing perforation of the stomach. The other had been operated for traumatic rupture of the diaphragm, and the colon had herniated into the thorax from the recurrent defect, causing obstruction.
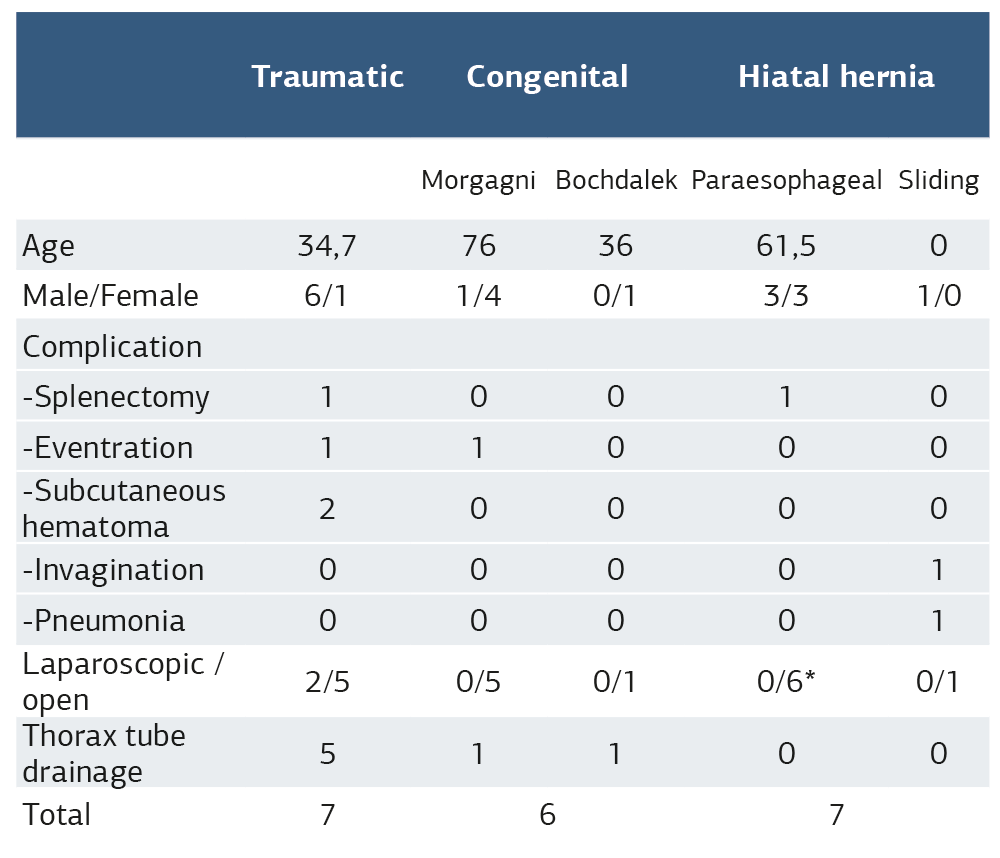
Among hernias requiring emergency intervention, 8 patients (42.1%) were operated on because of obstructive symptoms, while 6 (31.6%) others were operated on because of signs of strangulation (Figure 2). Organ perforation was present in 4 patients (21.1%) (stomach perforation in 2 patients and colon perforation in 2 patients). One patient (5.3%) was operated on for severe respiratory distress due to herniation of intraabdominal organs into the thorax from the defect caused by traumatic rupture of the diaphragm. One male infant diagnosed by contrast-enhanced tomography while being tested for respiratory distress in the second week after birth, was operated for sliding hernia of the stomach into the mediastinum and causing respiratory distress (Figure 3). General characteristics of the cases are presented in Table 1.
During surgery, herniated organs were reduced back into the abdominal cavity. Inside the hernia sac were the stomach in 13 patients, the colon in 8 patients, the omentum in 5 patients, and the intestines in 1 patient. In 7 cases, more than one organ was present in the hernia sac.
The operation was completed by the laparoscopic approach in 2 patients. In one patient, the presence of adhesions necessitated conversion to open surgery. The remaining 17 patients were operated on by open surgery. Mesh repair was performed in all patients with Morgagni’s hernia, whereas primary repair and fundoplication were the preferred methods for the patient with Bochdalek hernia. Among patients operated for traumatic diaphragmatic hernia, primary repair of the hernia defect was performed in all but one patient, for whom a synthetic mesh was also used. In addition to diaphragmatic cruroplasty, half of the patients with paraesophageal hernia underwent fundoplication. The surgical procedure used for the infant with sliding hernia consisted of diaphragmatic crus repair and Thal’s anti-reflux procedure.
Of the patients with organ perforation, 2 stomach perforations with paraesophageal hernia were repaired by primary suturing and omentoplasty following debridement of the wound edges. The perforated transverse colon of a patient with traumatic hernia was exteriorized by a loop colostomy. The micro-perforation caused by the reduction of the herniated colon in one patient was repaired by primary suturing because of a lack of contamination.
Tube thoracostomy was placed during the operation on 7 patients because of opening of the thoracic cavity. One of these patients had Morgagni’s hernia, 1 had Bochdalek hernia, while the other 5 were operated on for diaphragmatic hernia secondary to trauma. Splenectomy was also performed in 2 cases due to iatrogenic laceration of the spleen. In the postoperative period, wound dehiscence in 2 patients and subcutaneous hemorrhage in 2 patients were observed. On the third postoperative day of the infant with sliding hernia, ileoileal intussusception developed. He was operated on again for manual reduction of the invaginated segment. The subsequent right upper lobe pneumonia was treated medically, and the patient was discharged.
The mean hospital stay was 14.7 days in the adult group, while the duration of hospitalization of the infant was 21 days.
The overall frequency of intraoperative and postoperative morbidity of the 20 patients was 40%. The overall frequency of intraoperative and postoperative morbidity of the 20 patients was 40%. No surgery-related mortality was observed. However, one patient died on postoperative day 21 due to exacerbation of preexisting chronic obstructive pulmonary disease (COPD). One patient presented with respiratory distress after discharge, on postoperative day 13. He was hospitalized, and treatment for the exacerbation of his preexisting chronic obstructive pulmonary disease (COPD) was initiated by the pulmonology department. The patient failed to respond to treatment and died on postoperative day 21 because of COPD.
Discussion
Hiatal hernias consist of sliding hernias, which are usually asymptomatic or with gastroesophageal reflux (GER) symptoms, and paraesophageal hernias, which might cause a broad range of complications from distention of the stomach to strangulation. Surgery is not indicated for sliding hernias without complications, however, it might be considered if GER significantly affects the quality of life or if Barrett’s metaplasia has developed. No cases of sliding hernia were present among our adult patients; only one case requiring emergency surgery by a pediatric surgeon was included in the series. Although they can be asymptomatic, pediatric patients with hiatal hernia usually present with symptoms such as GER, respiratory tract infection and growth retardation.6 The infant in our series presented with respiratory distress caused by the dislocation of the intestines into the thorax. The subsequent upper lobe pneumonia was most likely a complication of GER. As in adults, sliding hernias in children often do not have any symptoms but occasionally, vomiting due to GER, respiratory distress or growth retardation are present.7
Paraesophageal hernias constitute only 14% of hiatal hernias.8 While the main principles of surgery are the reduction of the herniated organs back into the abdomen and crural repair, the addition of fundoplication to the procedure has an important role as well.3 One study has demonstrated that the determinants of success in surgery are the complete resection of the hernia sac, meticulous intrathoracic dissection of the esophagus, and repair of the crura.9 Unlike sliding hernias, diagnosis of the pathology is sufficient indication for the surgical treatment of paraesophageal hernias since complications such as strangulation, intestinal obstruction, and perforation are common in this group.10 The fact that all 6 of our adult hiatal hernia cases are paraesophageal hernias, despite the relatively low frequency, supports the validity of this approach. Stomach perforation in two of our cases with paraesophageal hernia is further proof of the high risk of complications in these patients. The use of synthetic mesh in the treatment of paraesophageal hernias is common. However, we did not use meshes in any of our paraesophageal hernia cases. The existence of perforation is another reason to avoid mesh placement, as the use of synthetic materials in infected sites is not recommended. Fundoplication was performed in half of these cases. No difference in outcome was observed, although it might be related to the small sample size. Thal’s anti-reflux procedure was performed for the infant patient. Thal’s is a partial wrapping procedure. It is commonly used in pediatric surgery as it is a relatively simple and safe procedure with low rates of perioperative complications and good long-term outcomes.11
Although rare in the adult population, surgical treatment for congenital hernias is recommended as they can have severe complications if not treated. There are not enough studies to determine the optimal surgical procedure, but the use of mesh for reinforcement is a widely accepted method.4 All but one of our cases had mesh repair, of which we did not observe any drawbacks. Very rarely, congenital and hiatal hernias can coexist. The recommended treatment is fundoplication and the use of mesh to repair both defects in the same operation.12 Our case with Bochdalek’s hernia was such a case, also containing sliding hiatal hernia. Primary repair of the diaphragmatic defect, as well as cruroplasty and fundoplication, was performed in the operation of this patient.
Trauma and iatrogenic diaphragmatic injuries are also major causes of diaphragmatic hernias. Trauma is an important factor in the development of diaphragmatic hernias; both penetrating and blunt trauma can cause rupture of the diaphragm. Rupture of the diaphragm can occur in 0.8% to 15% of all thoracoabdominal traumas.13 Early diagnosis through a high index of suspicion for diaphragmatic injury is necessary.14 Laparoscopic exploration after trauma of the thoracoabdominal region can detect injury to the diaphragm, allowing prevention of long-term complications. Therefore, acute detection of the problems is essential in avoiding chronic complications. Severe complications such as strangulation or perforation of hollow viscera can develop after undiagnosed diaphragmatic injuries.15,16
Timely diagnosis is of paramount importance as morbidity is much higher in complicated cases requiring emergency surgery compared to hernias diagnosed early and repaired under elective circumstances.17
Life-threatening conditions, such as perforation of hollow viscera, are frequently seen in complicated diaphragmatic hernias. In our series, the rate of such cases was 21.1%. As they can cause obstruction, strangulation, or perforation, paraesophageal and congenital hernias should be operated on under elective conditions shortly after diagnosis. Regarding the surgical approach, laparoscopy is increasingly popular in parallel with the increasing experience in laparoscopic surgery in general. Shorter length of hospital stay, better quality of life, less postoperative pain, and cosmetic concerns influence the preferences of the surgeons in favor of the minimally invasive approach. On the other hand, for emergency surgery in the presence of strangulation, tissue necrosis, or perforation, the open approach appears to be safer for both the patient and the surgeon. In our series, only 3 patients were operated laparoscopically, 2 completed as such, and 1 converted to open surgery. All 3 cases were operated on because of obstruction. Further studies comparing laparoscopic and open surgery in urgent cases of diaphragmatic hernias are needed. In one study about paraesophageal hernias, 50% of the conversions from laparoscopic to open were emergency cases. On the other hand, only 30% of all emergency cases were operated on with open surgery.9 One can conclude that laparoscopy will gain popularity in time. The surgeon should consider their experience, the status of the patient, the operative team, and available equipment in determining the surgical method. It should not be forgotten that for these types of diaphragmatic hernias, emergency surgery has high risks of morbidity and mortality; open surgery in many cases might provide more confidence.
The status of the patient is a major predictor of progress in the postoperative period. Possible complications can affect the abdomen, the thorax, or the mediastinum. Even after a successful operation, the progress might evolve into undesirable outcomes. One of our patients with COPD died of respiratory failure in the early postoperative period despite a successful and uncomplicated operation.
The infant had abdominal distention and bile in the nasogastric tube 3 days after the operation. Abdominal ultrasonography revealed an ileoileal postoperative intussusception of 3.5 cm length, which was corrected by manual reduction through laparotomy. In the postoperative period, pneumonia of the left lung was added to the clinical picture. After 18 days of inpatient treatment, the patient was discharged. Various complications have been reported following diaphragmatic hernia surgery, including dysphagia, recurrence, pneumonia, intestinal obstruction, intussusception, hemorrhage, surgical site infections, and gastroparesis.6,18 In pediatric patients, postoperative ileoileal intussusception typically occurs following retroperitoneal and prolonged abdominal operations.19
Thanks to modern imaging modalities such as computerized tomography (CT) and magnetic resonance imaging (MRI), all types of diaphragmatic hernia can be diagnosed with very high accuracy. Computerized tomography with coronal and sagittal sections is the most efficient diagnostic method in many cases of diaphragmatic hernia, as it clearly reveals the herniated organs and existing complications. In selected cases, MRI can be used for diagnosis, especially if CT is not conclusive.20 For all of our patients, the main diagnostic tests were CT or MRI, chest and abdominal X-rays, as well as blood tests were complementary tools. In order to differentiate the air-filled structure in the mediastinum from hiatal hernia and congenital bronchogenic cyst, a control thorax CT with oral contrast was needed in the infant patient.
Tube thoracostomy is required in the case of opening of the thoracic cavity; in 7 of our patients, thorax tube placement was needed. Iatrogenic opening of the thoracic cavity usually occurs during excision of the hernia sac. Some authors have therefore recommended against excision of the hernia sac in congenital hernias.21 In traumatic hernias, opening of the thoracic cavity is much more common due to the trauma itself. Although tube thoracostomy significantly impairs patient comfort, it is a mandatory procedure that also provides a sense of safety for both the patient and the surgeon. According to our findings, diaphragmatic hernias requiring emergency surgery can have severe consequences. They are true surgical emergencies that require immediate action, especially in the presence of strangulation and perforation.
Limitations
Our limiting factors were the small number of cases and the retrospective nature of the study.
Conclusion
Diaphragmatic hernias requiring emergency surgery can have severe consequences. They are true surgical emergencies that require immediate action, especially in the presence of strangulation and perforation.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of İstanbul Training and Research Hospital (Date: 2020-05-15, No: 2310).
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was waived by the Ethics Committee due to the retrospective design of the study and the use of anonymized patient data.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: E.Ş.
Methodology: M.Y.
Formal Analysis: S.A.
Investigation: S.A.
Data Curation: E.Ş.
Writing – Original Draft Preparation: E.Ş.
Writing – Review & Editing: M.Y., M.B.D.
Validation: M.B.D.
Supervision: M.Y., M.B.D.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
COPD: Chronic Obstructive Pulmonary Disease
CT: Computed Tomography
GER: Gastroesophageal Reflux
MRI: Magnetic Resonance Imaging
References
-
Crandall M, Popowich D, Shapiro M, West M. Posttraumatic hernias: historical overview and review of the literature. Am Surg. 2007;73(9):845-850.
-
Hanna WC, Ferri LE. Acute traumatic diaphragmatic injury. Thorac Surg Clin. 2009;19(4):485-489.
-
Dean C, Etienne D, Carpentier B, Gielecki J, Tubbs RS, Loukas M. Hiatal hernias. Surg Radiol Anat. 2012;34(4):291-299.
-
Ryan JM, Rogers AC, Hannan EJ, Mastrosimone A, Arumugasamy M. Technical description of laparoscopic Morgagni hernia repair with primary closure and only composite mesh placement. Hernia. 2018;22(4):697-705.
-
Moro K, Kawahara M, Muneoka Y, et al. Right-sided Bochdalek hernia in an elderly adult: a case report with a review of surgical management. Surg Case Rep. 2017;3(1):109.
-
Garvey EM, Ostlie DJ. Hiatal and paraesophageal hernia repair in pediatric patients. Semin Pediatr Surg. 2017;26(2):61-66.
-
Jang WN, Park IS, Park KW, Yoo SY, Lee J, Cho SH. A case of congenital paraesophageal hiatal hernia in infancy. Pediatr Gastroenterol Hepatol Nutr. 2012;15(2):100-104. 10.5223/pghn.2012.15.2.100
-
Hashemi M, Sillin LF, Peters JH. Current concepts in the management of paraesophageal hiatal hernia. J Clin Gastroenterol. 1999;29(1):8-13.
-
Latzko M, Borao F, Squillaro A, Mansson J, Barker W, Baker T. Laparoscopic repair of paraesophageal hernias. JSLS. 2014;18(3):e2014.00009. doi:10.4293/JSLS.2014.00009
-
Hill LD. Incarcerated paraesophageal hernia: a surgical emergency. Am J Surg. 1973;126(2):286-289.
-
Namgoong JM, Kim DY, Kim SC, Hwang JH. Hiatal hernia in pediatric patients: laparoscopic versus open approaches. Ann Surg Treat Res. 2014;86(5):264-269. doi:10.4174/astr.2014.86.5.264
-
Mittal A, Pardasani M, Baral S, Thakur S. A rare case report of Morgagni hernia with organo-axial gastric volvulus and concomitant para-esophageal hernia, repaired laparoscopically in a septuagenarian. Int J Surg Case Rep. 2018;45:45-50.
-
Thiam O, Konate I, Gueye ML, et al. Traumatic diaphragmatic injuries: epidemiological, diagnostic and therapeutic aspects. Springerplus. 2016;5(1):1614.
-
Lu J, Wang B, Che X, et al. Delayed traumatic diaphragmatic hernia: a case-series report and literature review. Medicine (Baltimore). 2016;95(32):e4362. doi:10.1097/MD.0000000000004362
-
Kumar A, Bagaria D, Ratan A, Gupta A. Missed diaphragmatic injury after blunt trauma presenting with colonic strangulation: a rare scenario. BMJ Case Rep. 2017;2017:bcr2017221220. doi:10.1136/bcr-2017-221220
-
Zhao H, Gao R, Jia D, Li A. Delayed traumatic parasternal hernia causes jejunal necrosis: a case report. Trauma Case Rep. 2017;9:30-33.
-
Raakow J, Schulte-Mäter J, Andreou A, Biebl M, Pratschke J. Diaphragmatic herniation of abdominal contents: case series and review of the literature. Zentralbl Chir. 2017;142(1):113-121.
-
Spitz L, Kirtane J. Results and complications of surgery for gastro-oesophageal reflux. Arch Dis Child. 1985;60(8):743-747. doi:10.1136/adc.60.8.743
-
Klein JD, Turner CG, Kamran SC, et al. Pediatric postoperative intussusception in the minimally invasive surgery era: a 13-year, single-center experience. J Am Coll Surg. 2013;216(6):1089-1093.
-
Eren S, Ciriş F. Diaphragmatic hernia: diagnostic approaches with review of the literature. Eur J Radiol. 2005;54(3):448-459.
-
Kuster GG, Kline LE, Garzo G. Diaphragmatic hernia through the foramen of Morgagni: laparoscopic repair case report. J Laparoendosc Surg. 1992;2(2):93-100. doi:10.1089/lps.1992.2.93
Figures
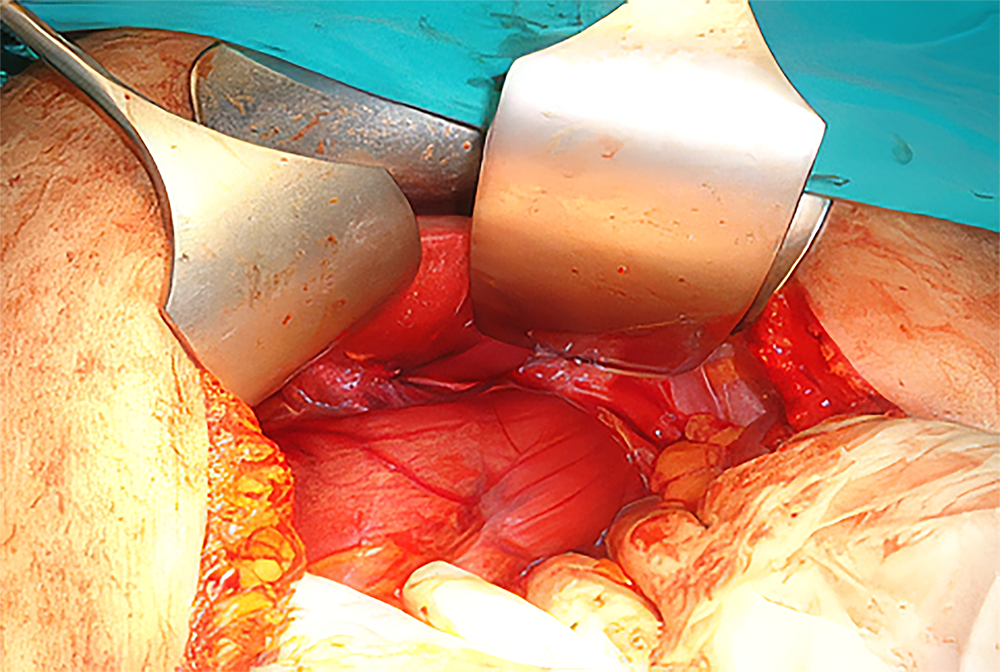
Figure 1. Incarcerated stomach within a paraesophageal hernia
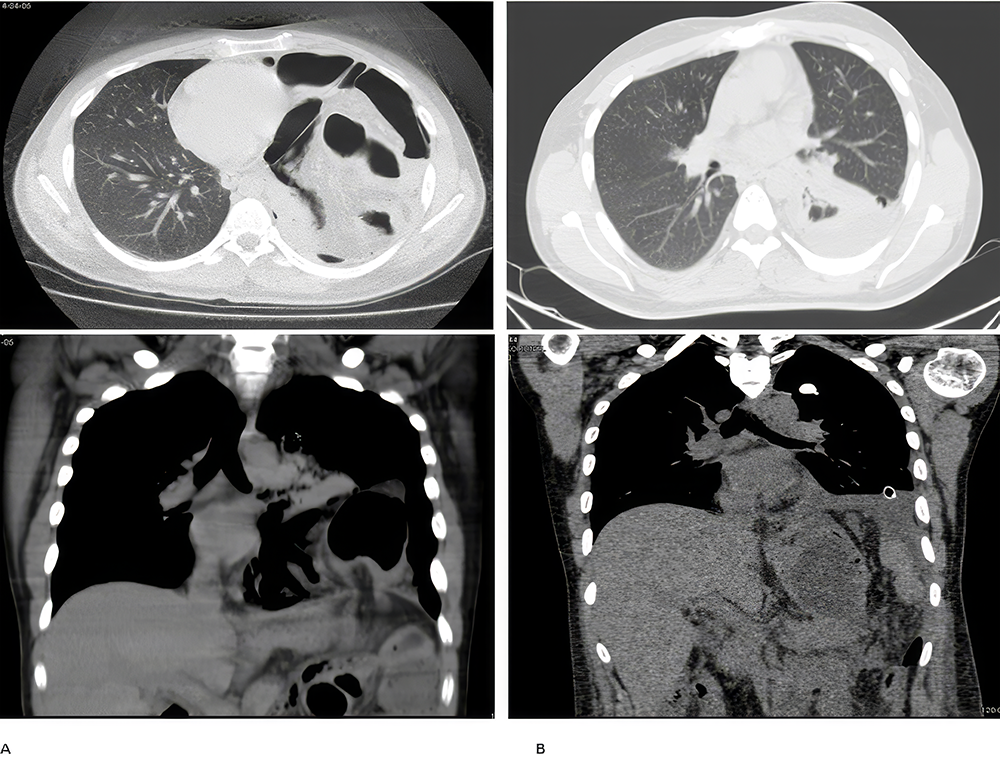
Figure 2. A: Strangulated colon within the diaphragmatic hernia secondary to a previous gunshot wound B: On postoperative day 5. Thorax tube and foreign body in the left lung, pleurisy, and partial atelectasis
Tables
Table 1. General characteristics of the cases
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Esin Şair, Mehmet Yazıcı, Soykan Arıkan, Mehmet Baki Dogan. Diaphragmatic hernias requiring emergency surgery: a retrospective analysis. Ann Clin Anal Med 2026;17(Suppl 1):S34-38
- Received:
- April 8, 2025
- Accepted:
- June 16, 2025
- Published Online:
- June 22, 2025