
Prognostic significance of clinical and laboratory parameters in pediatric intensive care sepsis: a retrospective cohort study
Biomarkers and mortality in pediatric sepsis
Authors
Abstract
Aim Sepsis is a major cause of morbidity and mortality among critically ill pediatric patients. Early identification of high-risk individuals through clinical and biochemical markers may improve patient outcomes. This study aimed to investigate the relationship between early clinical and laboratory parameters and mortality in children diagnosed with sepsis in a pediatric intensive care unit (PICU).
Methods This single-center, retrospective cohort study included 128 pediatric patients diagnosed with sepsis and admitted to the PICU of Gaziantep City Hospital between January 2024 and January 2025. Demographic, clinical, and laboratory data were recorded within the first 24 hours of admission. Survivors and non-survivors were compared, and logistic regression and ROC analyses were performed to identify independent predictors of mortality.
Results Of the 128 patients, 95 (74.2%) survived and 33 (25.8%) died. Non-survivors had significantly higher levels of lactate (4.30 ± 3.30 vs. 2.88 ± 2.23 mmol/L, p = 0.017), ferritin (940 ± 450 vs. 480 ± 320 ng/mL, p = 0.008), total and direct bilirubin, and lower bicarbonate and base excess levels (p < 0.05 for all). In multivariate logistic regression, lactate (OR = 1.21, p = 0.039), ferritin (OR = 1.20, p = 0.009), bicarbonate (OR = 2.16, p = 0.011), and base excess (OR = 0.51, p = 0.006) were identified as independent predictors of mortality. ROC analysis demonstrated acceptable discriminative ability for all four parameters (AUC range: 0.659–0.740).
Conclusion Elevated lactate and ferritin levels and decreased bicarbonate and base excess values were independently associated with mortality in pediatric sepsis. These commonly available biomarkers may provide valuable prognostic insight and help guide early clinical decision-making in the intensive care setting.
Keywords
Introduction
Sepsis remains one of the leading causes of morbidity and mortality among critically ill children admitted to pediatric intensive care units (PICUs) worldwide. Characterized by a dysregulated host response to infection, pediatric sepsis can rapidly progress to septic shock, multiorgan dysfunction, and death if not promptly diagnosed and treated.1,2 The early identification of high-risk patients is a cornerstone of effective clinical management, as it directly influences the timing of interventions and the allocation of intensive care resources.3
Despite significant advances in intensive care medicine, the heterogeneity of clinical presentations and the lack of universally accepted pediatric-specific diagnostic criteria continue to challenge early recognition of sepsis in children.4,5 Unlike in adults, where several risk stratification tools exist (e.g., SOFA, APACHE II), pediatric sepsis lacks validated biomarkers and clinical predictors to reliably predict poor outcomes, including mortality.6
Recent studies have focused on evaluating the prognostic significance of various laboratory parameters such as C-reactive protein (CRP), procalcitonin, ferritin, lactate, and albumin in pediatric sepsis.7,8,9 Elevated lactate levels, for instance, have been associated with impaired tissue perfusion and increased mortality, while hypoalbuminemia may reflect the severity of systemic inflammation and capillary leak syndrome.8,10 Similarly, high levels of procalcitonin and ferritin are frequently observed in patients with severe sepsis or septic shock, suggesting their potential utility in risk stratification.11,12,13
The present study aims to identify clinical and laboratory predictors of mortality in pediatric patients diagnosed with sepsis and admitted to a tertiary PICU. By analyzing retrospective data, we aim to determine which early biomarkers are most strongly associated with poor outcomes and whether they can aid in distinguishing high-risk patients during the initial stages of intensive care.
This study was designed as a retrospective cohort analysis to evaluate early predictors of mortality in pediatric sepsis.
Materials and Methods
Study Design and SettingThis retrospective cohort study was conducted at the Pediatric Intensive Care Unit (PICU) of Gaziantep City Hospital, a tertiary care center located in southeastern Türkiye. The study included pediatric patients (aged 0–18 years) who were admitted to the PICU with a diagnosis of sepsis between January 2024 and January 2025. The diagnosis of sepsis was based on clinical criteria in accordance with international pediatric sepsis guidelines.14
A total of 128 patients with a confirmed diagnosis of sepsis were included. Patients with incomplete medical records or those transferred to other institutions during treatment were excluded from the analysis. The study cohort was divided into two groups based on the clinical outcome: patients who survived (n = 95) and those who died during their PICU stay (n = 33).
Data CollectionDemographic data (age, gender), clinical information (length of stay in PICU, presence of comorbidities), and laboratory parameters obtained within the first 24 hours of admission were retrospectively retrieved from the hospital’s electronic medical record system. The laboratory variables included:
- Inflammatory markers: C-reactive protein (CRP) (mg/L), procalcitonin, ferritin (ng/mL)
- Metabolic and perfusion parameters: lactate, bicarbonate, base excess
- Organ function markers: blood urea nitrogen (BUN), creatinine, uric acid, alanine aminotransferase (ALT), aspartate aminotransferase (AST), total and direct bilirubin, lactate dehydrogenase (LDH), total protein, albumin (g/dL).
- Hematological parameters: hemoglobin, hematocrit, lymphocyte and neutrophil count, platelet count
- Acid–base and gas values: pH, bicarbonate, base excess
- Coagulation and acute phase reactants: fibrinogen
Outcome MeasureThe primary outcome of the study was all-cause mortality during PICU stay. The relationship between mortality and the above parameters was assessed.
Ethics ApprovalThe study was approved by the Ethics Committee of Gaziantep City Hospital Non-Interventional Clinical Research (Date: 2025-06-18, No: 218/2025)
Statistical AnalysisAll statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA), and a p-value of < 0.05 was considered statistically significant. Descriptive statistics were used to summarize the demographic and clinical characteristics. Continuous variables were expressed as mean ± standard deviation (SD), and categorical variables as frequencies and percentages. The normality of distribution was assessed using the Kolmogorov-Smirnov test. Group comparisons were made using the Mann-Whitney U test or independent t-test as appropriate. Categorical variables were compared using the chi-square test. Spearman correlation analysis was performed to evaluate the relationship between mortality and laboratory parameters. Before performing logistic regression analysis, multicollinearity among independent variables was assessed using the variance inflation factor (VIF) values. Variables with VIF > 5 were excluded from the model. Variables found to be significant in univariate analyses were included in a multivariate logistic regression model to identify independent predictors of mortality. Receiver operating characteristic (ROC) curve analysis was used to determine the cut-off values, sensitivity, specificity, and area under the curve (AUC) of significant biomarkers.
Reporting GuidelinesThis study was conducted and reported in accordance with the STROBE guidelines for observational studies.
Results
Comparison of Clinical and Laboratory Parameters Between Survivors and Non-survivors was shown in Table 1. A total of 128 pediatric patients diagnosed with sepsis were included in the study, of whom 33 (25.8%) died during their PICU stay and 95 (74.2%) survived. There were no significant differences in age (p = 0.872) or gender distribution between the groups. The duration of PICU stay was significantly longer in survivors than in non-survivors (43.48 ± 59.95 vs. 29.82 ± 66.29 days, p = 0.002). Among laboratory parameters, non-survivors exhibited significantly higher lactate levels (4.30 ± 3.30 vs. 2.88 ± 2.23 mmol/L, p = 0.017), LDH (763.21 ± 686.75 vs. 634.43 ± 830.09 U/L, p = 0.035), total bilirubin (1.56 ± 2.49 vs. 1.05 ± 2.52 mg/dL, p = 0.005), and direct bilirubin (0.68 ± 1.32 vs. 0.42 ± 1.38 mg/dL, p = 0.005). Bicarbonate levels (20.20 ± 6.73 vs. 22.81 ± 5.83 mmol/L, p = 0.031) and base excess (−5.54 ± 8.91 vs. −1.63 ± 7.20 mmol/L, p = 0.017) were significantly lower in the non-survivor group. Additionally, ferritin levels were notably elevated in non-survivors (940 ± 450 vs. 480 ± 320 ng/mL, p = 0.008). The presence of comorbidities was more frequent among non-survivors compared to survivors (69.7% vs. 52.6%, p = 0.041). Other parameters, including CRP, procalcitonin, and albumin, did not differ significantly between the groups.
Among the survivors, the most frequently observed comorbid conditions included epilepsy (8.4%), hydrocephalus (6.3%), traffic accident-related trauma (4.2%), immunodeficiency (4.2%), pleural effusion (3.2%), cerebral palsy (3.2%), and malignant brain neoplasms (3.2%). In addition, diseases such as acute myocarditis, sphingolipidosis, cardiomyopathy, gastrointestinal bleeding, acute renal failure, and atrial septal defect were each reported in approximately 2% of the cases. Notably, 21.1% of the survivor group had various other comorbidities that were each reported only once.
In the non-survivor group, the most commonly reported comorbidity was acute renal failure (18.2%), followed by hydrocephalus (15.2%), epilepsy (9.1%), heart failure (9.1%), liver failure (6.1%), and cerebral palsy (6.1%). Furthermore, 30.3% of non-survivors had a range of other conditions that were each observed in only one patient. A correlation analysis was performed to investigate the relationship between mortality and various clinical and laboratory parameters. A significant negative correlation was observed between PICU length of stay and mortality (r = −0.275, p = 0.001), suggesting that shorter ICU stays were associated with higher mortality. In contrast, positive correlations with mortality were found for direct bilirubin (r = 0.251, p = 0.004), total bilirubin (r = 0.250, p = 0.004), lactate (r = 0.213, p = 0.016), LDH (r = 0.187, p = 0.034), and ferritin (r = 0.585, p = 0.018), indicating that increases in these parameters were significantly associated with higher mortality risk.
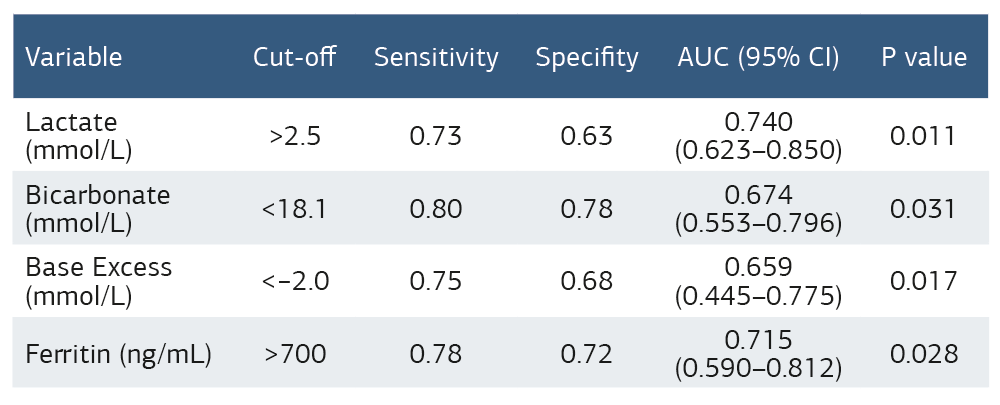
Furthermore, base excess (r = −0.213, p = 0.015) and bicarbonate (r = −0.192, p = 0.030) showed significant negative correlations with mortality, highlighting their potential as prognostic indicators. No statistically significant correlation was found for CRP, procalcitonin, albumin, or other common inflammatory and hematological markers.Multivariate logistic regression analysis was conducted to identify independent predictors of mortality in pediatric sepsis patients (Table 2). Among the variables included in the model, lactate (OR = 1.21, 95% CI: 1.00–1.47, p = 0.039), bicarbonate (OR = 2.16, 95% CI: 1.19–3.95, p = 0.011), base excess (OR = 0.51, 95% CI: 0.32–0.83, p = 0.006), and ferritin (OR = 1.20, 95% CI: 1.01–1.31, p = 0.009) were found to be statistically significant predictors of mortality (Table 2.). Receiver operating characteristic (ROC) curve analysis was performed to evaluate the diagnostic performance of significant biomarkers in predicting mortality (Table 3). Among the tested parameters, lactate demonstrated an optimal cut-off value of >2.5 mmol/L, with a sensitivity of 73% and specificity of 63% (AUC = 0.740, 95% CI: 0.623–0.850, p = 0.011). Bicarbonate levels below 18.1 mmol/L yielded a sensitivity of 80% and specificity of 78% (AUC = 0.674, 95% CI: 0.553–0.796, p = 0.031).
Base excess, with a threshold of <−2.0 mmol/L, had a sensitivity of 75% and specificity of 68% (AUC = 0.659, 95% CI: 0.445–0.775, p = 0.017). Additionally, a ferritin level above 700 ng/mL was associated with 78% sensitivity and 72% specificity in predicting mortality (AUC = 0.715, 95% CI: 0.590–0.812, p = 0.028) (Table 3, Figure 1).
Discussion
Sepsis is a leading cause of mortality and morbidity among critically ill pediatric patients, with complex pathophysiological mechanisms and variable clinical presentations that often hinder early diagnosis and risk stratification. Timely identification of high-risk patients is essential for initiating appropriate interventions and improving outcomes in the pediatric intensive care setting. In this study, we evaluated the association between early clinical and laboratory parameters and in-hospital mortality among children diagnosed with sepsis. Our findings revealed that elevated levels of lactate and ferritin, as well as decreased bicarbonate and base excess values, were significantly associated with increased mortality. Interestingly, classical inflammatory markers such as CRP and procalcitonin did not show statistical significance in predicting outcomes. This may be due to their broad sensitivity to various inflammatory conditions, potentially limiting their specificity in severe pediatric sepsis. These results suggest that these biomarkers may serve as useful tools for early prognostic assessment in pediatric sepsis and may help guide clinical decision-making.
Our findings are consistent with previous literature emphasizing the prognostic importance of lactate in pediatric sepsis. Song et al. demonstrated a significant non-linear association between lactate levels and 28-day mortality in pediatric patients, identifying a threshold of 2.2 mmol/L above which mortality risk increased notably.15 Similarly, Yalcın et al. found that blood lactate levels were more predictive of ICU mortality than base excess, underscoring its relevance in risk-stratification models.16 In our cohort, a lactate level above 2.5 mmol/L was associated with a significantly increased risk of mortality (OR = 1.21, p = 0.039), supporting its utility as a practical and accessible biomarker in early clinical evaluation.
Ferritin, an acute-phase reactant and intracellular iron storage protein, has been increasingly recognized as a marker of hyperinflammation and immune dysregulation in sepsis. In line with our findings, Sucianto et al. reported that elevated serum ferritin levels were significantly associated with mortality in pediatric sepsis, highlighting its prognostic relevance in critically ill children.17 In our study, non-survivors exhibited markedly higher ferritin levels compared to survivors (940 ± 450 vs. 480 ± 320 ng/mL, p = 0.008), and a threshold value of > 700 ng/mL demonstrated both high sensitivity (78%) and specificity (72%) for mortality prediction. These results underscore ferritin’s potential role not only as a diagnostic aid but also as a severity marker reflecting the underlying inflammatory burden in sepsis.
Metabolic acidosis is a common feature of sepsis and is often reflected in alterations of bicarbonate levels and base excess. In our study, both parameters were significantly associated with mortality: non-survivors had lower bicarbonate levels and more negative base excess values, indicating severe metabolic derangement. These findings are supported by Jovicic et al., who demonstrated that base excess is a reliable early indicator of prognosis in neonatal sepsis, with more negative values correlating with increased mortality.18 Additionally, low bicarbonate levels have been previously linked to higher severity scores and poorer outcomes in pediatric critical care settings. In our logistic regression analysis, bicarbonate and base excess emerged as independent predictors of mortality (OR = 2.16, p = 0.011 and OR = 0.51, p = 0.006, respectively), reinforcing their value in guiding early therapeutic strategies and monitoring disease progression. These biomarkers, particularly albumin and the D-dimer-to-albumin ratio, could be integrated into existing pediatric sepsis scoring tools such as pSOFA or PELOD to enhance early risk stratification and clinical decision-making.
Limitations
This study has several limitations that should be acknowledged. First, its retrospective and single-center design limits the generalizability of the findings. The results may reflect local patient characteristics, clinical practices, and resource availability, and thus may not be representative of other institutions or broader populations. Second, due to the retrospective nature of data collection, there may have been inconsistencies or missing values in the medical records, which could affect the accuracy of some variables. Third, although we identified significant associations between certain biomarkers and mortality, causality cannot be inferred. Additionally, dynamic changes in biomarker levels over time were not evaluated, and only values from the first 24 hours of PICU admission were considered. Finally, the relatively small sample size, particularly in the non-survivor group, may have limited the statistical power of some analyses, especially multivariate models. Despite these limitations, our study adds valuable insight into early prognostic assessment in pediatric sepsis. Future prospective multicenter studies with larger cohorts and serial biomarker measurements are warranted to validate these findings and to better understand the temporal dynamics of prognostic indicators in pediatric sepsis. Dynamic changes in biomarkers were not evaluated, which may limit temporal interpretation.
Conclusion
The clinical implications of our findings are significant for early risk stratification and personalized management of pediatric sepsis. The identification of readily measurable biomarkers such as lactate, ferritin, bicarbonate, and base excess provides clinicians with accessible tools for anticipating adverse outcomes and tailoring early treatment strategies, and optimizing resource allocation accordingly. These markers can aid in early recognition of critical illness, triage decisions, and prioritization of intensive monitoring and therapeutic interventions. Furthermore, the integration of these parameters into existing clinical scoring systems may enhance their predictive accuracy and assist in dynamic risk assessment throughout the patient’s ICU course. Overall, our study reinforces the growing emphasis in the literature on a multimodal, biomarker-driven approach to pediatric sepsis care, contributing to the development of evidence-based algorithms for improving survival.
Declarations
Ethics Declarations
The study was approved by the Ethics Committee of Gaziantep City Hospital Non-Interventional Clinical Research (Date: 2025-06-18, No: 218/2025)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Author Contributions (CRediT Taxonomy)
Conceptualization: S.U.
Methodology: S.U., I.B.
Formal Analysis: S.U.
Investigation: S.U., I.B.
Data Curation: S.U.
Writing – Original Draft Preparation: S.U.
Writing – Review & Editing: I.B.
Supervision: I.B.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
ALT: alanine aminotransferase
AST: aspartate aminotransferase
AUC: area under the curve
BUN: blood urea nitrogen
CI: confidence interval
CRP: C-reactive protein
LDH: lactate dehydrogenase
OR: odds ratio
PICU: pediatric intensive care unit
ROC: receiver operating characteristic
References
-
Yang WS, Kang HD, Jung SK, et al. A mortality analysis of septic shock, vasoplegic shock and cryptic shock classified by the third international consensus definitions (Sepsis-3). Clin Respir J. 2020;14(9):857-863. doi: 10.1111/crj.13218
-
Eygi E, Kucuk O, Aydemir S, Atilgan M, Dokuyucu R, Erbas O. Hydroxychloroquine mitigates cytokine storm and prevents critical illness neuromyopathy in a rat sepsis model. Medicina (Kaunas). 2024;60(11): 1791. doi: 10.3390/medicina60111791.
-
Schlapbach LJ, Watson RS, Sorce LR, et al. International consensus criteria for pediatric sepsis and septic shock. JAMA. 2024;331(8):665-674. doi:10.1001/jama.2024.0179
-
Menon K, Sorce LR, Argent A, et al. Reporting of social determinants of health in pediatric sepsis studies. Pediatr Crit Care Med. 2023;24(4):301-310. doi: 10.1097/PCC.0000000000003184
-
Demircubuk AG, Coskun MY, Demiryurek S, et al. Endothelial NOS gene Glu298Asp polymorphism in preterm neonates with respiratory distress syndrome. Pediatr Pulmonol. 2013;48(10):976-980. doi: 10.1002/ppul.22759
-
Weiss SL, Peters MJ, Alhazzani W, et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Intensive Care Med. 2020;46(1):10-67. doi:10.1007/s00134-019-05878-6
-
Varga NI, Benea AT, Suba MI, et al. Predicting mortality in sepsis: the role of dynamic biomarker changes and clinical scores—a retrospective cohort study. Diagnostics (Basel). 2024;14(17):1973. doi: 10.3390/diagnostics14171973
-
Yasseen BA, Elkhodiry AA, El-Sayed H, et al. The role of neutrophilia in hyperlactatemia, blood acidosis, impaired oxygen transport, and mortality outcome in critically ill COVID-19 patients. Front Mol Biosci. 2025;11:1510592. doi:10.3389/fmolb.2024.1510592
-
Carcillo JA, Berg RA, Wessel D, et al. A multicenter network assessment of three inflammation phenotypes in pediatric sepsis-induced multiple organ failure. Pediatr Crit Care Med. 2019;20(12):1137-1146. doi: 10.1097/PCC.0000000000002105
-
Gelbart M, Nahum E, Gelbart M, et al. Hyperlactatemia in children following brain tumor resection: prevalence, associated factors, and clinical significance. Childs Nerv Syst. 2022;38(4):739-745.
-
Valerie IC, Prabandari A, Wati DK. Ferritin in pediatric critical illness: a scoping review. Clin Exp Pediatr. 2023;66(3):98-109.
-
Fan Z, Kernan KF, Qin Y, et al. Hyperferritinemic sepsis, macrophage activation syndrome, and mortality in a pediatric research network: a causal inference analysis. Crit Care. 2023;27(1):347.
-
Hassuna NA, Elgezawy E, Mousa SO, et al. Diagnostic value of monocyte chemoattractant protein-1, soluble mannose receptor, presepsin, and procalcitonin in critically ill children admitted with suspected sepsis. BMC Pediatr. 2021;21(1):458.
-
Amer YS, Shaiba LA, Hadid A, Anabrees J, et al. Quality assessment of clinical practice guidelines for neonatal sepsis using the AGREE II instrument: a systematic review of neonatal guidelines. Front Pediatr. 2022;10:941575.
-
Song Y, Wang N, Xie X, Tian Y, Wang Y. Relationship between lactate levels and 28-day mortality in pediatric sepsis: results from the pediatric intensive care database. BMC Pediatr. 2024;24(1):712.
-
Uyur Yalcin E, Erdogan F, Topal E, Secim S, Sezer Yamanel RG. Relationship between lactate levels and length of hospital stay in infants with lower respiratory tract infection. Pediatr Allergy Immunol Pulmonol. 2021;34(2):68-72.
-
Sucianto A, Pudjiastuti P, Kawuryan DL. The role of ferritin serum level as predictor of sepsis mortality in children in Dr. Moewardi Hospital of Surakarta. J Matern Child Health. 2023;8(2):210-216.
-
Jovicic M, Milosavljevic MN, Folic M, Pavlovic R, Jankovic SM. Predictors of mortality in early neonatal sepsis: a single-center experience. Medicina (Kaunas). 2023;59(3):485.
Figures
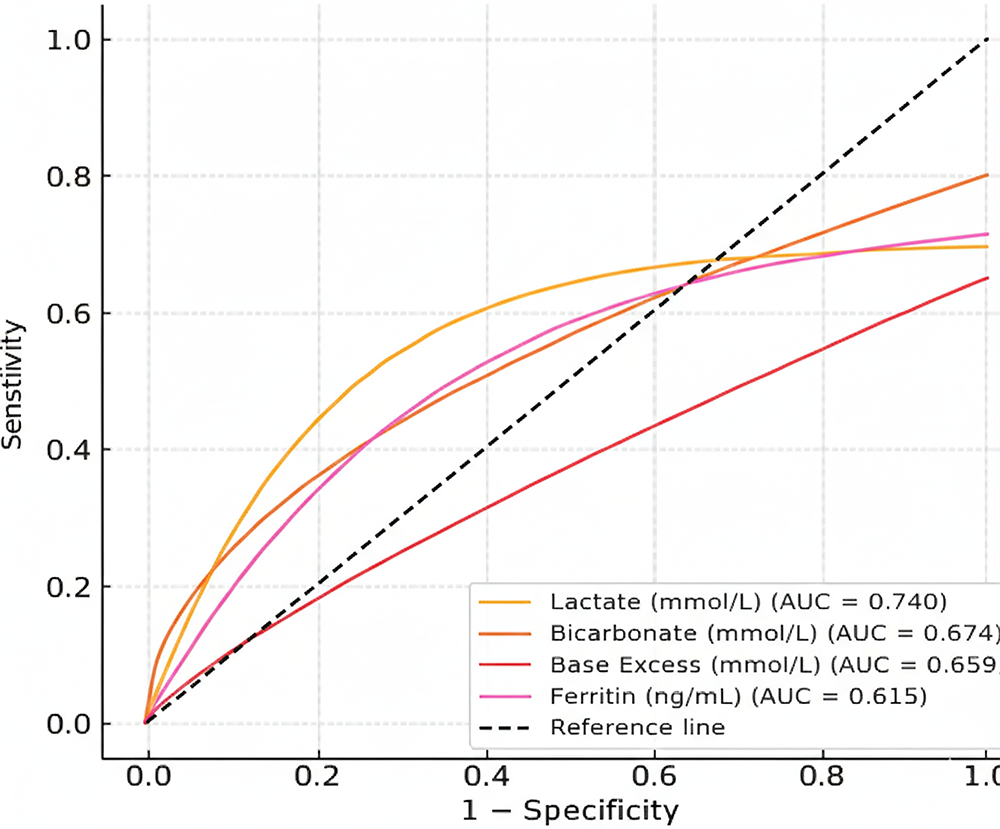
Figure 1. Receiver operating characteristic curves of lactate, ferritin, bicarbonate, and base excess for predicting mortality in pediatric sepsis
Tables
Table 1. Comparison of clinical and laboratory parameters between survivors and non-survivors
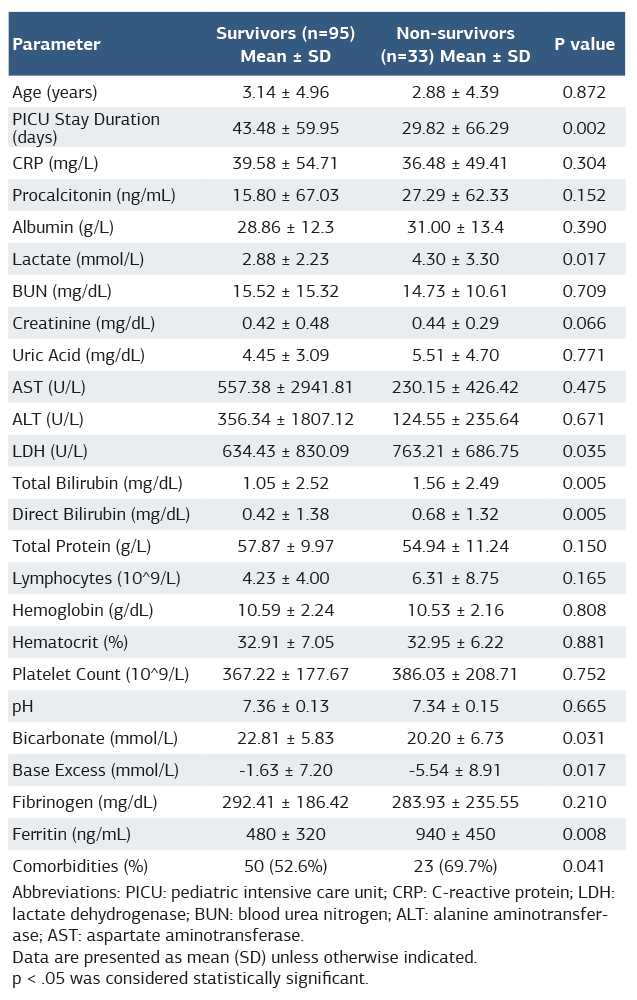
Abbreviations: PICU: pediatric intensive care unit; CRP: C-reactive protein; LDH: lactate dehydrogenase; BUN: blood urea nitrogen; ALT: alanine aminotransferase; AST: aspartate aminotransferase. Data are presented as mean (SD) unless otherwise indicated. p < .05 was considered statistically significant.
Table 2. Logistic regression analysis of factors associated with mortality
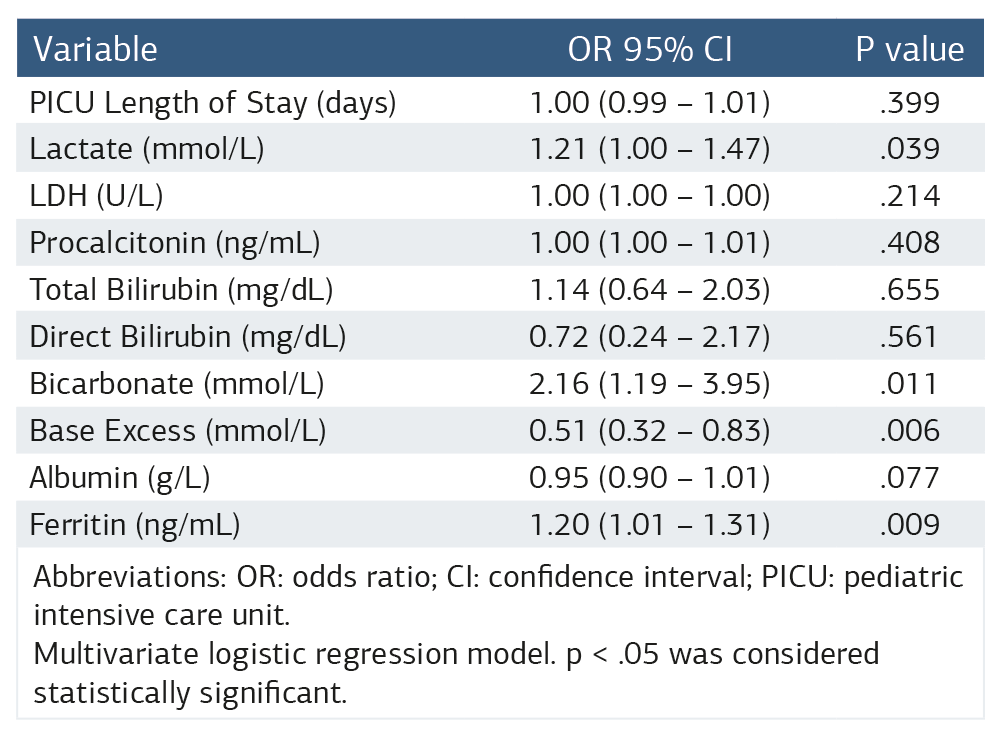
Abbreviations: OR: odds ratio; CI: confidence interval; PICU: pediatric intensive care unit. Multivariate logistic regression model. p < .05 was considered statistically significant.
Table 3. ROC analysis of biomarkers associated with mortality
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Sait Ucar, Ibrahim Bingol. Prognostic significance of clinical and laboratory parameters in pediatric intensive care sepsis: a retrospective cohort study. Ann Clin Anal Med 2026;17(Suppl 1):S39-43
- Received:
- April 12, 2025
- Accepted:
- June 23, 2025
- Published Online:
- July 8, 2025
- Printed:
- February 20, 2026