
Rhinovirus as an isolated pathogen in the pediatric intensive care unit: a 2-year inpatient experience
Childhood rhinovirus infections
Authors
Abstract
Aim Rhinoviruses (RV), non-enveloped RNA viruses of the family Picornaviridae, circulate year-round with peak incidence in early fall and late spring. They are a common cause of colds and upper respiratory tract infections in children, as well as lower respiratory tract infections and asthma attacks. The purpose of this study was to evaluate the clinical conditions, intensive care unit (ICU) admissions, oxygen supplementation requirements, and mechanical ventilation requirements of pediatric patients with positive RV tests who required hospitalization at our institution during the past two years.
Methods In this retrospective study, patients requiring hospitalization among RV-positive children were evaluated. The demographic and clinical characteristics of the patients, the need for intensive care, and the need for ventilators were analyzed.
Results The final analysis included 530 patients hospitalized with confirmed Rhinovirus infection. Admission to the ICU was required for 109 patients (20.6%). The presence of underlying comorbidities showed a strong and significant association with the need for ICU care and ventilator requirement (p < 0.001). The presence of concomitant viral infections had no effect on the need for intensive care (p: 0.330).
Conclusion This study highlights that RV is an important pathogen that can cause lower respiratory tract infections (LRTIs) of varying severity in children. Our findings suggest that RV can cause severe LRTIs requiring direct admission to the ICU and significant ventilatory support, regardless of identified viral or bacterial co-pathogens. The risk of severe infection is associated with comorbid chronic diseases.
Keywords
Introduction
Rhinoviruses (RV), non-enveloped RNA viruses belonging to the Picornaviridae family, encompass approximately 170 genotypes classified into three species: RV-A, RV-B, and RV-C.1 RV circulates year-round, exhibiting peak incidence during early autumn and late spring.2 While RV primarily infects the nasal and respiratory epithelium, infections are not confined to the upper airway and may extend to the lower respiratory tract.3
Viral infections and aeroallergens constitute well-established triggers for asthma exacerbations.4 Although predominantly associated with the common cold, RV has been implicated in the pathogenesis of asthma and recurrent wheezing, particularly among young children.5 In fact, epidemiological studies have identified RV as a significant pathogen in precipitating asthma exacerbations.6 Together with respiratory syncytial virus (RSV), RV represents a leading etiological agent of bronchiolitis.7 A surveillance study conducted in Mozambique identified RV as the most frequently detected viral pathogen among pediatric patients hospitalized with pneumonia.8 Recent reports indicate an increasing prevalence of RV detection in pediatric intensive care units.9
Based on the extant literature and available evidence, rhinoviruses have been established as not merely a common etiologic agent of upper respiratory tract infections, but also a significant contributor to respiratory diseases of varying severity. The present study sought to evaluate the clinical diagnoses, disease manifestations, intensive care unit (ICU) admissions, oxygen supplementation requirements, and mechanical ventilation needs among pediatric patients who tested positive for RV and subsequently required hospitalization at our institution during the preceding two-year period.
Materials and Methods
This retrospective study utilized patient data extracted from the hospital’s electronic health record system. We analyzed respiratory viral panel (RVP) results obtained via multiplex polymerase chain reaction (PCR) from nasopharyngeal specimens collected between January 1, 2023, and December 31, 2024. These diagnostic tests were ordered for pediatric patients (aged 0-18 years) presenting to the Pediatric Pulmonology, Pediatric Emergency, and Pediatric Intensive Care Departments. During the study period, 3098 RVP tests were performed, yielding 1156 RV-positive results. From this cohort of 1156 unique RV-positive patients, 578 required inpatient admission. Of these hospitalized patients, 48 were subsequently excluded due to documented concomitant bacterial infection, confirmed by positive blood, sputum, or throat cultures, where the clinical presentation was determined not to be primarily attributable to RV infection. This selection process resulted in a final sample of 530 patients.
Respiratory samples were processed using reverse transcription real-time polymerase chain reaction (RT-qPCR). Commercial multiplex RT-qPCR kits were employed for viral detection Bio- Speedy™ Respiratory RT-qPCR, Bioeksen, Istanbul, Türkiye, and SCM Biotech Co., Nevşehir, Türkiye). Assays were performed on Rotor-Gene Q (Qiagen, Hilden, Germany) and CFX96 Real- Time PCR Detection System (Bio-Rad Laboratories, Hercules, CA, USA) thermal cyclers. Threshold cycle (Ct) values were interpreted according to the respective manufacturer’s guidelines. The multiplex panels detected genetic material from the following respiratory viruses: RSV, Influenza A and B, Adenovirus, Parainfluenza viruses (types 1-4), Human Bocavirus (HBoV), RV, and Human Metapneumovirus (hMPV).
For the final cohort of 530 RV-positive inpatients, the following data were collected: age, gender, and season of admission. Clinical data analyzed included primary diagnosis at hospitalization, length of stay, requirement for supplemental oxygen, need for mechanical ventilation, and admission to the ICU. Laboratory and clinical variables extracted from the hospital’s data registry system included: results of the full RVP (to identify viral co-detections), complete blood count parameters (leukocyte, neutrophil, lymphocyte counts), C-reactive protein (CRP) levels, and presence of underlying chronic conditions, categorized as respiratory or other. These variables were analyzed to identify potential factors associated with clinical severity.
Ethical ApprovalThis study was approved by the Ethics Committee of Necmettin Erbakan University Faculty of Medicine (Date: 2025-01-10, No: 5424).
Statistical AnalysisData analysis was performed on SPSS version 23 statistical software IBM Corp., Armonk, NY, USA). Descriptive statistics were generated, with categorical variables presented as frequency distributions and percentages, while continuous variables were summarized through appropriate measures of central tendency and dispersion (mean, standard deviation, median, maximum, minimum). Statistical significance was established at p < 0.05 with a 95% confidence interval for all inferential analyses.
Comparisons between categorical variables were conducted by chi-squared analyses (Pearson’s chi-squared test and Fisher’s exact test, as appropriate). Following significant chi-squared results, post hoc pairwise comparisons were performed to identify specific group differences, with Bonferroni correction applied to adjust for multiple comparisons and mitigate Type I error inflation.
The normality of continuous variables was assessed via the Shapiro-Wilk test. For non-normally distributed data, the Mann- Whitney U test was employed for two-group comparisons, while the Kruskal-Wallis test was utilized for comparisons involving more than two groups. When the Kruskal-Wallis test yielded significant results, subsequent pairwise comparisons were conducted through the Mann-Whitney U test with Bonferroni- adjusted significance levels to identify specific between-group differences. Spearman’s rank correlation coefficient (p) was calculated to assess the association between non-normally distributed continuous variables.
Reporting GuidelinesThis study was reported in accordance with the STROBE guidelines.
Results
The final analysis included 530 patients hospitalized with confirmed Rhinovirus infection. Of these patients, 178 (33.6%) were aged ≤ 24 months, and 218 (41.1%) were female. Admission to the ICU was required for 109 patients (20.6%). The mean overall length of hospital stay was 6.56 ± 5.72 days, while the mean length of stay for patients admitted to the ICU was 9.94 ± 9.50 days. There were no mortalities recorded during the study period. Detailed sociodemographic characteristics, clinical features, and medical histories of the patient cohort are presented in Table 1.
Laboratory findings showed significant variability in inflammatory markers and blood counts between patients. Several parameters exhibited skewed distributions, with means differing substantially from medians. Key reported values included a mean leukocyte count of 12137.71 ± 5704.42 µL (Median: 10990.00 µL) and a mean CRP of 18.85 ± 29.58 mg/L (Median: 7.00 mg/L). The mean neutrophil-to-lymphocyte ratio was 2.86 ± 4.45 (Median: 1.50). Other recorded mean values were 6659.67 ± 5119.22 µL for neutrophil count, 4242.89 ± 2865.63 µL for lymphocyte count, and 18.88 ± 14.32 mm/h for erythrocyte sedimentation rate.
Data for leukocyte, neutrophil, and lymphocyte counts and neutrophil/lymphocyte ratios were not available for 15 patients. CRP (C-reactive protein) values were not available for 21 patients. Sedimentation data for 100 patients were not available.
Factors associated with the need for ICU admission are compared in Table 2. Analysis revealed that the patient’s age group was not statistically associated with ICU admission (p = 0.126). However, the presence of underlying comorbidities showed a strong significant association with the need for ICU care (p < 0.001). Specifically, a significantly higher proportion of patients with comorbidities were admitted to the ICU (34.2%; 54/158) compared to patients without comorbidities (14.8%; 55/372). The presence of a co-detected viral agent was not found to be significantly associated with ICU admission (p = 0.330).
An analysis of factors associated with the requirement for non- invasive or invasive ventilation (NIV/IV) is presented in Table 3. The need for NIV/IV was not significantly associated with patient age group (p = 0.881). However, a strong, significant association was observed between the presence of underlying comorbidities and the requirement for NIV/IV (p < 0.001). Patients with comorbidities were significantly more likely to need NIV/IV support (12.7%; 20/158) compared to those without comorbidities (4.0%; 15/372).
Discussion
Although widely recognized as a cause of the common cold, RV is also a significant etiology of both upper and lower respiratory tract infections. It represents an important pathogen, particularly in young children, where it is associated with hospitalization and acute respiratory illness.10,11 Supporting this, Louie et al. reported RV association with severe respiratory illness necessitating ICU admission in children, noting that over half required mechanical ventilation with a median ICU stay of 7 days.12 Our study aligns with the understanding that RV can cause severe disease; while we observed a substantial number of RV-related hospitalizations over two years, 20.6% of these admitted patients ultimately required ICU care, predominantly due to lower respiratory tract infection. Consistent with previous reports, the need for intensive care in our cohort was significantly associated with the presence of underlying comorbidities. Besides, high-flow nasal oxygen (HFNO) was the most frequently utilized respiratory support modality within the ICU.
Bronchiolitis and pneumonia are frequently cited as the primary diagnoses leading to RV-associated hospital admission. Hasegawa et al. identified RV as the second most common virus (28%), following RSV, in children requiring ICU admission for bronchiolitis.13 Similarly, another study identified pneumonia and bronchiolitis as the most common diagnoses among children needing intensive care for RV or enterovirus (EV) infections.14 Consistent with the literature, bronchiolitis and pneumonia were the predominant diagnoses in our hospitalized cohort (Table 1).
The burden of severe RV illness often falls on younger children. In the study by Varela et al, 42.2% of children hospitalized with lower respiratory tract infection due to rhinovirus or another viral agent were younger than 2 years.15 In our study cohort, while spanning a broader age range, younger children were also prominently represented among severe cases, with 40.4% of patients admitted to the ICU being ≤ 24 months old. This vulnerability in younger children may relate to factors such as airway size and an immature immune system, potentially struggle to control the infection effectively.
Underlying health conditions are known risk factors for severe RV outcomes. A study from China indicated that RV was more prevalent among children with asthma or immunosuppression admitted to the ICU.16 Another study highlighted RV’s role in triggering exacerbations in children with pre-existing respiratory conditions like asthma.17 Our findings resonate with this, as asthma was the most common chronic condition identified in our hospitalized cohort, and we found a statistically significant association between the presence of any comorbidity and the likelihood of ICU admission. Children with chronic health conditions may experience increased susceptibility to infections or exhibit a more pronounced inflammatory response, potentially leading to more severe disease courses.
Regarding the role of viral co-detection, some studies suggest no significant association between concurrent viral infections and disease severity in children hospitalized with RV.18,19 Miller et al., for instance, found that viral co-detections did not significantly alter the clinical status of children hospitalized with rhinovirus.19 Our findings align with this perspective; in our cohort of 530 patients, the presence of a concomitant virus detected on the RVP was not associated with an increased likelihood of ICU admission. This suggests that RV infection alone is capable of causing lower respiratory tract disease severe enough to necessitate intensive care.
Detailed analysis of respiratory support modalities used for the 109 patients admitted to the ICU in our study revealed that HFNO was the most common intervention, utilized in 67.8% of cases. Comparing our findings to the literature, one study reported HFNO use in 32% and NIV in 33.3% of children with RV/EV infection requiring respiratory support,14 while another noted NIV use in 53% and IV in 8% of RV/EV-related ICU admissions.20 HFNO therapy is a frequently employed strategy in our clinical setting, particularly for bronchiolitis and pneumonia in young children, often leading to observable clinical improvement. The proposed benefits of HFNO include rapid clinical improvement in patients, especially in the treatment of bronchiolitis and pneumonia in young children, reduction of anatomical dead space, generation of positive end-expiratory pressure (PEEP), and improved patient comfort compared to standard oxygen delivery methods.21 The relatively lower rates of NIV and IV observed in our ICU cohort compared to some published reports in the literature might reflect the proactive and potentially effective application of HFNO therapy in our institution.
Limitations
Finally, certain limitations of our study should be acknowledged. Its retrospective nature precluded performing RV genotyping. Given that different RV species or genotypes may exhibit varying clinical virulence, future prospective studies incorporating viral typing could provide important details concerning genotype-specific clinical presentations and outcomes, further contributing to the literature.
Conclusion
This study underscores that RV is a significant pathogen capable of causing lower respiratory tract infections of varying severity in children. Our findings demonstrate that RV, independent of identified viral or bacterial co-pathogens, can directly lead to severe lower respiratory tract infections necessitating ICU admission and substantial respiratory support. A key finding from our analysis was that the presence of underlying comorbidities significantly increased the risk for ICU admission among children hospitalized with RV infection. Children with RV positivity, particularly those with pre-existing chronic conditions such as asthma, immunosuppression, or neurological abnormalities, warrant heightened clinical vigilance. Prompt assessment and consideration of respiratory support strategies, including HFNO and non-invasive ventilation, should be considered in these higher-risk patients to manage respiratory distress effectively.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Necmettin Erbakan University Faculty of Medicine (Date: 2025-01-10, No: 5424).
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from patients’ parents or legal guardians at the time of hospital admission. For this retrospective analysis of anonymized
clinical records, the requirement for additional informed consent was waived by the ethics committee.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding
author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Author Contributions (CRediT Taxonomy)
Conceptualization: N.B.E., S.P.
Methodology: N.B.E., A.A.
Investigation: N.B.E., A.A., O.K.
Data curation: N.B.E., M.G.
Formal analysis: N.B.E., S.P.
Writing – original draft: N.B.E.
Writing – review & editing: S.P., M.Ö., O.K.
Supervision: S.P.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
CRP: C-Reactive Protein
Ct: Cycle Threshold
HFNO: High-Flow Nasal Oxygen
ICU: Intensive Care Unit
LRTI: Lower Respiratory Tract Infection
NIV: Non-Invasive Ventilation
PCR: Polymerase Chain Reaction
RVP: Respiratory Viral Panel
RSV: Respiratory Syncytial Virus
RV: Rhinovirus
RT-qPCR: Reverse Transcription Quantitative Polymerase Chain Reaction
References
-
Bochkov YA, Gern JE. Rhinoviruses and their receptors: implications for allergic disease. Curr Allergy Asthma Rep. 2016;16(4):30. doi: 10.1007/s11882-016-0608-7
-
Toivonen L, Schuez-Havupalo L, Karppinen S, et al. Rhinovirus infections in the first 2 years of life. Pediatrics. 2016;138(3):e20161309. doi: 10.1542/peds.2016-1309
-
Ljubin-Sternak S, Meštrović T, Ivković-Jureković I, et al. The emerging role of rhinoviruses in lower respiratory tract infections in children–clinical and molecular epidemiological study from Croatia, 2017–2019. Front Microbiol. 2019;10:2737. doi: 10.3389/fmicb.2019.02737
-
Reisli İ, Köksal Y. Astım Patogenezi [Pathogenesis of Asthma]. Selçuk Tıp Derg. 2002;18(4);267-73.
-
Gern JE. Rhinovirus and the initiation of asthma. Curr Opin Allergy Clin Immunol. 2009;9(1):73-8.
-
Ortega H, Nickle D, Carter L. Rhinovirus and asthma: Challenges and opportunities. Rev Med Virol. 2021;31(4):e2193. doi: 10.1002/rmv.2193
-
Makrinioti H, Hasegawa K, Lakoumentas J, et al. The role of respiratory syncytial virus - and rhinovirus-induced bronchiolitis in recurrent wheeze and asthma — a systematic review and meta-analysis. Pediatric Allergy Immunol. 2022;33(3):e13741.
-
Annamalay AA, Lanaspa M, Khoo SK, et al. Rhinovirus species and clinical features in children hospitalised with pneumonia from Mozambique. Trop Med Int Health. 2016;21(9):1171-80.
-
Lonngren C, Morrow BM, Haynes S, Yusri T, Vyas H, Argent AC. North–South divide: Distribution and outcome of respiratory viral infections in paediatric intensive care units in Cape Town (South Africa) and Nottingham (United Kingdom). J Paediatr Child Health. 2014;50(3):208-15.
-
Drysdale SB, Mejias A, Ramilo O. Rhinovirus – not just the common cold. J Infect. 2017;74(Suppl.1):S41-6.
-
Jacobs SE, Lamson DM, St George K, Walsh TJ. Human rhinoviruses. Clin Microbiol Rev. 2013;26(1):135-162. doi:10.1128/CMR.00077-12
-
Louie JK, Roy-Burman A, Guardia-LaBar L, et al. Rhinovirus associated with severe lower respiratory tract infections in children. Pediatr Infect Dis J. 2009;28(4):337-9.
-
Hasegawa K, Pate BM, Mansbach JM, et al. Risk factors for requiring intensive care among children admitted to ward with bronchiolitis. Acad Pediatr. 2015;15(1):77-81.
-
Barlas UK, Akcay N, Menentoglu ME, et al. Assessment of the clinical course of human rhinovirus/Enterovirus infections in pediatric intensive care. Pediatr Infect Dis J. 2023;42(12):e454-60.
-
Varela FH, Sartor ITS, Polese-Bonatto M, et al. Rhinovirus as the main co- circulating virus during the COVID-19 pandemic in children. J Pediatr (Rio J). 2022;98(6):579-86.
-
Li YT, Liang Y, Ling YS, Duan MQ, Pan L, Chen ZG. The spectrum of viral pathogens in children with severe acute lower respiratory tract infection: a 3-year prospective study in the pediatric intensive care unit. J Med Virol. 2019;91(9):1633-42.
-
Lau SK, Yip CC, Tsoi H-W, et al. Clinical features and complete genome characterization of a distinct human rhinovirus (HRV) genetic cluster, probably representing a previously undetected HRV species, HRV-C, associated with acute respiratory illness in children. J Clin Microbiol. 2007;45(11):3655-64.
-
Leotte J, Trombetta H, Faggion HZ, et al. Impact and seasonality of human rhinovirus infection in hospitalized patients for two consecutive years. J Pediatr (Rio J). 2017;93(3):294-300.
-
Miller EK, Lu X, Erdman DD, et al. Rhinovirus-associated hospitalizations in young children. J Infect Dis. 2007;195(6):773-81.
-
Smith ME, Wilson PT. Human rhinovirus/enterovirus in pediatric acute respiratory distress syndrome. J Pediatr Intensive Care. 2020;9(02):81-6.
-
Dysart K, Miller TL, Wolfson MR, Shaffer TH. Research in high flow therapy: mechanisms of action. Respir Med. 2009;103(10):1400-5.
Tables
Table 1. Sociodemographic characteristics, clinical features, and medical histories of patients
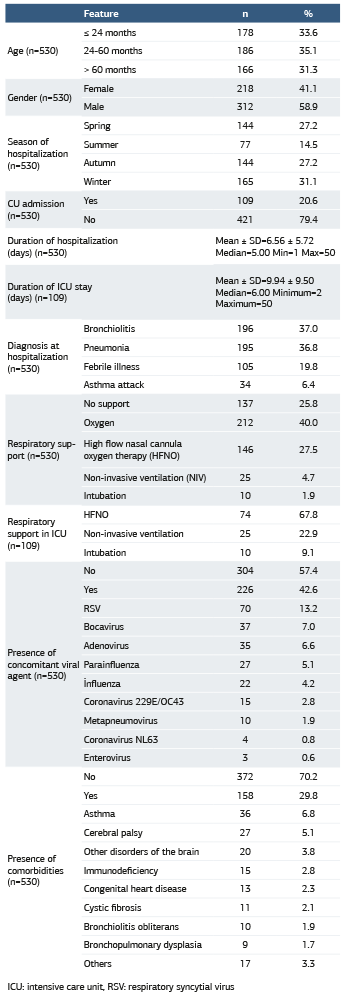
ICU: intensive care unit, RSV: respiratory syncytial virus
Table 2. Comparison of the need for ICU admission with patient age, presence of comorbidities, and co-viral agents
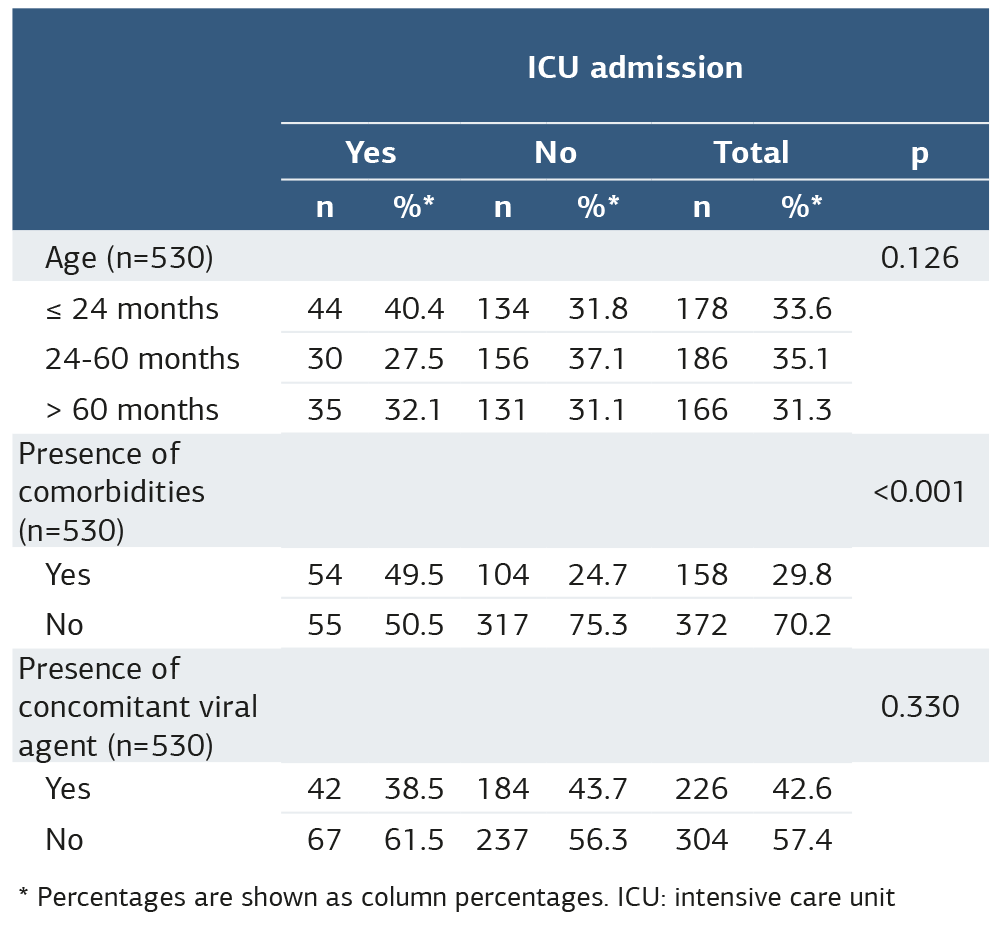
* Percentages are shown as column percentages. ICU: intensive care unit
Table 3. Comparison of patients’ need for NIV-IV with patient age, presence of comorbidities, and co-viral agents
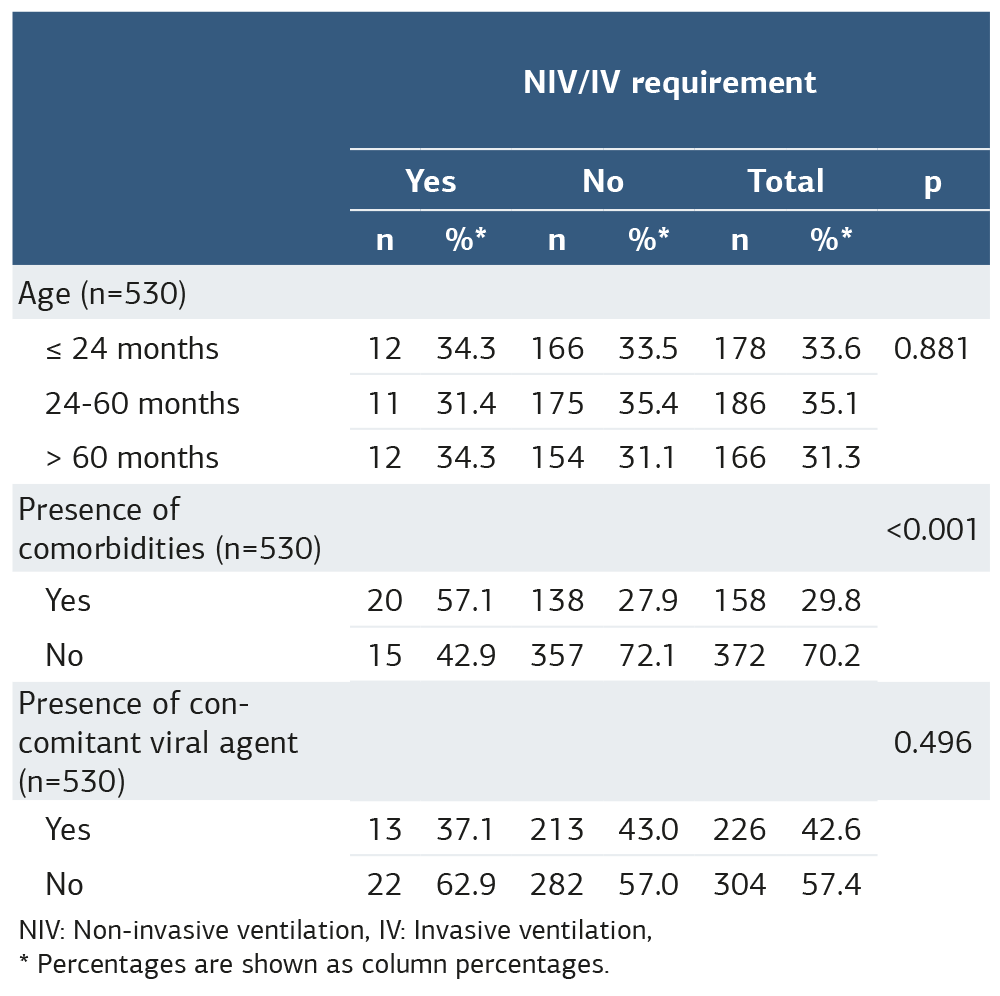
NIV: Non-invasive ventilation, IV: Invasive ventilation, * Percentages are shown as column percentages.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Nefise Betül Ercan, Sevgi Pekcan, Abdullah Akkuş, Mehmet Özdemir, Mustafa Genceli, Onur Kaya. Rhinovirus as an isolated pathogen in the pediatric intensive care unit: a 2-year inpatient experience. Ann Clin Anal Med 2026;17(Suppl 2):S130-134. doi: 10.4328/ ACAM.22705
- Received:
- April 2, 2025
- Accepted:
- May 19, 2025
- Published Online:
- July 24, 2025
- Printed:
- March 20, 2026