
Evaluation of the safety and efficacy of the limited rotation of the mobile-bearing posterior stabilised total knee prosthesis: a retrospective study
LRMB total knee arthroplasty outcomes
Authors
Abstract
Aim Reports on mobile-bearing total knee prostheses (TKPs) are limited, mostly focusing on designs with restricted rotation. It is hypothesized that limited-rotation designs may preserve the benefits of mobile-bearing systems while minimizing complications. This study aimed to present short-term clinical and radiological outcomes of limited-rotation mobile-bearing (LRMB) TKPs and assess prosthesis survival.
Methods This retrospective study included 120 patients who underwent total knee arthroplasty between January 2022 and January 2023. Of these, 103 patients who received the same LRMB implant and had a minimum follow-up of one year were analyzed. Pre and postoperative scores for the Knee Society Score (KSS), stair climbing ability, pain Visual Analog Scale (pVAS), Oxford Knee Score (OKS), and range of motion (ROM) were evaluated.
Results Postoperative KSS, stair climbing, pVAS, OKS, and ROM scores showed statistically significant improvements compared to preoperative values (p < 0.001). No major complications such as insert dislocation or radiographic loosening were observed.
Conclusion LRMB total knee arthroplasty demonstrated notable short-term improvements in pain and function, with no mechanical complications. Restricting excessive rotation may lower wear-related risks, making LRMB a reliable option, especially for active patients.
Keywords
Introduction
Total knee prosthesis (TKP) is a widely used surgical intervention for advanced knee osteoarthritis, with well-documented success in achieving satisfactory outcomes.1 According to the literature, the survival rate of TKPs over a 20-year period is reported to be approximately 90–95%.2 Although extensive research supports the effectiveness of TKPs in enhancing patient outcomes, the optimal prosthesis design remains a subject of ongoing debate.3
Fixed-bearing (FB) total knee arthroplasty (TKA) has been widely accepted as a standard technique, with numerous studies demonstrating excellent results across various design modifications—including variations in condylar geometry, tibial surface coverage (with or without patellar resurfacing), and cruciate ligament retention.4,5 In contrast, mobile-bearing (MB) TKPs have been less extensively reported, and most available studies focus on limited-rotation MB designs.6,7
The rotating platform in MB prostheses allows for improved tibiofemoral alignment without limiting axial rotation of the polyethylene insert. It has been hypothesized that MB designs provide a more conforming articulation, which reduces contact stress on the articular surfaces and improves functional outcomes. The axial mobility of the insert during daily activities may also lower stress at the bone–implant interface, potentially reducing polyethylene wear and enhancing implant longevity.8
However, potential disadvantages of the MB design include increased implant costs and the risk of insert dislocation.9,10 In our study, the limited-rotation mobile-bearing total knee prosthesis allows rotational movement of the polyethylene insert within ±10°, restricted by both a central and an anterior peg on the tibial component. In contrast, fully rotational mobile-bearing designs typically include only a central peg, allowing greater rotational freedom of the insert.
Fully rotational mobile-bearing systems enhance self-alignment and reduce polyethylene wear by accommodating femorotibial incongruities during dynamic activities. However, the unrestricted rotational freedom may lead to increased shear forces at the bone-implant interface, posing a risk for bearing spin-out or instability. In contrast, limited-rotation mobile-bearing (LRKMB) prostheses offer controlled rotational mobility that mitigates these risks. LRKMB designs aim to preserve the inherent advantages of mobile-bearing constructs, such as improved femorotibial conformity and reduced contact stress, while minimizing complications associated with unrestricted rotation. Furthermore, the restricted arc of rotation in LRKMB systems (typically ±10°) is considered to more closely reflect the physiological rotational range of the native knee, potentially contributing to improved kinematics and patient satisfaction in the early postoperative period.11 This study aims to present the short-term clinical and radiological outcomes of limited-rotation mobile-bearing (LRMB) TKPs and evaluate implant survival.
Materials and Methods
This retrospective study was conducted using data obtained from total knee arthroplasty (TKA) procedures performed in the Department of Orthopaedics and Traumatology at our institution. The study population consisted of 120 patients who underwent TKA between January 2022 and January 2023. Patients were selected based on predetermined inclusion and exclusion criteria, and those who did not meet the criteria were excluded from the study. Ultimately, 103 patients who received the same implant system and had a minimum of one year of follow-up were included in the final analysis.
Prior to surgery, all patients underwent a preoperative anaesthesia evaluation, followed by a detailed physical examination approximately one week before the operation. Demographic data, implant selection, and preoperative planning measurements were documented at this stage.
Informed consent was obtained from all participants before surgery. This document also included detailed information regarding the postoperative care process.
During the initial three days postoperatively, routine inpatient evaluations were conducted. Follow-up assessments focused on clinical and radiological outcomes, particularly at the 1-year mark. All postoperative control data were systematically recorded.
Patient records from 2022 to 2023 were retrospectively reviewed and evaluated using defined criteria. Only patients with a minimum of one year of regular postoperative follow-up were included in the analysis.
During the study period, our clinic predominantly used limited-rotation mobile-bearing (LRMB) prostheses (KAV Mobile Bearing Total Knee Prosthesis System, Kayseri, Türkiye) (Figure 1).
Inclusion criteria were defined as being between 30 and 85 years of age, having a diagnosis of osteoarthritis or rheumatoid arthritis, having undergone LRMB total knee arthroplasty, having a minimum follow-up period of 6 months, and having completed the clinical questionnaire during follow-up visits.
Exclusion criteria included a history of malignancy, failure to attend regular follow-up appointments, and having undergone unicondylar knee arthroplasty.
Surgical TechniqueAll procedures were performed under spinal anaesthesia with the patient in the supine position and the operative leg supported laterally. Standard sterilisation and draping protocols were followed. An elastic bandage was applied to the limb, and a pneumatic tourniquet was inflated to 250 mmHg.
A midline skin incision was made, followed by dissection through the subcutaneous tissue. Arthrotomy was performed approximately 5 mm lateral to the vastus medialis muscle, starting about three fingerbreadths proximal to the superior pole of the patella. A segment of the joint capsule was excised to create an approximate 5 mm gap between the patella and the capsule.
Intramedullary guides were used for femoral alignment, and extramedullary guides for tibial alignment. Bone cuts were made in accordance with the specifications of the pre-selected implant design. Trial components were inserted, and appropriate soft tissue balancing was performed. The need for patellar resurfacing was assessed intraoperatively.
After completing the bone preparation, thorough irrigation and lavage were carried out. The limited-rotation mobile-bearing (LRMB) tibial insert was then implanted using the preferred posterior-stabilized (PS) KAV total knee prosthesis system, with the corresponding tibial and femoral components applied as per the manufacturer’s instructions. Once the cement had set, the tourniquet was deflated and haemostasis was achieved.
A vacuum drain was placed in all cases and removed 24 hours postoperatively. The joint capsule and soft tissues were closed in layers. All patients received prophylactic antibiotic therapy with cefazolin and thromboprophylaxis with low-molecular-weight heparin.
Postoperative RehabilitationAll patients were mobilized on the first postoperative day with the assistance of a physiotherapist. Continuous passive motion (CPM) devices were used for knee joint mobilization starting within 24 hours following surgery, with a recommended usage of 4-6 hours per day to maintain joint mobility and prevent stiffness. Active and passive range-of-motion (ROM) exercises, along with quadriceps strengthening exercises, were initiated early to promote functional recovery. Full weight-bearing was encouraged as tolerated, with gradual progression based on the patient’s comfort and tolerance. Partial weight-bearing was introduced on the first postoperative day, progressing to full weight-bearing by the third or fourth postoperative day.
Patients were typically discharged once they demonstrated independent ambulation with assistive devices, within 3 to 4 days postoperatively. All patients had their sutures removed between postoperative days 14 and 16. Routine follow-up appointments were scheduled at 6 weeks, 3 months, and 6 months postoperatively to monitor progress and adjust rehabilitation plans as necessary. The first clinical evaluations and physical examination records were obtained during the outpatient clinic visit in the 6th postoperative week.
The rehabilitation protocol aimed to facilitate functional recovery while minimizing complications. On average, patients achieved independent ambulation within 3-4 days postoperatively.
Data Collection and Outcome MeasuresFollowing the initial three days of standard inpatient evaluation in the postoperative period, patients were scheduled for outpatient clinic visits at 3 months, 6 months, and 1 year after surgery. Subsequent annual follow-up appointments were conducted in accordance with the standard monitoring protocol.
Clinical evaluations included the Oxford Knee Score (OKS), stair-climbing test, Visual Analogue Scale for pain (pVAS), Knee Society Score (KSS), and range of motion (ROM). These parameters were systematically recorded during the preoperative period and reassessed during postoperative visits.
The primary outcome measures were:
Knee Society Score (KSS),
Stair-climbing ability,
Visual Analogue Scale (pVAS) for pain.
The secondary outcome measures included:
Oxford Knee Score (OKS),
Knee joint range of motion (ROM).
The primary objective was to evaluate the functional efficacy of the surgical intervention by comparing preoperative values with postoperative results, particularly at the 6-month follow-up.
Standard anteroposterior radiographs were obtained during the final follow-up to evaluate component positioning and detect any signs of loosening. Prosthesis survival was assessed by identifying any cases of mechanical failure, instability, or revision surgery.
Power AnalysisA retrospective cohort design was employed to evaluate the safety and efficacy of limited-rotation mobile-bearing total knee prostheses. To determine the minimum required sample size, anticipated changes in patients’ range of motion (ROM), pain scores (pVAS), and functional scores [Knee Society Score (KSS) and Oxford Knee Score (OKS)] were estimated based on data from previous studies. Assuming a type I error rate (α) of 5% and a statistical power (1–β) of 95%, a power analysis was conducted using the paired t-test model in G*Power version 3.1.9.4. A moderate effect size (Cohen’s d) was used for the estimation. Based on these calculations, it was deemed appropriate to include 103 patients, as retrospective evaluation would be performed using available patient records.
Ethical ApprovalThis study was approved by the Non-Interventional Clinical Research Ethics Committee of Kayseri City Hospital (Date: 2024-05-28, No: 100).
Statistical AnalysisThe normality of continuous variables was assessed using histograms, Q-Q plots, and the Shapiro-Wilk test for the comparison of pre- and post-operative clinical measurements. Based on the normality test results, parametric tests were applied to variables with a normal distribution, while non-parametric tests were used for non-normally distributed data. Descriptive statistics are presented as mean, median, minimum, maximum, and standard deviation.
Paired samples t-test and Wilcoxon tests were used to compare pre- and post-operative clinical measurements for variable pairs. Based on the p-values, statistically significant differences were observed in all objective knee variables between pre- and post-operative measurements. Additionally, the effect of the operation on stair climbing ability was visualized using bar charts comparing pre- and post-operative stair climbing levels. This provides a useful tool for assessing the impact of the operation on changes in this domain.
The effect of gender on pre- and post-operative measurements was analyzed using multivariate analysis. For this purpose, Pillai’s Trace statistic was chosen, considering the assumptions of MANOVA (Multivariate Analysis of Variance). In this study, Pillai’s Trace and associated p-values indicated that gender had no statistically significant effect on any of the pre- or post-operative measurements. All statistical analyses were performed using IBM SPSS Statistics version 26.
Reporting GuidelinesThis study is reported in accordance with the STROBE guidelines.
Results
The demographic characteristics of the participants, including age, sex, height (cm), and weight (kg), are presented in Table 1.
Statistically significant improvements were observed in postoperative Knee Society Score (KSS), stair climbing ability, Pain Visual Analog Scale (pVAS), Oxford Knee Score (OKS), and range of motion (ROM) when compared to preoperative values.
To assess changes in stair climbing ability, a cross-tabulation analysis was performed comparing pre- and postoperative categories. A graphical representation of these changes is provided in Figure 2.
The study population consisted of 91 female and 12 male patients. Descriptive statistics comparing pre- and postoperative outcomes by sex are summarized in Table 2.
Correlation analyses were conducted to evaluate the relationships between changes in clinical outcome measures. The following results were obtained:
• A strong, positive, and statistically significant correlation was observed between changes in OKS and KSS Function (ρ = 0.894; p < 0.05).
• A moderate, positive, and statistically significant correlation was observed between changes in OKS and KSS Knee Total (ρ = 0.484; p < 0.05).
• No statistically significant correlation was found between changes in OKS and ROM (ρ = 0.182; p > 0.05).
• A moderate, positive, and statistically significant correlation was found between changes in KSS Function and KSS Knee Total (ρ = 0.522; p < 0.05).
• No statistically significant correlation was observed between changes in KSS Function and ROM (ρ = 0.176; p > 0.05).
• A moderate, positive, and statistically significant correlation was found between changes in KSS Knee Total and ROM (ρ = 0.436; p < 0.05).
These correlation results are illustrated in Figure 3.
Importantly, no major postoperative complications, including insert dislocations, were reported in any patient throughout the follow-up period.
Discussion
Mobile-bearing (MB) knee arthroplasty systems were initially introduced to overcome certain biomechanical limitations of fixed-bearing designs. Over time, MB systems have been increasingly adopted for select patient populations due to their theoretical advantages in wear reduction, implant longevity, and joint kinematics.8,9 However, conventional instrumentation has also demonstrated near-perfect clinical results for up to 10 to 20 years, as extensively documented in the literature.10,11,12 Numerous studies suggest that while conventional fixed-bearing designs may be more suitable for elderly patients, MB systems may offer superior outcomes in younger, more active individuals. This distinction is primarily attributed to the reduced surface polyethylene wear, lower risk of aseptic loosening, and potentially improved implant survival associated with mobile-bearing (MB) designs.13,14 Although the present study includes only short-term data, no signs of aseptic loosening or insert wear (based on medial and lateral radiographic gap measurements) were detected in our radiographic assessments.
One of the key theoretical benefits of MB systems is the potential for the tibial component to realign itself under the femoral component—an effect termed “self-alignment”—which may help reduce malpositioning of the tibial implant. It is hypothesized that this mechanism could enhance patellofemoral tracking and reduce anterior knee pain. The significant improvement in VAS scores from the preoperative to the postoperative period (p < 0.001) observed in our study further supports this assumption. At the same time, the literature reveals conflicting evidence: while some publications argue that component design and surgical technique can reduce patellofemoral complications, others report no measurable difference in outcomes. This ongoing debate reflects the complexity of rotational alignment’s role in early clinical results.15
Despite their advantages, MB designs are not without drawbacks. Potential disadvantages include increased implant cost and the risk of insert dislocation.6,7 Several case series in the literature have described such dislocations, usually attributed to excessive rotational forces causing disengagement of the polyethylene insert from the tibial base.16 In response, limited-rotation mobile-bearing (LRMB) designs have been developed to restrict rotational motion within a safe range, thereby reducing the likelihood of dislocation. In our study, no insert dislocations were observed, supporting the safety profile of the LRMB design.
Another purported benefit of MB-TKA is the reduction in polyethylene wear and component loosening. In line with this theory, our cohort exhibited no radiographic signs of polyethylene insert wear (based on medial and lateral joint space measurements), osteolysis, or loosening during the follow-up period.5,16,17 Nevertheless, contradictory findings exist. For instance, Huang et al. reported a higher incidence of femoral-side osteolysis in MB patients, hypothesizing that the congruent articulating surfaces may generate finer polyethylene debris, which is more readily phagocytosed, thus contributing to osteolysis.18 It is conceivable that LRMB designs, by limiting rotational movement, may help mitigate this issue.
When comparing MB and conventional fixed-bearing designs, most studies—including ours—have found no significant differences in postoperative outcome scores such as the Knee Society Score (KSS), Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and Visual Analog Scale (VAS) for pain. However, both groups consistently show substantial improvements from preoperative baselines.19,20,21,22
In our study, the mean Oxford Knee Score (OKS) was 30.01, and the functional subscore of the Knee Society Score (KSS) was 54.17 in patients who underwent total knee arthroplasty with a mobile-bearing prosthesis. These findings demonstrate the functional effectiveness of mobile-bearing designs. In a study by Kim et al., the mean OKS was reported as 32.1 in the mobile-bearing group, with no significant difference compared to the fixed-bearing group.23 Similarly, Ruckenstuhl et al. found no statistically significant difference in OKS or KSS functional scores between mobile- and fixed-bearing prostheses in their prospective study.24 A meta-analysis conducted by Zhang et al. also reported that mobile-bearing prostheses did not demonstrate a functional advantage over fixed-bearing implants in terms of KSS scores.25 The slightly lower functional score in our cohort may be attributed to patient profile, comorbidities, or variations in rehabilitation protocols.
The mean Visual Analog Scale (VAS) score for pain in our study was 3.58, suggesting that mobile-bearing prostheses provide an acceptable level of postoperative pain relief. However, this score is somewhat higher than those reported in similar studies. For instance, Ruckenstuhl et al. reported a mean VAS score of 2.1 in the mobile-bearing group, with no significant difference from fixed-bearing implants.24 Although individual pain perception, psychological status, or inclusion of patients with rheumatologic conditions may have contributed to the higher score in our series, this relatively elevated VAS value highlights a potential area for improvement. Future studies investigating patient-related and perioperative factors affecting pain perception could help optimize outcomes and guide patient selection and postoperative care protocols in mobile-bearing total knee arthroplasty.
Limitations
The principal limitation of our study lies in its retrospective design. Additionally, the relatively short follow-up period limits our ability to assess the long-term durability and potential late complications associated with LRMB implants. Nevertheless, the early clinical and radiological outcomes appear promising. Future prospective studies with extended follow-up durations will be essential to validate these preliminary findings and determine the long-term performance of LRMB systems.
Conclusion
In this retrospective study, total knee arthroplasty using a limited-rotation mobile-bearing prosthesis demonstrated satisfactory short-term clinical and radiological outcomes. Functional assessments, including OKS and KSS scores, indicated adequate joint performance, while postoperative range of motion exceeded the functional threshold. Although pain levels were generally acceptable, the relatively higher VAS scores observed in our cohort suggest that further investigation is warranted to optimize pain management and identify contributing factors. These findings support the use of mobile-bearing designs as a viable option in total knee arthroplasty, though patient selection, perioperative care, and rehabilitation strategies may influence outcomes and should be the focus of future prospective studies.
Declarations
Ethics Declarations
Ethical approval was obtained from the Non-Interventional Clinical Research Ethics Committee of Kayseri City Hospital (Date: 2024-05-28; No: 100). All data were anonymized prior to analysis, and the study was conducted in accordance with the Declaration of Helsinki and its later amendments.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee.
Informed Consent
Written informed consent was obtained from all participants prior to surgery.
Data Availability
The data are available from the corresponding author upon reasonable request and are not publicly available due to patient privacy.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Author Contributions (CRediT Taxonomy)
Conceptualization: K.Ö., K.H.
Methodology: K.Ö., K.H.
Investigation: K.Ö., K.H.
Data curation: K.Ö.
Formal analysis: K.Ö., K.H.
Writing – original draft: K.Ö.
Writing – review & editing: K.Ö., K.H.
Supervision: K.H.
Final approval of the manuscript: All authors
Scientific Responsibility Statement
The authors declare that they are responsible for the scientific content of the article, including study design, data collection, analysis and interpretation, writing, critical revision, and approval of the final version.
Abbreviations
CPM: Continuous Passive Motion
FB: Fixed-Bearing
G*Power: (Statistical power analysis software)
KSS: Knee Society Score
LRKMB: Limited-Rotation Knee Mobile-Bearing (as used in text)
LRMB: Limited-Rotation Mobile-Bearing
MANOVA: Multivariate Analysis of Variance
MB: Mobile-Bearing
OKS: Oxford Knee Score
pVAS: Pain Visual Analog Scale
PS: Posterior-Stabilized
ROM: Range of Motion
SPSS: Statistical Package for the Social Sciences (IBM SPSS Statistics)
TKA: Total Knee Arthroplasty
TKP: Total Knee Prosthesis
VAS: Visual Analog Scale
WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index
References
-
Bachmann M, Bolliger L, Ilchmann T, Clauss M. Long-term survival and radiological results of the Duracon™ total knee arthroplasty. Int Orthop. 2014;38(4):747-752. doi:10.1007/s00264-013-2154-4
-
Bae DK, Song SJ, Heo DB, Lee SH, Song WJ. Long-term survival rate of implants and modes of failure after revision total knee arthroplasty by a single surgeon. J Arthroplasty. 2013;28(7):1130-1134. doi:10.1016/j.arth.2012.08.021
-
Hao D, Wang J. Fixed-bearing vs mobile-bearing prostheses for total knee arthroplasty after approximately 10 years of follow-up: a meta-analysis. J Orthop Surg Res. 2021;16(1):437. doi:10.1186/s13018-021-02560-w
-
Chen P, Huang L, Zhang D, Zhang X, Ma Y, Wang Q. Mobile Bearing versus Fixed Bearing for Total Knee Arthroplasty: Meta-analysis of Randomized Controlled Trials at Minimum 10-Year Follow-up. J Knee Surg. 2022;35(2):135-144. doi:10.1055/s-0040-1713356
-
van der Voort P, Pijls BG, Nouta KA, Valstar ER, Jacobs WCH, Nelissen RGH. A systematic review and meta-regression of mobile-bearing versus fixed-bearing total knee replacement in 41 studies. Bone Joint J. 2013;95-B(9):1209-1216. doi:10.1302/0301-620X.95B9.30386
-
Sohn S, Koh IJ, Kim MS, Choi KY, Lim DS, In Y. Mobile-Bearing has no Benefit Over Fixed-Bearing Total Knee Arthroplasty in Joint Awareness and Crepitus: A Randomized Controlled Trial. J Arthroplasty. 2023;38(1):78-84. doi:10.1016/j.arth.2022.07.021
-
Capella M, Dolfin M, Saccia F. Mobile bearing and fixed bearing total knee arthroplasty. Ann Transl Med. 2016;4(7):127. doi:10.21037/atm.2015.12.64
-
Sehat K, Devane P, Horne G. Fixed bearing or mobile bearing total knee arthroplasty? A review of the recent literature. Curr Opin Orthop. 2007;18(1):66-70. doi:10.1097/BCO.0b013e3280119624
-
Kim YH, Kim JS. Comparison of anterior-posterior-glide and rotating-platform low contact stress mobile-bearing total knee arthroplasties. J Bone Joint Surg Am. 2004;86(6):1239-1247. doi:10.2106/00004623-200406000-00017
-
Powell AJ, Crua E, Chong BC, Gordon R, McAuslan A, Pitto RP, Clatworthy MG. A randomized prospective study comparing mobile-bearing against fixed-bearing PFC Sigma cruciate-retaining total knee arthroplasties with ten-year minimum follow-up. Bone Joint J. 2018;100-B(10):1336-1344. doi:10.1302/0301-620X.100B10.BJJ-2017-1450.R1
-
Migliorini F, Maffulli N, Cuozzo F, Pilone M, Elsner K, Eschweiler J. No difference between mobile and fixed bearing in primary total knee arthroplasty: a meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2022;31(2):655-663. doi:10.1007/s00167-022-07065-5
-
Khalifa AA, Fayez M, Elkady H, Abdelaal AM, Elassal MA. The outcome of posterior-stabilized, rotating platform total knee arthroplasty at a minimum ten-year follow-up: a Middle East institution experience. J Clin Orthop Trauma. 2022;26:101768. doi:10.1055/s-0040-1716850
-
Heckmann ND, Steck T, Sporer SM, Meneghini RM. Conforming polyethylene inserts in total knee arthroplasty: beyond the posterior-stabilized and cruciate-retaining debate. J Am Acad Orthop Surg. 2021;29(22):e1097-e1104. doi:10.5435/JAAOS-D-20-01232
-
Kahlenberg CA, Chalmers B, Sun HJ, Mayman DJ, Westrich GH, Haas SB, Sculco PK. Polyethylene components in primary total knee arthroplasty: a comprehensive overview of fixed bearing design options. J Knee Surg. 2022;35(13):1401-1408. doi:10.1055/s-0041-1723981
-
Dalyan S, Ozan F, Altun İ, Kahraman M, Günay AE, Özdemir K. The influence of component rotational malalignment on early clinical outcomes in total knee arthroplasty. Cureus. 2022;14(2):e22444. doi:10.7759/cureus.22444
-
Schoutens C, Nolte PA, van Noort A. Traumatic anterior tibiofemoral dislocation of mobile-bearing total knee arthroplasty: two cases. Trauma Case Rep. 2025;56:101144. doi:10.1016/j.tcr.2025.101144
-
Haider H, Garvin K. Rotating platform versus fixed-bearing total knees: an in vitro study of wear. Clin Orthop Relat Res. 2008;466(11):2677-2685. doi:10.1007/s11999-008-0463-5
-
Kim YH, Kim DY, Kim JS. Simultaneous mobile- and fixed-bearing total knee replacement in the same patients: a prospective comparison of mid-term outcomes using a similar design of prosthesis. J Bone Joint Surg Br. 2007;89(7):904-910. doi:10.1302/0301-620X.89B7.18635
-
Amaro JT, Arliani GG, Astur DC, Debieux P, Kaleka CC, Cohen M. No difference between fixed- and mobile-bearing total knee arthroplasty in activities of daily living and pain: a randomized clinical trial. Knee Surg Sports Traumatol Arthrosc. 2017;25(6):1692-1696. doi:10.1007/s00167-016-4106-1
-
Abdel MP, Tibbo ME, Stuart MJ, Trousdale RT, Hanssen AD, Pagnano MW. Infographic: fixed- versus mobile bearing total knee arthroplasty at ten years. Bone Joint J. 2018;100-B(7):923-924. doi:10.1302/0301-620X.100B7.BJJ-2018-0577
-
Baktir A, Karaaslan F, Yurdakul E, Karaoğlu S. Mobile- versus fixed-bearing total knee arthroplasty: a prospective randomized controlled trial featuring 6-10-year follow-up. Acta Orthop Traumatol Turc. 2016;50(1):1-9.
-
Kim YH, Park JW, Kim JS. Prospective randomized study of mobile- and fixed-bearing total knee replacements in patients younger than fifty-five years with osteoarthritis: a follow-up of minimum twenty years. J Bone Joint Surg Am. 2020;102(5):386-394.
-
Kim YH, Choi Y, Kim JS. Comparison of fixed-bearing and mobile-bearing total knee arthroplasties. Clin Orthop Relat Res. 2012;470(2):351-358.
-
Ruckenstuhl P, Revelant F, Hauer G, et al. No difference in clinical outcome, pain, and range of motion between fixed and mobile bearing Attune total knee arthroplasty: a prospective single-center trial. BMC Musculoskelet Disord. 2022;23(1):413. doi:10.1186/s12891-022-05382-x
-
Zhang Q, Zhang Y, Ma J, Liu Y, Pei F. Fixed-bearing vs mobile-bearing prostheses for total knee arthroplasty after approximately 10 years of follow-up: a meta-analysis. J Orthop Surg Res. 2021;16(1):383.
Figures
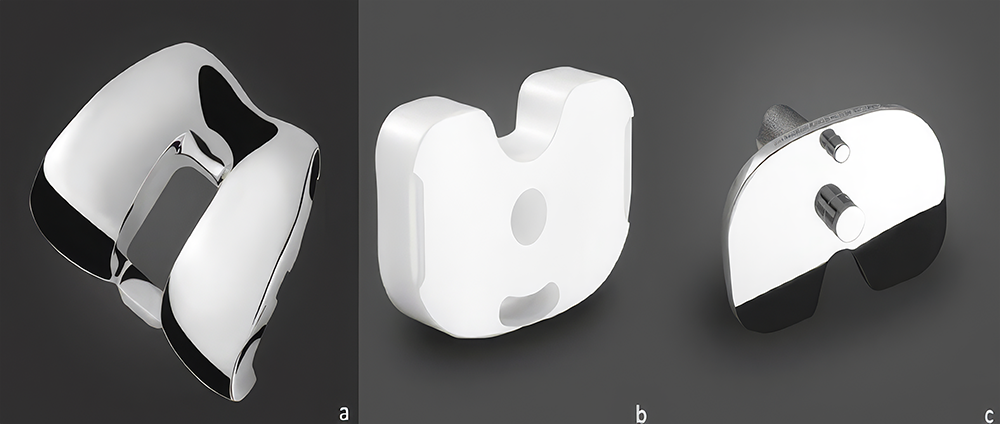
Figure 1. Bar charts of cross-tabulation for pre- and postoperative climbing stairs
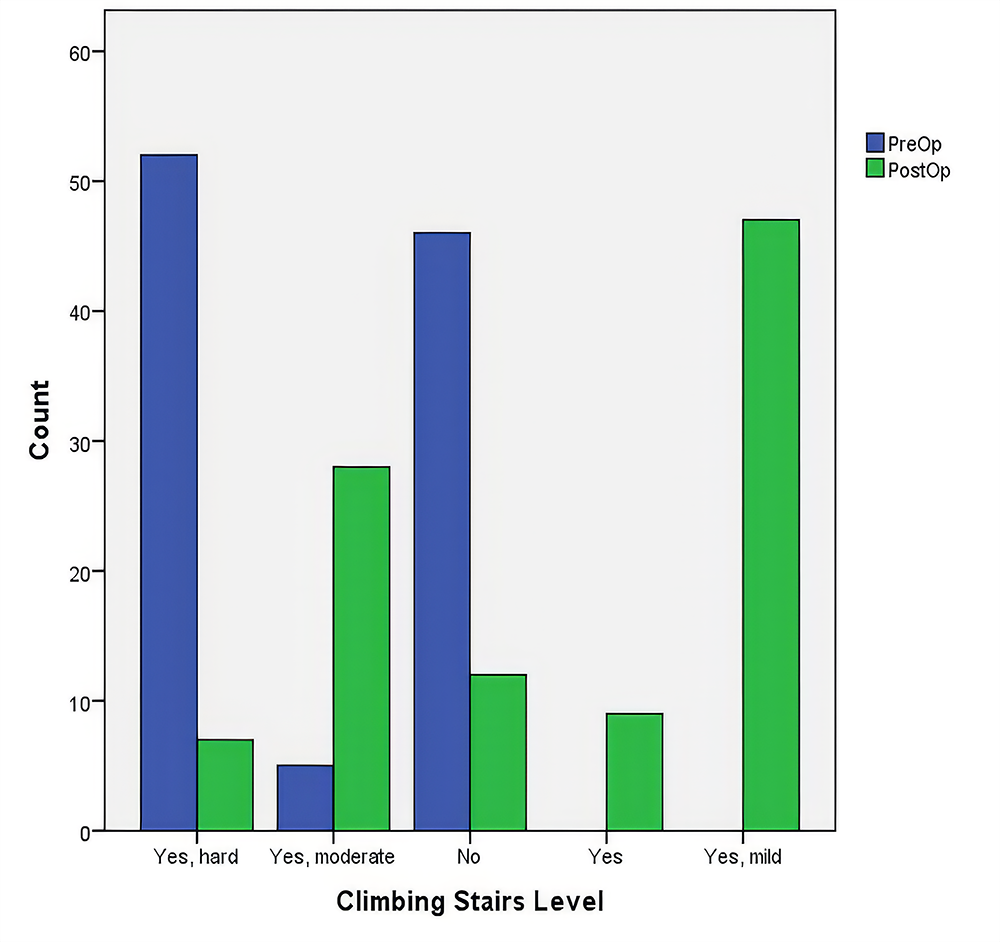
Figure 2. Scatter plot matrix displaying the correlation between changes in clinical variables (OKS, KSS Function, KSS Knee Score, and ROM)
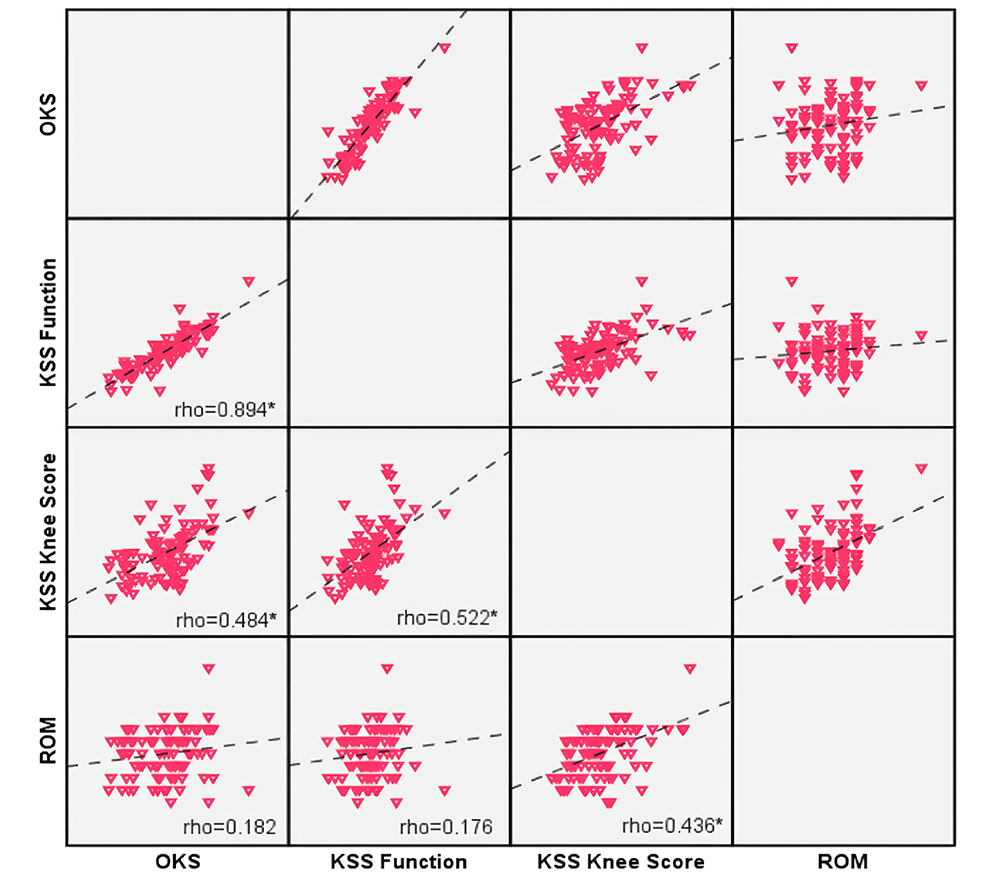
Figure 3
Tables
Table 1. Demographic data
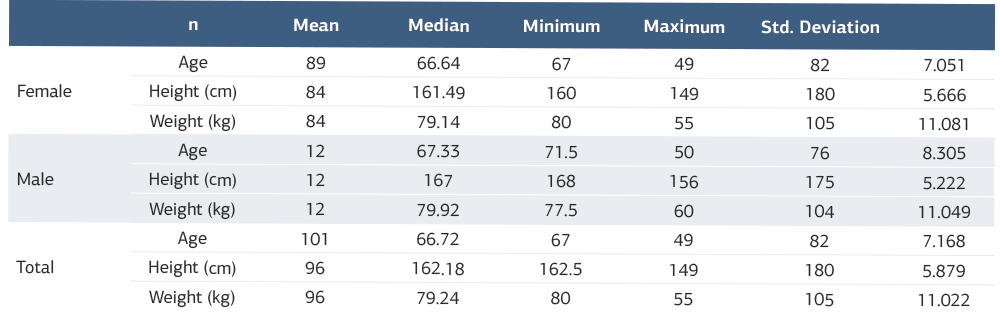
Table 2. Comparison of clinical measurements of patients
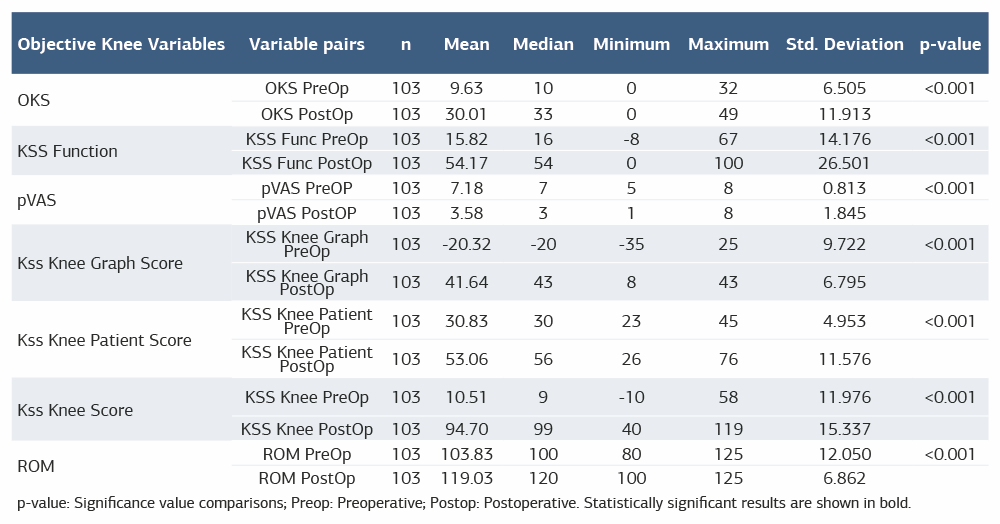
p-value: Significance value comparisons; Preop: Preoperative; Postop: Postoperative. Statistically significant results are shown in bold
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Koray Özdemir, Kazım Hüsrevoğlu Evaluation of the safety and efficacy of the limited rotation of the mobile-bearing posterior stabilised total knee prosthesis: a retrospective study. Ann Clin Anal Med 2026;17(3):203-209
- Received:
- April 12, 2025
- Accepted:
- May 2, 2025
- Published Online:
- June 23, 2025
- Printed:
- March 1, 2026