
Prospective screening for carbapenemase-producing gram-negative bacteria in rectal swabs of ICU patients
Detection of CPE in ICU patients
Authors
Abstract
Aim In recent years, carbapenem-resistant enteric gram-negative bacilli in intensive care units and their emergence as an important pathogen causing morbidity and mortality have been remarkably increasing. Considering that colonisation occurs primarily in Intensive Care Unit patients, we decided to perform a prospective surveillance study to investigate carbapenemase-producing Enterobacteriaceae in rectal swab samples.
Methods The patients were enrolled on admission to Intensive Care Units from the 1st of February to the 15th of May 2014. The rectal swabs were taken within the first 48 hours and then weekly during hospitalization. Rectal swab samples were plated on chromID CARBA (bioMérieux) chromogenic agar plates. The next day detected colonies were named according to their colors. At the same time, VITEK2 automated system identification was performed, and MIC values for carbapenems were determined by the E-test method. During the study period, 204 samples from 104 patients were evaluated.
Results Only 2 of the patients (1.9%) had initial rectal swab samples positive for carbapenemase-producing Enterobacteriaceae. Overall, during the hospitalization period, 6 patients (5.8%) were screened as carbapenem-resistant Enterobacteriaceae. One of the isolates (16.7%) was identified as E.coli, the others were Klebsiella pneumoniae (83.3%). Urine cultures of 2 patients were also detected as carbapenemase-producing Enterobacteriaceae. As a result, 2% of patients followed up in our Intensive Care Units had carbapenemase-producing Enterobacteriaceae in rectal swab cultures on admission.
Conclusion Screening Intensive Care Units with rectal swabs for colonization will provide us with early infection control and appropriate empiric therapies.
Keywords
Introduction
In recent years, the emergence of carbapenem-resistant enteric gram-negative bacilli as significant pathogens in intensive care units and the associated increase in morbidity and mortality have been striking. With new medical and surgical procedures, hospital infections are occurring more frequently and are increasingly important due to their rising costs and associated mortality, and the legal liabilities they entail are now part of our ongoing concerns.1,2 The primary role in the growing mortality associated with hospital infections is played by the increasing incidence of multidrug-resistant (MDR) microorganisms as causative agents. Over the past 20 years, while there has been a noteworthy increase in both gram-positive and gram-negative MDR bacteria, very few new antimicrobial drugs have been introduced.3 Carbapenems have become the last line of defense in treating infections caused by such bacteria. However, in recent years, carbapenem- resistant enteric gram-negative bacilli have become prominent among healthcare-associated pathogens worldwide.4,5 Carbapenemase-producing strains are not only capable of hydrolyzing carbapenems but are also resistant to a range of other antibiotics. Effectively treating infections caused by these pathogens presents a significant challenge for clinicians.5 Most infections originating in the intensive care unit (ICU) are preceded by colonization of the patient by the responsible microorganisms. Screening stool samples or rectal/perirectal swabs provides more meaningful results than screening other body sites.6 Presuming that colonization occurs first in patients, this prospective surveillance study was conducted to investigate the presence and, if present, the incidence of carbapenemase-producing Enterobacteriaceae in rectal swab samples from patients followed up in our ICUs.
Materials and Methods
This study was planned as a prospective, targeted, active surveillance study. Patients aged ≥ 18 years who were admitted to the Intensive Care Units (Central, Emergency, and Palliative Intensive Care Units) of Istanbul Dr. Lütfi Kırdar Kartal Training and Research Hospital between February 1 and May 15, 2014, were included in this study. Within the first 48 h of admission, rectal swab samples were collected from the patients, and case report forms were filled out to record patient information (age, sex, admission diagnosis, length of stay in the intensive care unit, comorbid diseases, and history of antibiotic use in the past month). Weekly rectal swab samples were collected from patients throughout their ICU stay. Rectal swab samples were examined for carbapenem-resistant gram-negative bacilli. The results of the rectal swab cultures, infections that developed during their stay in the ICU, infectious agents and their antibiotic susceptibilities, antibiotics used, and invasive procedures performed were all recorded. The relationship between colonization and the development of infection was investigated. Rectal swab samples were transported to the central microbiology laboratory using Stuart transport medium and immediately inoculated onto chromID CARBA (bioMérieux) agar plates, which are chromogenic media. After incubation at 35 ± 2°C for 18-24 hours, the plates were individually assessed for growth. Colonies growing on the plates were identified by color according to the manufacturer’s instructions. The same colonies were identified using the VITEK 2 automated system with GN-ID and GN09 (bioMérieux) cards. After identification and antibiogram, the MIC (Minimum Inhibitory Concentration) values for imipenem, ertapenem, and meropenem were recorded. The MIC values were interpreted according to CLSI (Clinical Laboratory Standards Institute) 2012 criteria. All KPC- producing strains isolated from rectal swabs were subjected to the Modified Hodge test. A suspension was prepared from the E. coli ATCC 25922 strain according to 0.5 McFarland standards. An antibiogram was prepared using Mueller-Hinton agar (MHA) medium. After the medium was allowed to dry for 10-15 minutes, a 10 µg ertapenem disk was placed at the center of the plate. The strains to be tested were streaked from the periphery towards the center along the four sides of the plate with a loop. After incubation at 35 ± 2°C for 18-24 hours, any distortion or cloverleaf-shaped zone of inhibition around the disk was considered positive.
Ethical ApprovalThis study was approved by the Ethics Committee of Dr. Lütfi Kırdar Kartal Training and Research Hospital (Date: 2014-02- 11, No: 22).
Statistical AnalysisData obtained from the study were recorded into the SPSS for Windows 15.0 program and statistically analyzed. In the study, descriptive statistics including frequency, ratio, median, mean, and standard deviation were used.
Reporting GuidelinesThe study was reported in accordance with STROBE.
Results
During the study period, 104 patients were included, and 204 swab samples were assessed. Of these patients, 41 (39.4%) were monitored in the emergency intensive care unit, 37 (35.6%) in the central intensive care unit, and 26 (25%) in the palliative care unit. 51 patients (49%) were admitted to the ICU from home, 36 (34.6%) from surgical clinics, 12 (11.5%) from internal medicine clinics, and 5 (4.8%) from other hospitals. Of the patients included in the study, 68 (65.4%) were male and 36 (34.6%) were female, with a mean age of 61.1 ± 18 (median age 65). Among the patients, 41 had cardiovascular disease, 35 had malignancy, 21 had diabetes mellitus, 17 had chronic obstructive pulmonary disease, 11 had cerebrovascular events, 7 had chronic renal failure, and 2 had collagen tissue disease; one patient each had splenectomy, trauma, and burn as comorbidities. Eight patients had a history of surgical intervention within the last month, and 32 (30.8%) had a history of antibiotic use within the last month. The admission diagnoses to the ICU were: respiratory failure in 29 patients (27.9%), pneumonia in 18 (17.3%), intracranial hemorrhage in 15 (14.4%), postoperative follow-up in 12 (11.5%), acute abdomen in 10 (9.7%), trauma in 7 (6.7%), cerebrovascular event in 4 (3.8%), gastrointestinal bleeding in 2 (1.9%), and hypoxic encephalopathy, drug intoxication, diabetic ketoacidosis, Guillain-Barre syndrome, urinary tract infection, and burn in one patient each. During their ICU stay, 47 patients (45.2%) had a central venous catheter placed: 22 (46.8%) subclavian, 17 (16.3%) jugular, and 8 (7.7%) femoral catheters. During the ICU follow-up, 52 patients (50%) died. Twenty-five (24%) patients were still being monitored in the ICU at the end of the study period. Twenty-five (24%) were transferred to the relevant clinics. Two (1.9%) patients were discharged in good health. Only two patients (1.9%) showed CPE growth in the first rectal swab sample. In the weekly samples, CPE was detected in six patients (5.8%). The mean age of the six patients in whom CPE was isolated in rectal swab samples during screening was 63.6 ± 25.6 (median age 58). Two (33.3%) were women, and four (66.7%) were men. Three patients (50%) were monitored in the central intensive care unit, two (33.3%) in the palliative care unit, and one (16.7%) in the emergency intensive care unit. Two were admitted with respiratory failure, and one each with acute abdomen, intracranial hemorrhage, pneumonia, and hypoxic encephalopathy. Four of the six patients with CPE colonization had a catheter. All four catheters were jugular type. Among the six patients who tested positive in the screening, one (16.6%) died. The mean length of stay for these patients was 37 days. Of the two patients who had CPE colonization upon ICU admission, one had a history of antibiotic use within the previous 30 days. In patients without CPE colonization, 30% had a history of antibiotic use. All four patients who developed CPE colonization during their ICU stay had used at least one antibiotic prior to colonization while in the ICU. Of these four cases, three used carbapenems, three cephalosporins, three glycopeptides, two beta-lactam/beta-lactamase inhibitors, and two colistin. In contrast, the antibiotic usage rate among patients who did not develop CPE colonization was 69%. In one patient with CPE colonization, the rectal swab turned negative during follow-up. The CPE microorganisms isolated from the patients’ rectal swabs and their MIC values are listed in Table 1. Of the CPE isolates, 5 (83.3%) were Klebsiella pneumoniae and one (16.7%) was E. coli. During follow-up of the six patients with CPE colonization, two developed carbapenem- resistant Klebsiella pneumoniae ssp. in their urine cultures, and one developed carbapenem-resistant Acinetobacter baumannii in their catheter tip culture. During the study period in intensive care units, at least one microbiologically proven infection developed in 18 (17.3%) of the 104 patients followed: six patients had Acinetobacter baumannii-related primary bloodstream infection, four patients had ventilator-associated pneumonia due to A. baumannii, one patient had secondary bloodstream infection due to A. baumannii, one patient had urinary tract infection due to A. baumannii, one patient had wound and soft tissue infection due to A. baumannii, two patients had urinary tract infection due to K. pneumoniae, one patient had ventilator-associated pneumonia due to E. coli, one patient had wound and soft tissue infection due to P.eruginosa, and one patient had primary bloodstream infection due to Candida parapsilosis.
Discussion
In 2% of our patients admitted to the ICU, Enterobacteriaceae producing KPC were detected in rectal swab samples at the beginning. A study showed that 12.8% of ICU patients had enteric colonization with KPC-producing K.pneumoniae upon admission.7 Our rate is lower than other studies and centers’ data, indicating the KPC problem, but during ICU monitoring, gastrointestinal colonization with carbapenemase-producing Enterobacteriaceae occurred in 6% of the patients in rectal swab cultures. KPC-producing Enterobacteriaceae have caused a series of infection outbreaks in the northeastern USA, Israel, and Greece, where they are highly endemic.5,8 Most reports on these outbreaks are molecular-level in vitro reports, not focusing on issues in treating infections and the negative impact on patient prognosis.6,9 Small clinical studies have shown high failure rates in the treatment of these infections, with mortality rates ranging from 22% to 72%.10 In our study, the mortality rate for bacteria producing KPC was reported as 16%. The spread of KPC-producing K.pneumoniae is a growing problem, limiting treatment options for the infections it causes and frequently leading to clinical failure in ICUs. Studies have shown a significant relationship between the number and specific class of antibiotics previously used by patients and infection and/or colonization with carbapenemase-producing Enterobacteriaceae. Most studies have found that prior exposure to carbapenems is an independent risk factor. Apart from carbapenems, aminopenicillins and other anti-pseudomonal penicillins (with or without ß-lactamase inhibitors) have also been identified as independent risk factors.11,12 One study indicated that antibiotics posing a risk for colonization with KPC-producing K.pneumoniae are carbapenems and ß-lactam/ ß-lactamase inhibitors.7 The same study showed that, besides antibiotic use history, previous ICU admission history, previous hospital stay duration, and the presence of COPD were risk factors for colonization with KPC-producing K.pneumoniae (7). ChromID CARBA agar medium is an easily applicable and highly accurate screening method for detecting Enterobacteriaceae producing KPC in rectal swabs. This method detected KPC- producing colonized patients much faster than manually prepared screening media (within 24 hours). Considering that the time to detect such pathogens is crucial for infection control policies, this method is very important for the immediate reporting of isolates with carbapenemase activity and taking appropriate infection control measures, as well as for identifying colonized patients at risk of invasive infections.13 In our study, patients colonized with Enterobacteriaceae producing KPC, detected using chromID CARBA agar medium, were reported to the infection control committee to ensure that appropriate measures were taken.Studies on the use of the modified Hodge test have shown conflicting results. While some indicate its inadequacy in detecting metallo-beta-lactamases, others argue that the modified Hodge test yields false-positive results.14 One study in India suggested avoiding the modified Hodge test for non-fermentative gram-negative bacteria and recommended the use of the EDTA-meropenem or EDTA- ceftazidime combination tests.15 Another study clearly showed that carbapenemase activity was present at high rates in members of the Enterobacteriaceae family detected with the modified Hodge test, which is shown to be easy to apply and inexpensive. All clinical isolates should be routinely tested for possible carbapenemase activity. In terms of public health, confirming the resistance mechanism is not necessary. The evaluation of risk factors for infection with carbapenemase- producing bacteria should be encouraged. Infection control programs combined with effective antibiotic policies and good medical practices can help manage the threat of antibiotic resistance.16 In our study, the modified Hodge test results for KPC-producing isolates detected using chromogenic agar medium were also positive. The CDC’s guidelines for preventing carbapenem-resistant Enterobacteriaceae discuss the necessary precautions to be taken. The importance of hand hygiene and access to necessary protective equipment is particularly emphasized. Contact precautions should be applied to patients infected or colonized with carbapenem-resistant Enterobacteriaceae. Information on patients with a history of colonization should be recorded. Although it is not clearly stated for how long strict contact precautions should be applied, the CDC recommends at least 6 months. Healthcare workers caring for patients infected or colonized with MDR microorganisms, including carbapenem-resistant Enterobacteriaceae, must be trained on measures to prevent the spread of these microorganisms. Invasive procedures applied to patients (central catheters, endotracheal tubes, and urinary catheters) pose a significant risk for developing device-associated infections, especially in colonized patients.17 In our study, four of the six patients with positive results had central venous catheters.
Limitations
The study was conducted as a single-center study over a short period (February 1 to May 15, 2014), which limits its ability to detect longer-term trends in colonization or infection rates. Molecular typing of carbapenemase genes (e.g., KPC, NDM, OXA-48) was not performed, which would have provided more precise information regarding the resistance mechanisms and their potential for transmission. Additionally, the study did not evaluate patient-level outcomes in detail, such as infection-related mortality, length of ICU stay related specifically to colonization or infection, or potential clonal spread between patients. Finally, due to limited resources, only the Modified Hodge test was used for phenotypic confirmation, despite the existence of more sensitive and specific molecular or biochemical assays.
Conclusion
The detection of Enterobacteriaceae producing KPC in rectal swab samples at the beginning in 2% of the ICU patients we monitored indicates a significant problem we will face shortly. However, this study was conducted over a short period. Surveillance data over a longer period on more patients are needed. Investigating rectal colonization in high-risk units, such as ICUs, and incorporating it into routine surveillance services will ensure early infection control and proper guidance for empirical treatments.
Declarations
Ethics Declarations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and its later amendments. All procedures involving human participants were approved by the relevant institutional ethics committee. Patient confidentiality and data protection principles were strictly maintained throughout the study.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all participants prior to inclusion in the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: G.A.Ö., S.G.
Methodology: G.A.Ö.
Formal Analysis: G.A.Ö.
Investigation: G.A.Ö., S.G., D.H., B.Ç.
Data Curation: G.A.Ö.
Writing – Original Draft Preparation: G.A.Ö.
Writing – Review & Editing: S.G., D.H., B.Ç.
Supervision: B.Ç.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
CLSI: Clinical Laboratory Standards Institute
CPE: Carbapenemase-Producing Enterobacteriaceae
ICU: Intensive Care Unit
KPC: Klebsiella pneumoniae Carbapenemase
MDR: Multidrug-Resistant
MIC: Minimum Inhibitory Concentration
MHA: Mueller-Hinton Agar
SPSS: Statistical Package for the Social Sciences
References
-
Flodgren G, Conterno LO, Mayhew A, Omar O, Pereira CR, Shepperd S. Interventions to improve professional adherence to guidelines for prevention of device-related infections. Cochrane Database Syst Rev. 2013;3;CD006559. doi:10.1002/14651858.CD006559.pub2
-
Marschall J, Mermel LA, Fakih M, et al. Strategies to Prevent Central Line– Associated Bloodstream Infections in Acute Care Hospitals: 2014 Update. Infect Control Hosp Epidemiol. 2014;35(7):753–771. doi:10.1086/676533
-
Ramana KV, Mohanty SK, Kumar A. In vitro activities of current antimicrobial agents against isolates of pyoderma. Indian J Dermatol Venereol Leprol. 2008;74(4):430. doi:10.4103/0378-6323.42886
-
Schwaber MJ, Carmeli Y. Carbapenem-resistant Enterobacteriaceae: a potential threat. JAMA. 2008;300(24):2911-2913. doi:10.1001/jama.2008.896
-
Nordmann P, Naas T, Poirel L. Global spread of carbapenemase-producing Enterobacteriaceae. Emerg Infect Dis. 2011;17(10):1791-1798.
-
Lledo W, Hernandez M, Lopez E, et al. Guidance for control of infections with carbapenem-resistant or carbapenemase-producing Enterobacteriaceae in acute care facilities. MMWR Morb Mortal Wkly Rep. 2009;58(10):256-260.
-
Papadimitriou-Olivgeris M, Marangos M, Fligou F, et al. Risk factors for KPC- producing Klebsiella pneumoniae enteric colonization upon ICU admission. J Antimicrob Chemother. 2012;67(12):2976-29781.
-
Cuzon G, Naas T, Truong H, et al. Worldwide diversity of Klebsiella pneumoniae that produce β-lactamase blaKPC-2 gene. Emerg Infect Dis. 2010;16(9):1349-1356.
-
Marchaim D, Navon-Venezia S, Schwaber MJ, Carmeli Y. Isolation of imipenem- resistant Enterobacter species: emergence of KPC-2 carbapenemase, molecular characterization, epidemiology, and outcomes. Antimicrob Agents Chemother. 2008;52(4):1413-1418.
-
Hirsch EB, Tam VH. Detection and treatment options for Klebsiella pneumoniae carbapenemases (KPCs): an emerging cause of multidrug-resistant infection. J Antimicrob Chemother. 2010;65(6):1119-1125.
-
Hyle EP, Ferraro MJ, Silver M, Lee H, Hooper DC. Ertapenem-resistant Enterobacteriaceae: risk factors for acquisition and outcomes. Infect Control Hosp Epidemiol. 2010;31(12):1242-1249.
-
Gasink LB, Edelstein PH, Lautenbach E, Synnestvedt M, Fishman NO. Risk factors and clinical impact of Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. Infect Control Hosp Epidemiol. 2009;30(12):1180-1185. doi:10.1086/648451
-
Vrioni G, Daniil I, Voulgari E, et al. Comparative evaluation of a prototype chromogenic medium (ChromID CARBA) for detecting carbapenemase- producing Enterobacteriaceae in surveillance rectal swabs. J Clin Microbiol. 2012;50(6):1841-1846.
-
Carvalhaes CG, Picão RC, Nicoletti AG, Xavier DE, Gales AC. Cloverleaf test (modified Hodge test) for detecting carbapenemase production in Klebsiella pneumoniae: be aware of false positive results. J Antimicrob Chemother. 2010;65(2):249-251.
-
Noyal MJ, Menezes GA, Harish BN, Sujatha S, Parija SC. Simple screening tests for detection of carbapenemases in clinical isolates of nonfermentative Gram-negative bacteria. Indian J Med Res. 2009;129(6):707-712.
-
Ramana KV, Rao R, Sharada ChV, Kareem M, Reddy LR, Ratna Mani M. Modified Hodge test: a useful and low-cost phenotypic method for detection of carbapenemase producers in Enterobacteriaceae members. J Nat Sci Biol Med. 2013;4(2):346-348.
-
Chitnis AS, Edwards JR, Ricks PM, Sievert DM, Fridkin SK, Gould CV. Device- associated infection rates, device utilization, and antimicrobial resistance in long-term acute care hospitals reporting to the National Healthcare Safety Network, 2010. Infect Control Hosp Epidemiol. 2012;33(10):993-1000.
Tables
Table 1. Carbapenemase-producing enterobacterales (CPE) isolated from patients’ rectal swabs and their MIC values
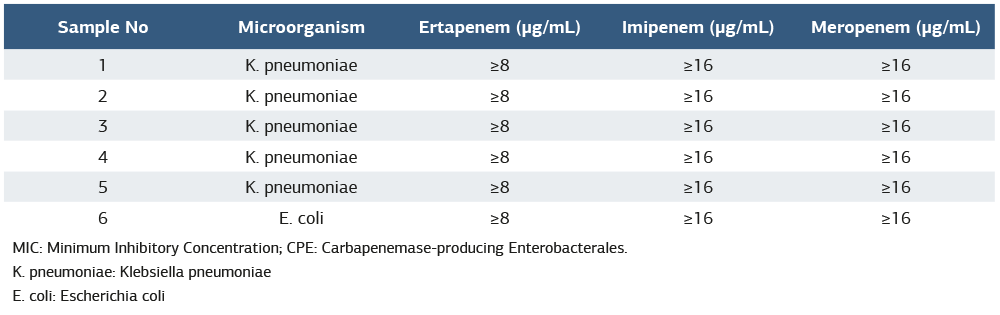
MIC: Minimum Inhibitory Concentration; CPE: Carbapenemase-producing Enterobacterales. K. pneumoniae: Klebsiella pneumoniae E. coli: Escherichia coli
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Conference Presentation
This study was presented as an oral presentation at the 15th UTSAK Congress, Ankara, Türkiye, 2024
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Gülfem Akengin Öcal, Serap Gencer, Demet Hacıseyitoğlu, Banu Çevik. Prospective screening for carbapenemase-producing gram-negative bacteria in rectal swabs of ICU patients. Ann Clin Anal Med 2026;17(Suppl 2):S152-156. doi: 10.4328/ACAM.22809
- Received:
- July 13, 2025
- Accepted:
- August 19, 2025
- Published Online:
- August 30, 2025
- Printed:
- March 20, 2026