
Could microRNA-146a and microRNA-223 serve as biomarkers for predicting disease activity in rheumatoid arthritis patients?
Microrna-146a and microrna-223 as ra biomarkers
Authors
Abstract
Aim This study aimed to investigate the potential utility of circulating microRNA-146a and microRNA-223 as biomarkers for assessing disease activity in patients with rheumatoid arthritis (RA).
Methods Serum levels of miRNA-146a and miRNA-223 were measured in 60 RA patients and 30 healthy controls. Disease activity was assessed using the Disease Activity Score 28 (DAS28). Patients were stratified into two groups based on their treatment regimen: 30 patients on conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) and 30 patients on biologic disease-modifying antirheumatic drugs (bDMARDs). The expression levels of miRNA-146a and miRNA-223 were assessed by real-time polymerase chain reaction (RT-PCR).
Results In patients with RA, there was a significant overexpression of miRNA-146a compared to healthy controls (p<0.05). The Area Under the Curve (AUC) for miRNA-146a in serum was 0.679 (95% confidence interval (CI): 0.572-0.774, p<0.001), indicating its diagnostic potential. ROC curve analysis revealed that miRNA-146a had a sensitivity of 66.67% and a specificity of 70%. Both miRNA-146a and miRNA-223 levels were found to be highest in patients with high disease activity, and their elevated levels were strongly associated with elevated CRP and DAS28 scores, both of which are indicators of systemic inflammation and disease activity in RA.
Conclusion MiRNA-146a and miRNA-223 are valuable biomarkers for assessing disease activity in RA, particularly miRNA-146a, which demonstrated good diagnostic performance.
Keywords
Introduction
Rheumatoid arthritis (RA) is one of the most common systemic autoimmune diseases, affecting approximately 0.5-1% of the global population.1 Although the exact mechanisms underlying RA are not yet fully understood, various immune cells, such as T and B lymphocytes, macrophages, synovial fibroblasts, and neutrophils, are known to play key roles in its pathogenesis.2 The disease course in RA is highly variable, characterized by episodic flares and chronic inflammation in the synovial joints, which can lead to irreversible joint damage and significant physical and psychological dysfunction if not treated early and effectively.3 Therefore, early diagnosis is extremely critical for halting disease progression, preventing disability, and preserving patients’ quality of life. Although a few autoantibodies have been identified as biomarkers for RA, their sensitivity and specificity are limited. The most commonly used markers in clinical practice are rheumatoid factor (RF) and anti- citrullinated protein antibodies (ACPA), with antibodies against mutant citrullinated vimentin (MCV) also serving as useful alternatives.4 Despite their utility, these biomarkers are not ideal for detecting RA at its earliest stages or for accurately assessing disease activity. Therefore, there is a need for new biomarkers with higher sensitivity and specificity to improve both diagnosis and disease monitoring. Recent advances in early diagnosis and treatment have significantly improved the clinical management of RA, helping to prevent joint damage and systemic complications. Disease-modifying antirheumatic drugs (DMARDs) are the cornerstone of treatment, including conventional synthetic DMARDs (csDMARDs), biologic DMARDs (bDMARDs), and targeted synthetic DMARDs (tsDMARDs). However, the development of more sensitive biomarkers remains an essential goal for improving early diagnosis and personalized treatment.
Epigenetic modifications play a crucial role in the development of RA and influence disease activity and severity.5 MicroRNAs (miRNAs) are small non-coding RNA molecules typically 20-22 nucleotides in length that regulate a wide range of cellular processes.6 While their primary function is to modulate gene expression at the post-transcriptional level, miRNAs also control other non-coding RNAs.7 These molecules are critical in regulating immune responses by targeting various molecules, including transcription factors, cytokines, chemokines, and key signaling proteins. Aberrant miRNA expression, whether upregulated or downregulated, can contribute to the pathogenesis of a variety of diseases, including autoimmune disorders like RA, cancer, cardiovascular diseases, and neuropsychiatric conditions.8 Some studies have shown that the expression of several specific miRNAs is dysregulated in RA and is associated with chronic inflammation.5 Notably, many miRNAs, once detectable only in tissues and cells, can now be isolated from extracellular body fluids such as plasma, serum, saliva, and urine.9,10 The levels and composition of these extracellular miRNAs may correlate with specific diseases and pathological states, making them promising candidates as biomarkers for assessing disease activity, progression, and prognosis in RA.11
MicroRNAs play a critical role in regulating immune responses, immune cell development, and autoimmunity, suggesting their involvement in the pathogenesis of autoimmune diseases like RA, Sjögren’s syndrome, and systemic lupus erythematosus (SLE).12,13 For example, miRNA-146a is a key negative feedback regulator of the innate immune response and autoimmunity.14 Fibroblast-like synoviocytes (FLS), along with other immune cells, are central to RA development. These cells can release exosomes and other factors that influence RA onset and progression.15 Studies have shown that miRNAs such as miRNA-146 and miRNA-155 are highly expressed in RA synovial fibroblasts compared to those from osteoarthritis. miRNA-146 is predominantly expressed in CD68+ macrophages, some CD3+ T-cell subsets, and CD79a+ B-cells in RA synovial tissue.16 High levels of miRNA-146a and miRNA-16 correlate with active RA, while low levels are associated with disease remission.17 Additionally, miRNA-223 is overexpressed in RA synovial tissue, and its silencing has been shown to reduce disease severity in experimental arthritis models.18 Given these findings, we sought to determine whether serum levels of miRNA-223 and miRNA-146a could serve as diagnostic biomarkers for RA, correlate with disease activity, and potentially reflect treatment response.
Materials and Methods
Study Subjects and PatientsThis cross-sectional study included 90 participants: 60 patients who presented to the rheumatology department between 27.11.2015 - 01.03.2016 and who were diagnosed with RA according to the 2010 College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria 19 and 30 healthy individuals over 18 years of age. Of the 60 patients, 30 were on csDMARDs and 30 on bDMARDs. CsDMARD group; consisted of patients receiving methotrexate (MTX) monotherapy, a combination of MTX with other csDMARD(s), or csDMARD monotherapy or in combination. On the other hand, the bDMARD group included patients treated with bDMARDs with or without MTX and Janus kinase (JAK) inhibitors, with or without MTX.
This clinical study was approved by the local ethics committee. The study was conducted in adherence to the tenets of the Declaration of Helsinki. Prior to the study, all patients were informed about the purpose of the study and gave consent.
Clinical Variables and Disease Activity-Swollen joint count (SJC) and tender joint count (TJC) on 46 joints.
-Distribution of swollen and tender joints on 46 joint counts.
-Symmetrical swelling was observed in the metacarpophalangeal joints (MCPs), proximal interphalangeal joints (PIPs), wrists, metatarsophalangeal joints (MTPs), knees, ankles, and elbows. C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR).
-Investigator’s global assessment of disease activity (IGA).
-Patient-reported outcomes (PROs) such as pain, fatigue, and
-Patient Global Assessment (PGA).
-Self-reported functional capacity according to the Stanford
-Health Assessment Questionnaire (HAQ).
-Modified Larson score.
-Disease Activity Score 28-joint count (DAS28) was used to assess disease activity.
Total RNA ExtractionTotal RNA was isolated from serum samples (200 μl per sample) of 60 RA patients and 30 controls using a miRNeasy Serum/Plasma Kit (Qiagen, Hilden, Germany), following the manufacturer’s protocols. RNA was isolated from the required blood samples using an RNA extraction kit. RNA extraction from all blood samples was performed according to the steps outlined in Figure 1.
RNA to cDNA conversion and real-time Polymerase Chain Reaction (RT-PCR) analysis of plasma samples.
The extracted RNA was stored under appropriate conditions, and cDNA synthesis was initiated. cDNA synthesis was performed using the Qiagen miScript Reverse Transcription (RT) Kit II (Hilden, Germany). The cDNAs were amplified using the Qiagen miScript PreAMP PCR Kit (Hilden, Germany). After cDNA extraction, the RT-PCR step was started to analyze the expression levels of miRNA-146a and miRNA-223. The reaction components for RT-PCR were prepared using the Qiagen miScript SYBR Green PCR kit. SNORD61 served as the normalization control for RT-PCR. RT-PCR Rotor-Gene Q (Qiagen) was used to identify SNORD61 expression levels as a reference, along with the hsa-miRNA-146-3p and hsa-miRNA- 3p miRNA primers.
Calculation of Gene Expression of miRNAsChanges in miRNA-146a and miRNA-223 expression levels were calculated. The delta Ct (Cycle threshold) values were determined using SNORD61 as a reference miRNA. The Ct values obtained from the real-time PCR analysis were recorded in Excel for further analysis.
Ethical ApprovalThis study was approved by the Ethics Committee of Firat University Faculty of Medicine (Date: 2015-10-27, No: 19/02).
Statistical AnalysisStatistical analysis was performed using the Statistical Package for Social Sciences for Windows (SPSS) 22.0. Categorical measures were expressed as numbers and percentages, and numerical measures were expressed as means ± standard deviations. The Mann-Whitney U test was used to compare non-normally distributed numerical data between two groups, and the Kruskal-Wallis test was used to compare means between three or more groups. An independent samples t-test was used to compare normally distributed data between two groups, while one-way ANOVA was used to compare means between three or more groups. The odds ratio (OR) with a 95% confidence interval (CI) was used to report the strength of association. Spearman’s and Pearson’s correlation tests were used for correlation analysis. A p-value of p<0.05 was considered statistically significant.
Reporting GuidelinesThis study is reported in accordance with the STROBE guidelines.
Results
Sociodemographic and Clinical Characteristics of PatientsThe mean age was 56±13.1 years in the cDMARD group (8 men, 22 women), 51±12.4 years in the bDMARD group (7 men, 23 women), and 50.5±15.5 years in the control group (11 men, 34 women).
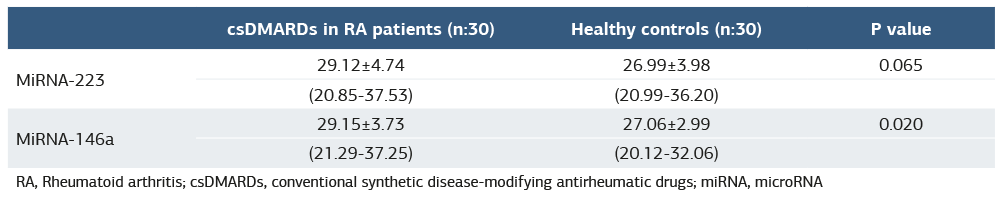
Serum Levels of miRNA-146a and miRNA-223The mean serum miRNA-146a and miRNA-223 levels of RA patients using csDMARDs were compared with the miRNA-146a and miRNA-223 levels of healthy controls and are shown in Table 1. Expression levels of miRNA-146a are independently increased in RA patients compared to healthy controls (p<0.05). The mean serum levels of miRNA-146a and miRNA-223 in RA patients treated with bDMARDs were compared to those in healthy controls, as presented in Table 2. Additionally, no significant difference was observed between the csDMARDs group and the bDMARDs group in serum levels of miRNA-146a and miRNA-223 (p=0.516; p=0.473).
In this study, the cut-off value for serum miRNA-146a was determined to be 28.10 ng/ml, with a sensitivity of 66.7% and a specificity of 63.3%. For serum miRNA-223, the cut-off value was 27.56 ng/ml, with a sensitivity of 58.3% and a specificity of 56.7%.
Predictive Values of miRNA-146a and miRNA-223 in RAThe AUC for serum miRNA-146a in predicting RA was 0.679 (95% CI: 0.572–0.774, p<0.001), while the AUC for serum miRNA-223 was 0.588 (95% CI: 0.479–0.691, p=0.155) (Table 3).
ROC analysis showed that miRNA-146a had a sensitivity of 66.67% and specificity of 70% in association with RA (Figure 2A). For miRNA-223, the sensitivity was 51.67% and the specificity was 91% (Figure 2B). The cut-off values were 28.10 ng/ml for serum miRNA-146a and 27.56 ng/ml for serum miRNA-223.
Correlating Serum miRNA-146a and miRNA-223 with Disease ActivityIn all RA patients, DAS28 levels were positively correlated with miRNA-146a (r=0.468, p<0.001; Figure 3A) and miRNA-223 levels (r=0.404, p<0.001; Figure 3B). In the csDMARDs group, a positive correlation was observed between miRNA-146a (r=0.465, p<0.001) and miRNA-223 levels (r=0.353, p=0.001)
with the TJC on a 46-joint count. Expression levels of miRNA- 146a and miRNA-223 were also significantly associated with CRP levels. Additionally, in all subjects, miRNA-146a levels correlated with IGA (r=0.330, p=0.001), PROs such as pain (r=0.308, p=0.003), fatigue (r=0.444, p<0.001), PGA severity (r=0.308, p<0.001), and the modified Larson score (r=0.282, p=0.007). No significant associations were found between miRNA-223 levels and these parameters.
Discussion
This study was limited by its single-center design and relatively small sample size. Additionally, the absence of early treatment- naïve RA patients may have influenced the diagnostic performance of the studied biomarkers.
Rheumatoid arthritis is characterized by chronic synovial membrane inflammation, which can destroy cartilage and bone.20 Early diagnosis and treatment are important to prevent and reduce the complications of RA. Although ACPA and, to a lesser extent, rheumatoid factor are biomarkers with high sensitivity and specificity, they are inadequate biomarkers for monitoring response to treatment and tracking disease activity. The identification of additional biomarkers is therefore one of the most challenging issues in RA research. We showed that expression levels of miRNA-146a are independently increased in RA patients compared to healthy controls, and miRNA-146a levels correlated with CRP, DAS28, TJC, IGA, PROs such as pain and fatigue, PGA severity, and the modified Larson score.
In RA, early diagnosis can be challenging due to the absence of typical clinical and laboratory findings in the disease’s initial stages. To address this, researchers are focusing on identifying novel diagnostic and prognostic biomarkers. An ideal biomarker should be highly specific to the disease, detectable before clinical symptoms appear, and capable of reflecting ongoing inflammation, even in patients undergoing treatment that may alter the disease course. MicroRNAs exhibit many qualities of effective biomarkers. Unlike protein-based biomarkers, which may undergo post-translational modifications affecting measurement accuracy, miRNAs are relatively homogeneous.21 Although most miRNAs are intracellular, some are found in the extracellular compartment. In a study by Jessica A. and colleagues, multiple miRNAs were detected in 12 different types of body fluids, with notable differences in composition and concentration.22 While the role of extracellular miRNAs is not fully understood, their presence in exosomes suggests they may participate in cell-to-cell communication.23 This opens new avenues for biomarker discovery and miRNA-based therapeutic approaches. At the same time, PCR can easily detect most circulating miRNAs. In recent years, there have been significant advancements in our understanding of the role of miRNAs in various physiological processes and their application in clinical biochemistry, thanks to a growing body of research. MiRNAs may play a role in the development of autoimmune diseases when their regulatory effect on maintaining immune homeostasis and normal immune function is impaired.24
MiRNA-146a-5p plays a crucial role in the differentiation and function of both innate and adaptive immune cells.16 In 2008, Nakasa T. et al. reported that miRNA-146a was expressed in various cell types in synovial tissues, including synovial fibroblasts, macrophages, T cells, and B cells, after TNFα stimulation in RA patients, and they also reported miRNA-146 expression in CD3+ cells, suggesting that miRNA-146 may contribute to persistent inflammation in RA through a T cell network.16 In another similar study, synovial miRNA- 146a and miRNA-223 expression levels were independently associated with RA.24 The results of this study revealed a significant increase in the relative expression of miRNA-146a in RA patients compared to healthy controls, consistent with previous research findings. When evaluating whether miRNA- 146a could serve as a diagnostic marker for RA, our study found the highest AUC to be 0.679, with 66.7% sensitivity and 70% specificity. In comparison, Safari F. et al. reported a higher AUC of 0.8 for miRNA-146a, achieving 96% sensitivity and 86% specificity among miRNAs.24 The slightly lower sensitivity and specificity in our study may be attributed to the absence of early-diagnosed and treatment-naïve patients in the sample population. Overall, these findings suggest that miRNA-146a has potential as a biomarker for the diagnosis of RA.
Limitations
This study has several limitations. Firstly, it was conducted in a single center with a relatively small sample size, which may limit the generalizability of the findings. Secondly, the study population did not include treatment-naïve or early-stage RA patients, which may have affected the diagnostic accuracy of the investigated miRNAs. Additionally, the cross-sectional design precludes causal inferences between miRNA levels and disease activity or treatment response. Future prospective studies with larger and more diverse patient populations are needed to validate these findings and evaluate the prognostic utility of circulating miRNA-146a and miRNA-223 in RA.
Conclusion
Our study demonstrates that circulating miRNA-146a levels are significantly elevated in RA patients and are positively correlated with disease activity parameters, particularly DAS28, CRP, and patient-reported outcomes. Although miRNA-223 showed a similar trend, its diagnostic performance was less robust. These findings support the potential utility of miRNA- 146a as a biomarker for disease activity monitoring in RA, paving the way for further validation studies in larger and more diverse patient populations.
Declarations
Ethics Declarations
The study protocol was reviewed and approved by the institutional ethics committee, and all procedures were conducted in accordance with the Declaration of Helsinki and its later amendments.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants prior to enrollment in the study.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: U.B., A.G.
Methodology: U.B., G.A.
Investigation: A.K., A.S., D.E.
Data curation: T.I.D., Y.G.
Formal analysis: Y.G.
Writing – original draft: U.B.
Writing – review & editing: A.G., G.A., A.S.
Supervision: U.B.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article
Abbreviations
ACPA: Anti-Citrullinated Protein Antibody
ACR: American College of Rheumatology
AUC: Area Under the Curve
bDMARDs: Biologic Disease-Modifying Antirheumatic Drugs
CRP: C-Reactive Protein
csDMARDs: Conventional Synthetic Disease-Modifying Antirheumatic Drugs
DAS28: Disease Activity Score 28
ESR: Erythrocyte Sedimentation Rate
HAQ: Health Assessment Questionnaire
IGA: Investigator Global Assessment
miRNA: MicroRNA
MCP: Metacarpophalangeal
MTP: Metatarsophalangeal
PCR: Polymerase Chain Reaction
PGA: Patient Global Assessment
PIP: Proximal Interphalangeal
PROs: Patient-Reported Outcomes
RA: Rheumatoid Arthritis
RT-PCR: Real-Time Polym
References
-
Almutairi K, Nossent J, Preen D, Keen H, Inderjeeth C. The global prevalence of rheumatoid arthritis: a meta-analysis based on a systematic review. Rheumatol Int. 2021;41(5):863–877. doi:10.1007/s00296-020-04731-0
-
Deng GM, Lenardo M. The role of immune cells and cytokines in the pathogenesis of rheumatoid arthritis. Drug Discov Today Dis Mech. 2006;3(2):163–168.
-
Casey J. Anti-MCV antibodies—A promising new biomarker for RA. Nat Rev Rheumatol. 2009;5(4):179.
-
Araki Y, Mimura T. The mechanisms underlying chronic inflammation in rheumatoid arthritis from the perspective of the epigenetic landscape. J Immunol Res. 2016;2016:6290682. doi:10.1155/2016/6290682
-
Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell. 2004;116(2):281–297. doi:10.1016/s0092-8674(04)00045-5
-
Filipowicz W, Bhattacharyya SN, Sonenberg N. Mechanisms of post- transcriptional regulation by microRNAs: are the answers in sight? Nat Rev Genet. 2008;9(2):102–114. doi:10.1038/nrg2290
-
Sun BK, Tsao H. Small RNAs in development and disease. J Am Acad Dermatol. 2008;59(5):725–737. doi:10.1016/j.jaad.2008.08.017
-
Cortez MA, Calin GA. MicroRNA identification in plasma and serum: a new tool to diagnose and monitor diseases. Expert Opin Biol Ther. 2009;9(6):703–711. doi:10.1517/14712590902932889
-
Park NJ, Zhou H, Elashoff D, et al. Salivary microRNA: discovery, characterization, and clinical utility for oral cancer detection. Clin Cancer Res. 2009;15(17):5473–5477. doi:10.1158/1078-0432.CCR-09-0736
-
Gilad S, Meiri E, Yogev Y, et al. Serum microRNAs are promising novel biomarkers. PLoS One. 2008;3(9):e3148.
-
Pauley KM, Cha S, Chan EK. MicroRNA in autoimmunity and autoimmune diseases. J Autoimmun. 2009;32(3–4):189–194.
-
Alevizos I, Alexander S, Turner RJ, Illei GG. MicroRNA expression profiles as biomarkers of minor salivary gland inflammation and dysfunction in Sjögren’s syndrome. Arthritis Rheum. 2011;63(2):535–544.
-
Chan EK, Ceribelli A, Satoh M. MicroRNA-146a in autoimmunity and innate immune responses. Ann Rheum Dis. 2013;72(Suppl 2):ii90–5.
-
Stanczyk J, Pedrioli DM, Brentano F, et al. Altered expression of microRNA in synovial fibroblasts and synovial tissue in rheumatoid arthritis. Arthritis Rheum. 2008;58(4):1001–1009.
-
Nakasa T, Miyaki S, Okubo A, et al. Expression of microRNA-146 in rheumatoid arthritis synovial tissue. Arthritis Rheum. 2008;58(5):1284–1292.
-
Pauley KM, Satoh M, Chan AL, Bubb MR, Reeves WH, Chan EK. Upregulated miR-146a expression in peripheral blood mononuclear cells from rheumatoid arthritis patients. Arthritis Res Ther. 2008;10(4):R101.
-
Li YT, Chen SY, Wang CR, et al. Brief report: amelioration of collagen-induced arthritis in mice by lentivirus-mediated silencing of microRNA-223. Arthritis Rheum. 2012;64(10):3240–3245.
-
Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581.
-
Etheridge A, Lee I, Hood L, Galas D, Wang K. Extracellular microRNA: a new source of biomarkers. Mutat Res. 2011;717(1–2):85–90.
-
Weber JA, Baxter DH, Zhang S, et al. The microRNA spectrum in 12 body fluids. Clin Chem. 2010;56(11):1733–1741.
-
Valadi H, Ekström K, Bossios A, Sjöstrand M, Lee JJ, Lötvall JO. Exosome- mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat Cell Biol. 2007;9(6):654–659.
-
Dai R, Ahmed SA. MicroRNA, a new paradigm for understanding immunoregulation, inflammation, and autoimmune diseases. Transl Res. 2011;157(4):163–179.
-
Furer V, Greenberg JD, Attur M, Abramson SB, Pillinger MH. The role of microRNA in rheumatoid arthritis and other autoimmune diseases. Clin Immunol. 2010;136(1):1–15.
-
Safari F, Damavandi E, Rostamian AR, et al. Plasma levels of microRNA-146a- 5p, microRNA-24-3p, and microRNA-125a-5p as potential diagnostic biomarkers for rheumatoid arthritis. Iran J Allergy Asthma Immunol. 2021;20(3):326–337.
Figures
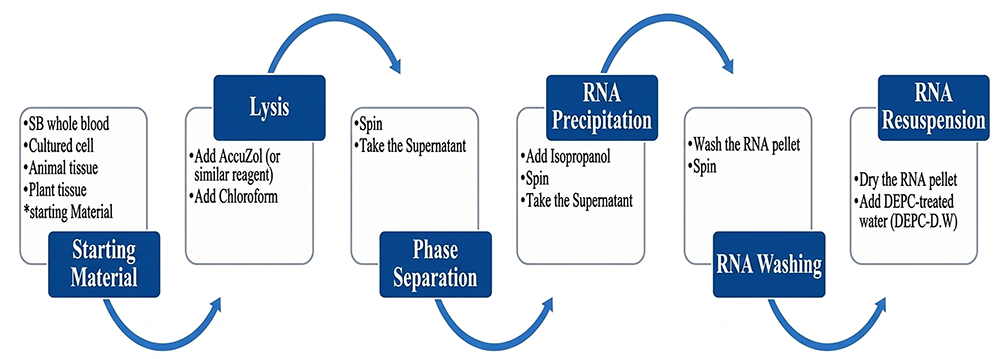
Figure 1. Total RNA Extraction
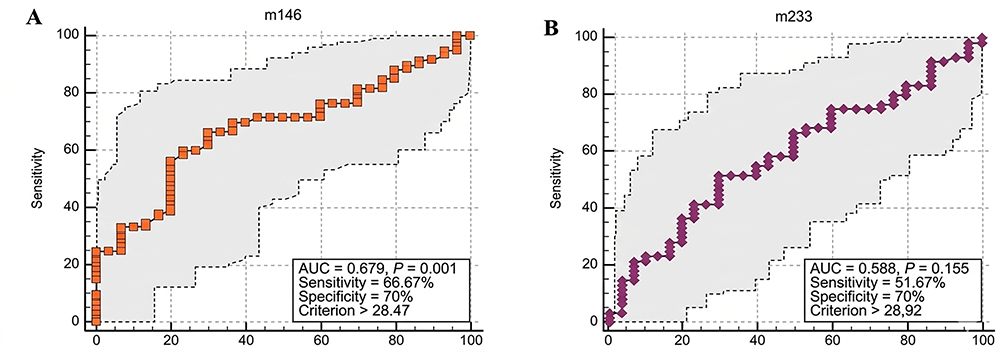
Figure 2. miRNA-146a and miR-223 exhibited upregulation in RA; however, the increase in miRNA-223 was not statistically significant. 2A: ROC analyses linked miRNA-146a and RA with a sensitivity of 66,67% and specificity of 70%, 2B: ROC analyses linked miRNA-223 and RA with a sensitivity of 51.67% and specificity of 70%
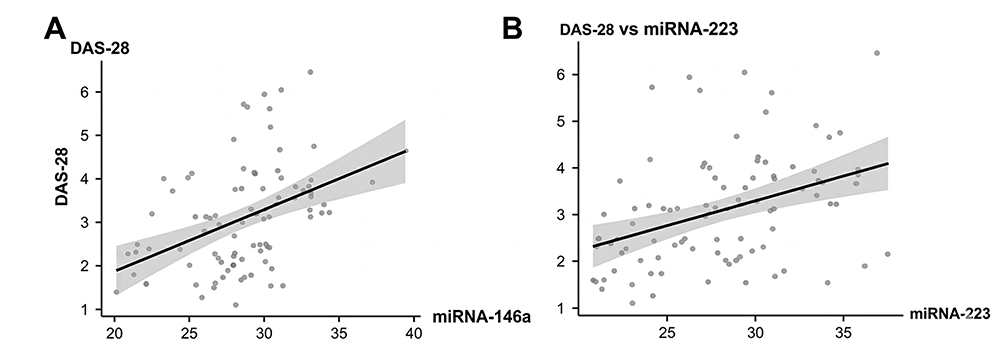
Figure 3. miRNA-146a and miRNA-223 are upregulated in rheumatoid arthritis and correlate with Disease Activity Score 28 (DAS28). 3A: DAS28 levels correlated with miRNA-146a levels in all study subjects (r=0.468, p<0.001), 3B: DAS28 levels correlated with miRNA-223 levels in all study subjects (r=0.404, p<0.001)
Tables
Table 1. Expression levels of miRNA-146a and miRNA-223 in serum from RA patients receiving cDMARDs compared to healthy controls
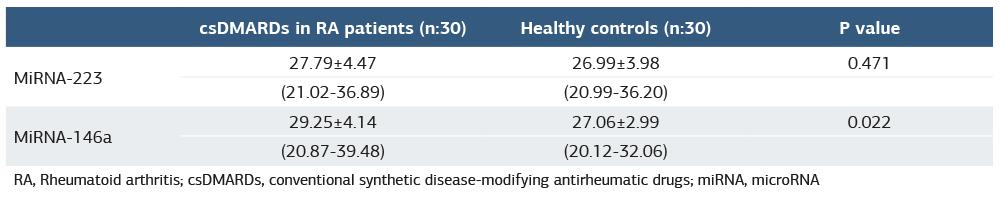
RA, Rheumatoid arthritis; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; miRNA, microRNA
Table 2. Expression levels of miRNA-146a and miRNA-223 in serum from RA patients receiving bDMARDs compared to healthy controls
RA, Rheumatoid arthritis; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; miRNA, microRNA
Table 3. Predictive values of miRNA-146a and miRNA 223 for RA

Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Umut Bakay, Arif Gulkesen, Aşkin Sen, Deniz Erol, Arzu Kaya, Tugba Izci Duran, Yunus Gural. Could microRNA-146a and microRNA-223 serve as biomarkers for predicting disease activity in rheumatoid arthritis patients? Ann Clin Anal Med 2026;17(Suppl 2):S135-140. doi: 10.4328/ACAM.22719
- Received:
- April 21, 2025
- Accepted:
- June 9, 2025
- Published Online:
- July 2, 2025
- Printed:
- March 20, 2026