
Association of breast cancer with different molecular subtypes and Ki67 proliferation with 18F-FDG PET/CT
18F-FDG PET/CT in breast cancer
Authors
Abstract
Aim The main molecular factors affecting the aggressiveness of breast cancer are estrogen receptor, progesterone receptor, and human epidermal growth factor-2. We wanted to study how molecular subtypes make a difference in tumor metabolism and staging in 18F-FDG PET/CT.
Methods Between 2023 and 2024, 110 patients with breast cancer who presented to our nuclear medicine clinic for staging were included in the study.
Results There was no statistically significant correlation between the molecular classification of the patients and the SUVmax levels of the primary breast tumor (p = 0.055). There was a significant correlation between breast molecular types and the presence of lymph node metastasis (p = 0.032). Triple-negative and Luminal B type patients had a higher risk of lymph node metastasis compared to other molecular subtypes. There was a significant correlation between Ki67 proliferation and molecular subtypes (p = 0.000). We also found a significant correlation between Ki67 index and breast tumor and lymph node SUVmax levels (p = 0.000, p = 0.03). There was a significant correlation between Ki67 proliferation and the presence of lymph node metastasis (p = 0.000).
Conclusion In the present study, we demonstrated that different molecular subtypes show different metabolic characteristics. We also revealed that tumor Ki67 levels cause metabolic differences, and tumors with high Ki67 levels on 18F-FDG PET/CT have an increased likelihood of lymph node metastasis. We think that Ki67 levels should be taken into consideration when interpreting lymph node positivity in these patients.
Keywords
Introduction
Breast cancer is the most common type of cancer in women and accounts for approximately 15.5% of cancer deaths in women 1. The main molecular factors affecting the aggressiveness of breast cancer are estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor-2 (HER-2) 2. Approximately 70% of breast cancers are ER-positive, and the majority of them also have a positive PT. The prognosis of this group of breast cancers is much better than the others 3. HER-2 positivity is associated with an extremely poor prognosis. These molecules determine the treatment option and prognosis 4. As treatment options are related to molecular subtypes, staging is also very important in treatment. Therefore, ultrasonography, mammography, computed tomography, and magnetic resonance imaging, which are traditional imaging methods, are used in the staging of breast cancer. However, the lack of whole-body imaging may lead to errors in staging and, therefore, errors in treatment selection.
Fluorine-18 (F18) fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) is a non-invasive functional imaging system used in the diagnosis, staging, and evaluation of response to treatment of various cancers 5. In addition to tumor staging, PET/CT imaging allows quantitative assessment of glucose metabolism 6. Although 18F-FDG PET/ CT imaging in breast cancer is recommended for stage IIB and stage III breast cancer in the SNNMI and EANM guidelines, it is not recommended for stage I 7. However, in a recent systematic review and meta-analysis by Han et al., it changed the initial stage in 25% of newly diagnosed breast cancer patients and changed the treatment management in 18 8.
We wanted to study how molecular subtypes make a difference in tumor metabolism and staging in 18F-FDG PET/CT.
Materials and Methods
Between 2023 and 2024, 110 patients who were diagnosed with breast cancer by biopsy and applied to our nuclear medicine clinic for staging were included in the study. PET/ CT imaging was performed at least 1 week after biopsy. In addition, the patients included in the study had not received any treatment for breast cancer and did not have any other concomitant malignancies.
Classification of Molecular SubtypesThe subtypes were classified by ER, PR, and HER-2 studies on tissues obtained from breast tumors by the Tru-Cut biopsy method. Molecular subtypes were divided into 4 classes as luminal A, luminal B, HER-2 positive, and triple negative.
Luminal A: estrogen receptor positive/progesterone receptor positive and HER-2 negative.
Luminal B: estrogen receptor±/progesterone receptor ± and c-erbB-2 ±.
HER-2 positive: estrogen receptor negative/progesterone receptor negative and HER-2 positive.
Triple negative: estrogen receptor negative/progesterone receptor negative and HER-2 negative.
8F-FDG PET/CT Imaging Protocol: The patients were asked to fast for at least 4-6 hours, and their blood glucose levels were measured before imaging was performed. Only patients with fasting blood glucose levels below < 200 mg/dL were injected with radiopharmaceuticals. During 18F-FDG PET/ CT examinations, the patients were administered an average of 10 mCi 18F-FDG. All the patients stayed in the relaxation room for 45-60 minutes after the injection. The General Electric Discovery PET/CT 600 device was used for imaging. CT imaging was performed with a spiral 16-slice scanner at 120 kV and 172 mAs for attenuation correction and anatomical correlation. Three-dimensional PET imaging was performed, covering the body parts from the skull to the proximal thigh. PET imaging was conducted for approximately 2 minutes in each bed position. Axial, coronal, and sagittal fusion images were created using the iterative reconstruction method. The maximum standardized uptake values (SUVmax) were calculated based on the PET images. An adaptive threshold setting of 42% of maximum regional metabolic activity was used for the PET images, and the region of interest (ROI) was placed within the primary tumor in the breast by avoiding the peripheral area.
The following formula was used to calculate the SUVmax: [Activity in ROI (mCi/mL) × Body Weight (grams)] ÷ Injected Dose (mCi)
Ethical ApprovalAn informed consent form was obtained from the patients for this study. This study was approved by the Ethics Committee of Tokat Gaziosmanpasa University (Date: 2025-05-27, No:15235480-050.04-579263).
Results
The mean age of the 110 patients included in the study was 54.18 years (range: 24-86). All patients had invasive ductal carcinoma breast cancer. Of the 110 patients, 66 (60%) had luminal type A, 25 (22.7%) had luminal type B, 12 (10.9%) had HER2-positive, and 7 (6.4%) had triple negative subtypes. There was no statistically significant correlation between the molecular classifications of the patients and the SUVmax levels of the primary breast tumor (p = 0.055) (Table 1). Although not statistically significant, the lowest SUVmax values were measured in the Luminal A group, while the highest SUVmax values were in the Triple negative group.
In 66 patients with Luminal type A breast tumors on PET/ CT, the median SUVmax value was 4.7 (range 1-20.5). In 30 Luminal type A patients with lymph node metastases, the median SUVmax value for metastatic lymph nodes was 4 (range: 1-16.8). Luminal type A 7 patients with distant metastases had a median SUVmax value of 6.4 (range: 1.5-15.2). In 27 patients with Luminal type B breast tumors on PET/CT, the median SUVmax value was 7 (range: 1-39.8). In 20 Luminal type B patients with lymph node metastases, the median SUVmax value for metastatic lymph nodes was 5.3 (range: 1-19.7). In 5 Luminal type B patients with distant metastases, the median SUVmax value for distant metastases was 4 (range: 3.3-9.7). The median SUVmax value of breast tumor on PET/CT of 12 HER2-positive patients was 7.35 (range 2.1-15.2). The median SUVmax value of metastatic lymph nodes in 7 HER2-positive patients with lymph node metastasis was 5.9 (range: 1.7- 12.9). In 2 HER2-positive patients with distant metastases, the median SUVmax value for distant metastases was 3.05 (range: 2-4.1). The median SUVmax value of breast tumor on PET/CT of 8 triple negative patients was 8.4 (range 4.1-13.2). In 5 triple-negative patients with lymph node metastases, the median SUVmax value for metastatic lymph nodes was 4.9 (range: 2.3- 10.2). The median SUVmax value of a 1 triple-negative patient with distant metastasis was 4. No significant correlation was found between breast cancer molecular subtypes and the SUVmax values of lymph node and distant metastases (p = 0.630, p = 0.593) (Table 1).
While 59 (89.4%) of 66 patients with luminal type A had no distant metastasis, 7 (10.6%) had distant metastasis. Luminal type B 20 (80%) of 25 patients had no distant metastasis, while 5 (20%) had distant metastasis. While 10 (83.3%) of 12 HER2-positive patients had no distant metastasis, 2 (16.7%) had distant metastasis. While 6 (85.7%) of 7 triple-negative patients had no distant metastasis, 1 (14.3%) had distant metastasis. No significant association was found between breast molecular subtypes and the presence of distant metastasis (p = 0.689). Of 66 patients with luminal type A, 37 (56.1%) had no lymph node metastasis, and 29 (43.9%) had lymph node metastasis. While 6 (24%) of 25 patients with luminal type B had no lymph node metastasis, 19 (76%) had lymph node metastasis. While 5 (41.7%) of 12 HER2-positive patients had no lymph node metastasis, 7 (58.3%) had lymph node metastasis. Of the 7 triple-negative patients, 2 (28.6%) had no lymph node metastasis, while 5 (71.4%) had lymph node metastasis. There was a significant association between breast molecular subtypes and the presence of lymph node metastasis (p = 0.032). The risk of lymph node metastasis was higher in triple-negative and Luminal B type patients compared to other molecular subtypes.
Ki67 proliferation index was less than 15% in 37 patients and more than 15% in 72 patients. The Ki67 index of 1 patient was not available. Of the 37 patients with Ki67 proliferation less than 15%, 34 (91.9%) had no distant metastasis, while 3 (8.1%) had distant metastasis. Of 72 patients with Ki67 proliferation greater than 15%, 60 (83.3%) had no distant metastasis, while 12 (16.7%) had distant metastasis. There was no significant correlation between i67 proliferation and the presence of distant metastasis (p = 0.219). Of 37 patients with Ki67 proliferation less than 15%, 8 (22%) had lymph node metastasis, while 29 (78%) had no lymph node metastasis. Of 72 patients with Ki67 proliferation greater than 15%, 21 (29%) had no lymph node metastasis, while 51 (71%) had lymph node metastasis. There was a significant correlation between Ki67 proliferation and the presence of lymph node metastasis (p = 0.000) (Table 2). Of 65 luminal type A patients, 33 (51%) had less than 15% Ki67 proliferation, and 32 (49%) had more than 15% Ki67 proliferation. Luminal type B was less than 15% in 3 (12%) and more than 15% in 22 (88%) of 25 patients. In 1 (8%) of 12 HER2- positive patients, Ki67 was less than 15% and in 11 (92%), Ki67 was more than 15%. In all 7 triple-negative patients (100%), Ki67 was more than 15%. There was a significant association between Ki67 proliferation and molecular subtypes (p = 0.000) (Table 2). We also found a significant correlation between Ki67 index and breast tumor and lymph node SUVmax levels (p = 0.000, p = 0.03).
Discussion
Breast cancer exhibits highly heterogeneous pathologic and molecular features. According to these characteristics, treatment modalities and prognosis of patients are determined. Breast tumors with different molecular subtypes may have different uptake levels of 18F-FDG in PET/CT.
In the present study, although we did not find a statistically significant relationship between molecular subtypes and SUVmax, according to our results, the highest tumor SUVmax was calculated in the triple negative subtype, while the lowest tumor SUVmax was calculated in the luminal A type. This is consistent with other studies in the literature. Akin et al. found that luminal type B and triple negative type breast cancer had higher SUVmax values than luminal type A 9. Oner et al. in their study, the breast tumor SUVmax value of luminal type B, HER-2 positive, and triple negative patients was higher than the SUVmax value of luminal type A patients 10. Consistent with the results of our study, Koo and Kitajima et al. also found lower SUVmax values in luminal type A patients compared to luminal type B and triple negative tumor SUVmax 11,12.
In the present study, there was a significant relationship between molecular subtypes and lymph node metastasis. In the study by Koo et al., lymph node involvement was found to be 1.67 times higher in HER-2 and triple negative patients compared to luminal type A patients. In our study, statistically significant triple-negative patients had the highest lymph node metastasis rate. 2. The highest probability of lymph node metastasis was found in HER2-positive patients. The lowest lymph node metastasis rate was in luminal type A patients 11. In addition, the incidence of lymph node metastasis was higher in patients with high Ki67 in our study. In the Aktaş et al. study, the lymph node SUVmax value was higher in patients with high Ki67 compared to those with low Ki67 13. Similar to the results of our study, Aktaş et al. found a significant correlation between primary tumor SUVmax and metastatic lymph node SUVmax values and molecular subtypes.
In contrast to our study, Topuz et al. did not find a significant correlation between breast tumor and lymph node SUVmax and Ki67. We found a significant correlation between Ki67 elevation and the frequency of lymph node metastasis. Topuz et al. did not find a significant correlation between Ki67 and axillary lymph node involvement in their study 14. Shen et al. also found a significant correlation between breast tumor SUVmax and elevated Ki67 15.
Consistent with the results of our study, Li et al. also found a relationship between Ki67 elevation and molecular subtypes 16. In George et al.’s study, as in our study, the highest rate of Ki67 elevation was observed in triple negative patients and the lowest in the luminal type A group 17. No significant correlation was found between Ki67 and the presence of lymph node metastasis in Tuzcu et al. However, in our study, there was a significant correlation between Ki67 elevation and lymph node metastasis 18.
Limitations
We could not perform a prognosis study because our study was retrospective. Although the 8th edition of the American Joint Committee on Cancer (AJCC) staging guidelines does not include 18F-FDG hypermetabolism as a prognostic factor in breast cancer, increasing evidence suggests that SUV max is useful in predicting prognosis. Studies are needed in this regard.
Conclusion
Molecular classification in breast cancer is very important in the treatment and prognosis follow-up of the disease. In our study, we demonstrated that different molecular subtypes show different metabolic characteristics. We also revealed that tumor Ki67 levels cause metabolic differences, and tumors with high Ki67 levels on 18F-FDG PET/CT have an increased likelihood of lymph node metastasis. We think that Ki67 levels should be taken into consideration when interpreting lymph node positivity in these patients.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Tokat Gaziosmanpasa University (Date: 2025-05-27, No:15235480-050.04-579263).
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The data supporting the findings of this article are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions. The corresponding author has committed to share the de-identified data with qualified researchers after confirmation of the necessary ethical or institutional approvals. Requests for data access should be directed to bmp.eqco@gmail.com
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
References
-
Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-49. doi:10.3322/caac.21660.
-
Orrantia-Borunda E, Anchondo-Nuñez P, Acuña-Aguilar LE, Gómez-Valles FO, Ramírez Valdespino CA, Maytovitz HN. Subtypes of breast cancer. In: Maytovitz HN, editor. Breast cancer. Brisbane: Exon Publications; 2022.p.31-42. doi:10.36255/exon-publications-breast-cancer-subtypes.
-
Goldhirsch A, Winer EP, Coates AS et al. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen iınternational expert consensus on the primary therapy of early breast cancer 2013. Ann Oncol. 2013;24(9):2206-23. doi:10.1093/annonc/mdt303.
-
Curigliano G, Burstein HJ, Winer EP, et al. De-escalating and escalating treatments for early-stage breast cancer: the St Gallen International Expert Consensus Conference on the primary therapy of early breast cancer 2017. Ann Oncol. 2017;28(8):1700-12. doi:10.1093/annonc/mdx308.
-
Kapoor V, McCook BM, Torok FS. An introduction to PET-CT imaging. Radiographics. 2002;24(2):523-43. doi:10.1148/rg.242025724.
-
Almuhaideb A, Papathanasiou N, Bomanji J. 18F-FDG PET/CT imaging in oncology. Ann Saudi Med. 2011;31(1):3-13. doi:10.4103/0256-4947.75771.
-
Hindié E. The EANM-SNMMI guideline on the role of [18F] FDG-PET/CT in breast cancer: Important milestones and perspectives for the future.Eur J Nucl Med Mol Imaging. 2024;51(9):2695-700. doi:10.1007/s00259-024-06758-y.
-
Han S, Choi JY. Impact of 18F-FDG PET, PET/CT, and PET/MRI on staging and management as an initial staging modality in breast cancer: a systematic review and meta-analysis. Clin Nucl Med. 2021;46(4):271-82. doi:10.1097/RLU.0000000000003502.
-
Akın M, Örgüç S, Aras F, Kandiloğlu AR. Molecular subtypes of invasive breast cancer: correlation between PET/computed tomography and MRI findings. Clin Nucl Med. 2020;41(8):810-6. doi:10.1097/MNM.0000000000001220.
-
Öner AO, Yıldırım Ş, Budak ES, Alikanoğlu AS. The relationship between 18F-FDG PET/CT parameters and histopathological-immunohistochemical properties in breast cancer. Health Sci Q. 2023;3(4):259-68. doi:10.26900/hsq.2122.
-
Koo HR, Park JS, Kang KW , et al.18 F-FDG uptake in breast cancer correlates with immunohistochemically defined subtypes. eEur Radiol. 2014;24(3):610-8. doi:10.1007/s00330-013-3037-1.
-
Kitajima K, Fukushima K, Miyoshi Y, et al. Association between 18F-FDG uptake and molecular subtype of breast cancer. Eur J Nucl Med Mol Imaging. 2015;42(9):1371-7. doi:10.1007/s00259-015-3070-1.
-
Aktaş A, Aslayan SO, Gürleyik MG, Güngör S. Correlations of primary tumor SUV max and axillary lymph node SUV max with molecular subtypes of invasive breast cancer. Indian J Surg. 2021;83:1-7. doi:10.1007/s12262-021-02770-w.
-
Topuz ÖV, Arslan E, Usul G. Relation Between Primary Tumor Suvmax Value, Ki-67 Proliferation Index and Axillary Metastasis in Patients with Triple-Negative Breast Cancer. Bagcilar Med Bull. 2025;10(1):51-7. doi:10.4274/BMB.galenos.2025.69885.
-
Shen G, Hu S, Kuang A. Relationship between FDG uptake on PET, tumor histology, and Ki-67 proliferation index in patients with breast cancer. J Nuclear Med. 2016;57(Suppl 2):1492.
-
Li Y, Zhang X, Qiu J, Pang T, Huang L, Zeng Q. Comparisons of p53, KI67, and BRCA1 expressions in patients with different molecular subtypes of breast cancer and their relationships with pathology and prognosis. J buon. 2019;24(6):2361-8.
-
Stathopoulos GP, Malamos NA, Markopoulos C, et al. The role of Ki-67 in the proliferation and prognosis of breast cancer molecular classification subtypes. Anticancer drugs. 2014;25(8):950-7. doi:10.1097/CAD.0000000000000123.
-
Tuzcu SA, Gezici A, Taşdemir B, Büyükbayram H, Çetin FA. The association of axillary lymph node-positive breast cancer with metabolic parameters of 18F-fluorodeoxyglucose PET/CT: axillary lymph node-positive breast cancer and PET/CT. MSD. 2020;7(3):445-9. doi:10.36472/msd.v7i3.363.
Tables
Table 1. Relationship between molecular subtypes and 18F-FDG PET/CT data
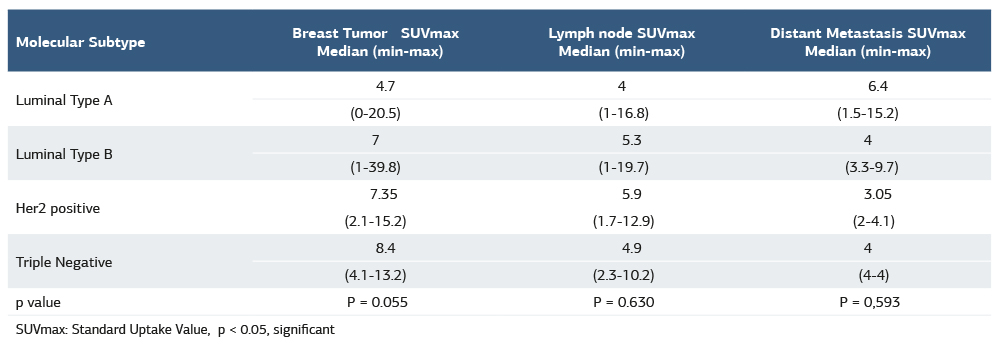
SUVmax: Standard Uptake Value, p < 0.05, significant
Table 2. Relationship between histologic subtypes and K67 proliferation
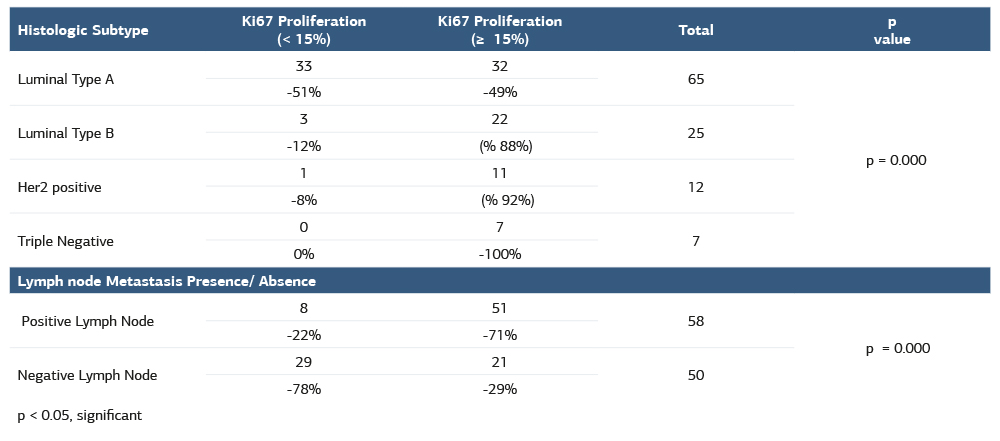
p < 0.05, significant
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ozge Ulaş, Zekiye Hasbek. Association of breast cancer with different molecular subtypes and ki-67 proliferation with 18f-fdg pet/ct. Ann Clin Anal Med 2026;17(2):139-143
- Received:
- May 21, 2025
- Accepted:
- July 21, 2025
- Published Online:
- August 27, 2025
- Printed:
- February 1, 2026