
Comparison of the analgesic efficacy of transversus abdominis plane block and quadratus lumborum block after a cesarean section under general anaesthesia: a randomised controlled trial
TAP vs QLB for post-cesarean analgesia
- Received:
- July 2, 2025
- Accepted:
- September 8, 2025
- Published Online:
- September 16, 2025
- Printed:
- October 1, 2025
Authors
Abstract
AimPostoperative pain following caesarean section is a significant clinical issue affecting maternal comfort, mobilisation, and recovery. This study aimed to compare the analgesic efficacy of ultrasound-guided Transversus Abdominis Plane (TAP) block and Quadratus Lumborum Block (QLB) in patients undergoing caesarean section under general anaesthesia.
MethodsFifty pregnant women scheduled for elective caesarean section between 2020 and 2021 were enrolled in this randomised controlled trial. Participants were randomly assigned into two groups: Group 1 received the TAP block (n = 25), and Group 2 received the QLB (n = 25). Postoperative pain was assessed using the Visual Analogue Scale (VAS) at the 1st, 3rd, 12th, and 24th hours. Additional parameters such as time to first analgesic requirement, total analgesic use within 24 hours, haemodynamic data, and complications were also recorded.
ResultsVAS scores were significantly lower in the QLB group at all measured time points (p < 0.05). Moreover, analgesia was required later, and total analgesic consumption was lower in the QLB group compared to the TAP group. Although nausea and vomiting were more frequent in the TAP group, the difference was not statistically significant. Haemodynamic parameters remained stable in both groups.
ConclusionBoth TAP and QLB blocks are safe and effective for postoperative pain control after caesarean delivery. However, QLB offers superior analgesic outcomes, including lower pain scores, delayed analgesic need, reduced analgesic consumption, and potentially greater patient comfort. QLB may therefore be a preferred technique in enhancing postoperative recovery in caesarean section patients.
Keywords
Introduction
Caesarean section is an invasive surgical procedure that is frequently preferred in high-risk situations for maternal and fetal health. This operation decreases patient comfort and may adversely affect the healing process due to incisional pain, which is frequently observed in the postoperative period. Uncontrolled postoperative pain may lead to cardiac complications as well as impaired respiratory function, inability to cough, atelectasis, and pulmonary complications 1. When appropriate analgesia is provided, the risk of these complications decreases and patient satisfaction and mobilisation process are positively affected. In recent years, regional block techniques have an important place in postoperative pain management. Transversus Abdominis Plane (TAP) block, one of these techniques, is widely used in abdominal surgeries and provides effective analgesia by blocking somatic nerves in the anterolateral abdominal wall 2. In this technique, local anaesthetic agents are injected into the fascial space between the internal oblique muscle and the transversus abdominis muscle, and nerve conduction is blocked 3. Direct visualisation of anatomical structures is possible with ultrasonography guidance, thus increasing both the accuracy and safety of block application 4. TAP block is widely preferred in the management of analgesia after caesarean section because it reduces the need for opioids and increases patient comfort 3,5,6. Alternatively, Quadratus Lumborum Block (QLB) is applied by injection into the interfascial space more posterior to the transversus abdominis muscle and is thought to provide a more comprehensive analgesia by targeting both somatic and visceral pain 7. In the literature, it has been reported that QLB not only provides longer-lasting analgesia, but also reduces opioid use and contributes to early postoperative mobilisation 8. Compared with TAP, QLB has been suggested to be superior, especially in terms of duration of analgesia and efficacy on visceral pain 9. However, a definite superiority between these two techniques in terms of analgesic efficacy, opioid requirement, and patient satisfaction has not been determined. Although there are studies in the literature comparing both blocks in different surgical fields, comparative studies in caesarean section are limited. In this context, this study aimed to compare the effects of TAP and QLB blocks on postoperative pain management, analgesic requirement, and patient comfort in women undergoing caesarean section.
Materials and Methods
Fifty patients who gave birth by caesarean section in a secondary care hospital between 2020-2021 were included in the study. Women who underwent caesarean section under general anaesthesia were included in the study. Women who underwent caesarean section under spinal anaesthesia, women with pain problems such as chronic fibromyalgia, women with unexplained and unexplained pain problems, or women receiving treatment were not included in the study.The pregnant women included in the study underwent caesarean section under general anaesthesia by the same physician, and the patients were divided into 2 groups by coin flip technique. Group 1 patients (n = 25) received Transversus Abdominis Plane (TAP) block, while Group 2 patients (n = 25) received Quadratus Lumborum Block (QLB). Pulse rate, blood pressure, pain intensity, the number of hours, and the number of times analgesia was needed postoperatively, and complications were recorded.
Statistical Analysis
Statistical analyses of the data obtained in this study were performed using SPSS (Statistical Package for Social Sciences) software. Firstly, the suitability of continuous variables for normal distribution was evaluated by using kurtosis and skewness values, and the range of -3 to +3 was accepted as the critical value. In the comparison of two independent groups in terms of continuous variables, Independent Groups T test was applied when the data were suitable for normal distribution, and Mann-Whitney U test was applied when the data did not show normal distribution. The Chi-Square test was used to compare categorical variables between groups and to evaluate their relationships. Repeated Measures ANOVA test was used for time-dependent repeated measurements (Mean Arterial Pressure, Pulse, and VAS (Visual Analog Scale) scores) during and after the operation, and time-dependent changes were evaluated separately within the groups.
Ethical Approval
This study was approved by the Ethics Committee of Esenyurt University (Date: 2025-05-14, No: 2025/04-52) and designed in accordance with the Declaration of Helsinki.
Results
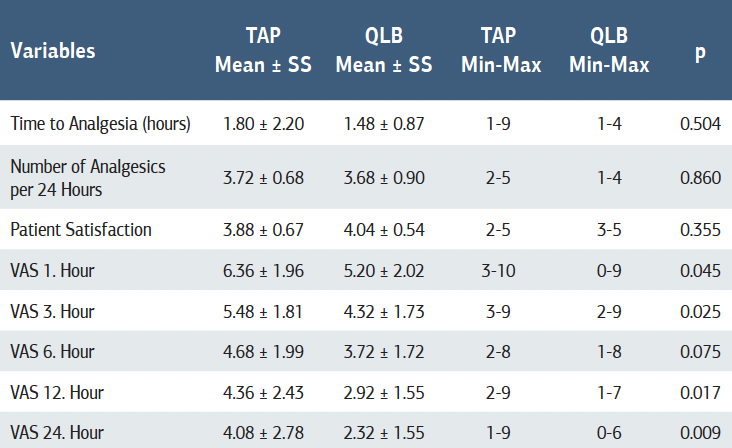
Demographic data of 50 patients included in the study are given in Table 1. Comparisons of complications and vital signs between the groups are given in Table 2. Information on the analgesia needs of the patients and the distribution of the pain felt by the patients according to the hours are shown in Table 3. When the complications were analysed, nausea was observed with a rate of 16% in the TAP block group and 8.0% in the QLB group, and no significant relationship was found between the groups. Similarly, while the frequency of vomiting was 4% in the TAP block group, no case of vomiting was detected in the QLB group, and no significant relationship was found between the groups. Urinary retention was not observed in any patient in both groups. While 96% of the patients in the TAP block group were in the ASA 2 anaesthesia group, all of the patients in the QLB group were in the ASA 2 anaesthesia group.
Discussion
This study aims to compare the effectiveness of Transversus Abdominis Plane (TAP) block and Quadratus Lumborum Block (QLB) on postoperative analgesia during caesarean section operations. The study findings show that both subjective pain scores (VAS) and analgesic requirements were significantly lower and patient satisfaction was higher in patients who underwent QLB. In addition, patient satisfaction scores were significantly higher in the QLB group, suggesting that this block method provides advantages not only in pain control but also in patient comfort and quality of the surgical experience. The Enhanced Recovery After Surgery (ERAS) protocol is currently used in most surgical fields to reduce morbidity, length of hospital stay, and promote postoperative recovery 10. However, postoperative pain is one of the undesirable outcomes that decreases postoperative quality of life for patients 11. Pain after abdominal surgery is largely related to somatic pain signals in the abdomen 12. To reduce this pain and increase patient comfort, local anaesthetics can be injected into the space between the internal oblique and transversus abdominis muscles to block the T6-L1 nerves, usually under ultrasonographic guidance 13. The literature has also shown that the dose of local anaesthesia in the TAP block is of great importance in the pain felt by the patient in the postoperative period. Some studies have argued that this block should be performed preoperatively to interrupt early pain impulses and reduce the need for opioids 14.
Alsharari et al. reported that TAP block was used as an effective strategy for pain management in laparoscopic colectomy patients, and the application of this procedure in addition to general anaesthesia reduced opioid consumption and accelerated the recovery time of patients 15. Some studies have found that there was no reduction in the need for opioids in the first 12 hours in patients who underwent TAP block 5. Erol et al. compared the VAS scores of the TAP blog combined with different types of anaesthesia and found that the 12th hour VAS scores were significantly higher in the groups in which only general anaesthesia, TAP with general anaesthesia, TAP with spinal anaesthesia and TAP with epidural anaesthesia were performed compared to the groups in which TAP was not performed 6. In a study conducted in Canada, it was found that the duration of analgesia requirement after TAP was prolonged up to 24 hours 16. These results have been shown to have favourable effects on patient satisfaction 2. Baaj et al. also found that there was better analgesia and patient satisfaction and less opioid requirement in the group in which TAP blog was applied compared to the group in which placebo was applied 17. In studies, it has been observed that QLB provides effective analgesia and decreases the mean VAS score 18. In addition, it has been reported that the side effects of QLB application are minimal and patients provide rapid mobilisation after general anaesthesia 19. In some studies comparing the analgesic superiority of both blogs, it has been claimed that the TAP blog has superior analgesic effects compared to QLB 20. There are studies showing that these blocks have similar effects. However, in this study, it was also reported that the TAP block was easier to administer and a lower level of expertise was required. It is also said to have less risk of nausea and vomiting 21. In our study, no significant difference was found in the incidence of nausea between the two block types. Although there is no consensus in the literature about the superiority of these two blocks, the QLB block comes to the fore. Roy et al. found a 25% decrease in fentanyl consumption with the QLB block compared to the TAP block up to 24 hours after the block, and also found that the duration of the need for additional analgesia was significantly longer 9. Dam et al. found that TAP block decreased opioid consumption during the operation in patients with percutaneous nephrolithotomy, but QLB was more effective in opioid consumption and analgesia 22. In a study comparing TAP block and QLB in patients undergoing total abdominal hysterectomy, it was observed that the duration of postoperative analgesia was higher in the QLB group than in the TAP group, and opioid requirement was significantly reduced in the QLB group 23. In their study, Blanco et al. observed that QLB block was better than TAP block for pain relief after caesarean section with longer- acting analgesia exceeding 24 hours and less additional opioid consumption 8. Verma et al. found that QLB block reduced the number of analgesic dose consumption and prolonged the duration of analgesia for 72 hours after caesarean section compared to patients receiving TAP block 20. Various studies have also shown that QLB block has less opioid requirement and analgesic effect persists for a longer period of time compared to TAP block despite the use of different analgesic agents 24. However, some recent studies have shown that QLB block failed to reduce morphine consumption in the first 12 hours 25. In parallel with this result, there are studies claiming that TAP block leads to better analgesia in the early short postoperative period, whereas QLB block provides more prolonged analgesia 9. In this study, VAS scores were found to be lower in all time periods in the QLB group. This difference was statistically significant, especially at the 1st, 3rd, 12th, and 24th hours (p < 0.05). This strongly supports that QLB is more effective in pain control than TAP block. In addition, it was observed that patients in the QLB group needed analgesia later, consumed less analgesics in 24 hours, and had higher satisfaction levels. These findings suggest that QLB block is superior to TAP block in terms of postoperative comfort and analgesia. However, it was also observed that the techniques had similar effects on haemodynamic stability. These findings are in agreement with the literature that QLB provides a more generalised analgesia that covers both visceral and somatic pain. While TAP block blocks only the somatic nerves of the anterolateral abdominal wall, QLB can provide deeper and longer-lasting analgesia by affecting both somatic and visceral afferent fibres thanks to the spread of local anaesthetics to the paravertebral area 8. This difference is manifested by lower VAS scores and less opioid requirement in the QLB group, especially in the first 24 hours. In addition, later analgesic requirement in the QLB group suggests that this method may increase early mobilisation and maternal comfort in the postoperative period. Similarly, Vaghela et al. reported that QLB provided more effective analgesia than TAP block in abdominal surgeries such as appendectomy and inguinal hernia repair, which supports the results of our study 7. Thus, QLB can be considered as an effective alternative to increase maternal safety and patient satisfaction, especially in obstetric surgeries.
Limitations
This study has some limitations. First of all, the study was conducted in a single centre with a limited number of patients (n = 50), and the generalisability of the results is limited. In addition, the use of coin toss technique as a randomisation method cannot completely eliminate the potential selection bias. Considering that the efficacy of the applied blocks may depend on the experience of the operator, the single practitioner may pose other limitations in terms of external validity. In addition, the subjective measure of VAS score was used for analgesia assessment, which may influence the results due to individual differences in patients’ pain threshold and perception. Finally, the follow-up period was limited to 24 hours, and late pain and complications were not evaluated. Therefore, studies with larger samples, multicentre and long-term follow- up are needed.
Conclusion
This study comparatively evaluated the efficacy of QLB and TAP blocks in postoperative pain management after caesarean section. Results showed that QLB provided a superior analgesic effect compared to TAP block with lower VAS scores, later analgesic requirement, less analgesic consumption, and higher patient satisfaction, especially in the first 24 hours. Both blocks were found to be safe and had similar effects on haemodynamic stability. These results increase the preferability of QLB in the management of analgesia after obstetric surgery and guide clinical practice to provide more effective patient comfort. However, the validity of the proposed approach will be further strengthened by supporting the findings with larger sample sizes and multicentre studies.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Esenyurt University (Date: 2025-05-14, No: 2025/04-52)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
References
-
De Oliveira GS Jr, Castro-Alves LJ, Nader A, Kendall MC, McCarthy RJ. Inadequate postoperative pain management is associated with persistent pain, delayed functional recovery, and longer hospital stay, which increase medical expenses, and is becoming a public health issue. BMC Anesthesiol. 2019;19(1):86.
-
Mishriky BM, George RB, Habib AS. Transversus abdominis plane block for analgesia after Cesarean delivery: a systematic review and meta-analysis. Can J Anaesth. 2012;59(8):766-78.
-
Zhang D, Zhou C, Wei D, Ge L, Li Q. Dexamethasone added to local anesthetics in ultrasound-guided transversus abdominis plain (tap) block for analgesia after abdominal surgery: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2019;14(1):e0209646.
-
Warman P, Nicholls B. Ultrasound-guided nerve blocks: efficacy and safety. Best Pract Res in Clin Anaesthesiol. 2009;23(3):313-26.
-
Yan ZR, Chen LJ, Zhang SJ, et al. The transversus abdominis plane block in conjunction with intrathecal morphine use after cesarean section in women with severe pre-eclampsia: a randomized controlled trial. BMC Anesthesiol. 2023;23(1):100.
-
Erol MK, Şengel A, Tammo Ö, Seçilmiş S, Kaya F. The effect of TAP block use in postoperative analgesic in cesarean section. Eur Rev Med Pharmacol Sci. 2023;27(7):2786-93.
-
Vaghela S, Chaurasiya M, Prakash R, Khan M. Ultrasound-guided quadratus lumborum block versus transversus abdominis plane block for laparoscopic inguinal hernia repair and appendicectomy using ropivacaine with dexmedetomidine. Cureus. 2023;15(1):e33450.
-
Blanco R, Ansari T, Riad W, Shetty N. Quadratus lumborum block versus transversus abdominis plane block for postoperative pain after cesarean delivery: a randomized controlled trial. Reg Anaesth Pain Med. 2016;41(6):757-62.
-
Roy A, Bhoi D, Chhabra A, Mohan VK, Darlong V, Prasad G. Quadratus lumborum block vs. transversus abdominis plane block in laparoscopic trans-abdominal pre- peritoneal repair of inguinal hernia in adults: a randomised controlled trial. Indian J Anaesth. 2023;67(2):207-15.
-
Helander EM, Billeaud CB, Kline RJ, et al. Multimodal approaches to analgesia in enhanced recovery after surgery pathways. Int Anesthesiol Clin. 2017;55(4):51–69.
-
Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;10:2287-98.
-
Kamel BH, Ibrahim SF, Abo Seif EMK, Hassan HS. Comparison of ultrasound guided transversus abdominis plane block versus intravenous patient controlled analgesia for post operative analgesia in patients undergoing lower abdominal surgeries under spinal anesthesia. QJM. 2024;117(Suppl 2):hcae175.025.
-
Li C, Shi J, Jia H. Ultrasound guided transversus abdominis plane block as an effective anesthetic technique for transverse colostomy in a high risk elderly patient: a case report. Front Med (Lausanne). 2023;10:1102540.
-
De Oliveira GS Jr, Castro-Alves LJ, Nader A, Kendall MC, McCarthy RJ. Transversus abdominis plane block to ameliorate postoperative pain outcomes after laparoscopic surgery: a meta-analysis of randomized controlled trials. Anesth Analg. 2014;118(2):454-63.
-
Alsharari AF, Abuadas FH, Alnassrallah YS, Salihu D. Transversus abdominis plane block as a strategy for effective pain management in patients with pain during laparoscopic cholecystectomy: a systematic review. J Clin Med. 2022;11(23):6896.
-
Abdallah FW, Halpern SH, Margarido CB. Transversus abdominis plane block for postoperative analgesia after Cesarean delivery performed under spinal anesthesia? A systematic review and meta-analysis. Br J Anaesth. 2012;109(5):679-87.
-
Baaj JM, Alsatlı RA, Majaj HA, Babay ZA, Thallaj AK. Efficacy of ultrasound guided transversus abdominis plane (TAP) block for post-cesarean section delivery analgesia – a double-blind, placebo-controlled, randomized study. Middle East J Anaesthesiol. 2010;20(6):821-6.
-
Zhao Z, Xu K, Zhang Y, Chen G, Zhou Y. Quadratus lumborum block for postoperative analgesia after cesarean section: a meta-analysis of randomized controlled trials with trial sequential analysis. Sci Rep.2021;11(1):18104.
-
Haskins SC, Tseng A, Zhong H, et al. Anterior quadratus lumborum block does not provide superior pain control after hip arthroscopy: a double-blinded randomized controlled trial. Anesthesiology. 2021;135(3):433-41.
-
Verma K, Malawat A, Jethava D, Jethava DD. Comparison of transversus abdominis plane block and quadratus lumborum block for post-caesarean section analgesia: a randomised clinical trial. Indian J Anaesth. 2019;63(10):820-6.
-
El Boghdadly K, Desai N, Halpern S, et al. Quadratus lumborum block vs. transversus abdominis plane block for caesarean delivery: a systematic review and network meta analysis. Anaesthesia. 2021;76(3):393-403.
Tables
Table 1. Demographic data
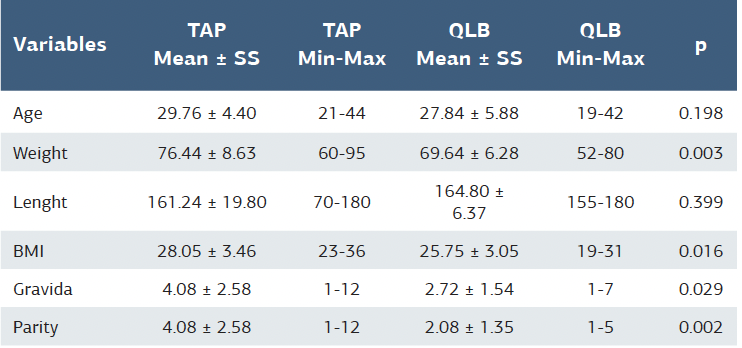
Table 2. Mean arterial pressure and pulse rate
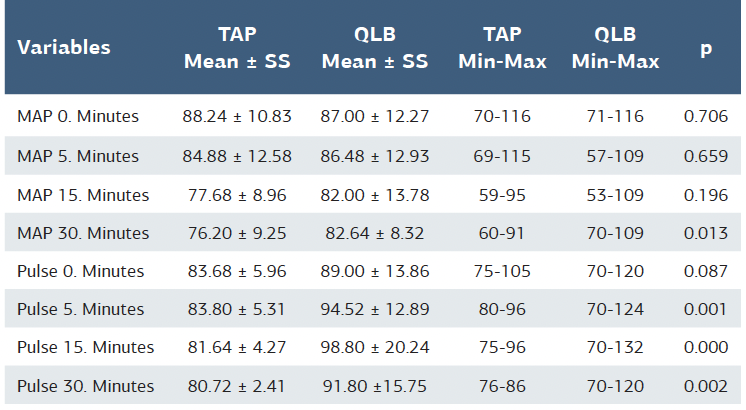
Table 3. Time to analgesia, analgesic use in 24 hours, patient satisfaction, and VAS score
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Melih Bestel, Elif Ucar, Abdulhakim Şengel, Nesrin Burcu Kaya, Güven Arslan, Erkan Şimşek. Comparison of the analgesic efficacy of transversus abdominis plane block and quadratus lumborum block after caesarean section under general anaesthesia: A randomised controlled trial. Ann Clin Anal Med 2025;16(10):725- 729