
The relationship between 18F-FDG PET/CT semi-quantitative values and systemic inflammation markers in lung cancer
18F-FDG PET/CT in lung cancer
Authors
Abstract
Aim This study investigated the relationship between systemic inflammation markers in peripheral blood, 18F-FDG PET/CT staging, PET/CT visual data, and semi-quantitative values in lung cancer.
Methods The study included 76 newly diagnosed lung cancer patients who underwent 18F-FDG PET/CT for staging between 2023 and 2024.
Results A significant positive correlation was found between the maximum standardized uptake value (SUVmax) of the lung mass and the systemic immune-inflammation index (SII). However, no significant correlation was observed between the SUVmax of the lung mass and the platelet-to-lymphocyte ratio (PLR) or neutrophil-to-lymphocyte ratio (NLR). A significant positive correlation was also found between the total lesion glycolysis and metabolic tumor volume of the lung mass and the SII, NLR, and PLR.
Conclusion Our findings suggest that metabolic parameters on initial PET/CT are positively correlated with systemic inflammation markers. We propose that both factors contribute to a poorer prognosis in lung cancer and should be considered during patient follow-up. Additionally, we would like to emphasize that the possibility of an underlying malignancy should not be overlooked in patients with elevated inflammation levels, especially those admitted to the hospital for other clinical reasons.
Keywords
Introduction
It is estimated that one in three people worldwide will develop cancer, and one in four will die from it.1 Lung cancer is the cause of cancer-related deaths on a global scale, with approximately 2.48 million new cases and 1.8 million deaths, respectively.2 It is also the second most common type of cancer in both women and men.2 Approximately 80% of lung cancer cases are attributed to smoking.3 In general, lung cancers are classified into small-cell lung cancer and non-small-cell lung cancer.4
Inflammation has been recognized as an unfavourable prognostic factor in lung cancer.5 Numerous studies have demonstrated its role in promoting angiogenesis, immune evasion, and the development of distant metastases.6 As a result, several indices have been developed to reflect peripheral inflammation. These include the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and the systemic immune-inflammation index (SII), which is calculated by multiplying the NLR by the platelet count. Furthermore, studies have reported that elevated levels of these inflammatory markers are associated with more advanced tumour stages.7
18F- fluorodeoxyglucose positron emission tomography/ computer tomography (18F-FDG PET/CT), which provides both functional and anatomical imaging, is a non-invasive whole-body imaging modality used in the diagnosis, staging, and assessment of treatment response in lung cancer.8 Semi-quantitative parameters derived from PET/CT, such as maximum standardized uptake value (SUVmax), total lesion glycolysis (TLG), and metabolic tumour volume (MTV), reflect tumour metabolism and biological aggressiveness.9 Additionally, a recent systematic review indicated that PET/CT metabolic parameters have prognostic value in various cancers, including lung cancer.10
The aim of this study was to investigate the relationship between systemic inflammation markers in peripheral blood and 18F-FDG PET/CT findings, including staging, visual assessment, and semi-quantitative parameters, in patients with lung cancer.
Materials and Methods
The study included 76 newly diagnosed lung cancer patients who underwent 18F-FDG PET/CT for staging between 2023 and 2024. Patients with a history of prior cancer treatment were excluded from the study. Additionally, those who had received surgery, chemotherapy, or radiotherapy were not included.
18F-FDG PET/CT PET/CT images were evaluated in the Department of Nuclear Medicine both visually and quantitatively. Quantitative parameters included maximum standardized uptake value (SUVmax), mean standardized uptake value (SUVmean), total lesion glycolysis (TLG), and metabolic tumour volume (MTV). The presence or absence of metastases and their anatomical locations, as detected on PET/CT, were also recorded.
18F-FDG PET/CT Imaging ProtocolPatients were instructed to fast for at least 4-6 hours, and their blood glucose levels were measured before the imaging procedure. Only patients with fasting blood glucose levels below 200 mg/dL were injected with the radiopharmaceutical. During the 18F-FDG PET/CT examinations, an average dose of 10 mCi of 18F-FDG was administered. After the injection, all patients were asked to rest in the relaxation room for 45-60 minutes. Imaging was performed using the General Electric Discovery PET/CT 600 device. CT imaging was conducted with a 16-slice spiral scanner at 120 kV and 172 mAs for attenuation correction and anatomical correlation. Three-dimensional PET imaging was performed, covering the body from the skull to the proximal thigh. PET imaging was conducted for approximately 2 minutes at each bed position. Axial, coronal, and sagittal fusion images were generated using the iterative reconstruction method. The maximum standardized uptake values (SUVmax) were calculated based on the PET images. An adaptive threshold setting of 42% of the maximum regional metabolic activity was applied to the PET images, and the region of interest (ROI) was placed within the primary tumor, avoiding the peripheral area.
The following formula was used to calculate the SUVmax: [Activity in ROI (mCi/mL) × Body Weight (grams)] ÷ Injected Dose (mCi)
Ethical ApprovalThis study was approved by the Ethics Committee of Tokat Gaziosmanpasa University, Faculty of Medicine (Date: 2025-02-25, No: E-15235480-050.04-534232).
Statistical AnalysisThe data obtained from our study were analyzed using the SPSS 23.0 software. The normality of the data was assessed both visually (histogram and probability plots) and analytically (Kolmogorov-Smirnov/Shapiro-Wilk tests). Since the data did not meet the assumptions of normality, the Mann-Whitney U test was used to compare two independent groups. For categorical data, differences in frequencies between groups were evaluated using the Chi-square test. For the analysis of numerical variables, correlation coefficients and statistical significance were calculated using the Spearman test when at least one of the variables did not follow a normal distribution. The significance level was set at 0.05.
Reporting GuidelinesThis retrospective observational study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
Results
The mean age of the 76 patients, 12 of whom were female (15.8%) and 64 of whom were male (84.2%), was 65 years. Of these, 35 patients (46.1%) were younger than 65 years, while 41 patients (53.9%) were 65 years or older. A total of 55 patients (72%) were smokers, and 21 patients (28%) were non-smokers. Data from 3 patients (4%) were unavailable. At the time of diagnosis, 25 patients (32.9%) had metastasis, while 51 patients (67.1%) did not. No significant correlation was found between the presence of metastasis and smoking status, lung tumour SUVmax, TLG, or MTV values (p = 0.917, p = 0.232, p = 0.899, p = 0.511). Furthermore, no significant correlation was observed between metastasis and SII, PLR, or NLR (p = 0.532, p = 0.899, p = 0.486). Regarding pathological subtypes, 34 patients (44.7%) had squamous cell carcinoma, 29 patients (38.2%) had adenocarcinoma, and 13 patients (17.1%) had small cell carcinoma. No significant correlation was found between metastasis and pathological subtypes (p = 0.234).
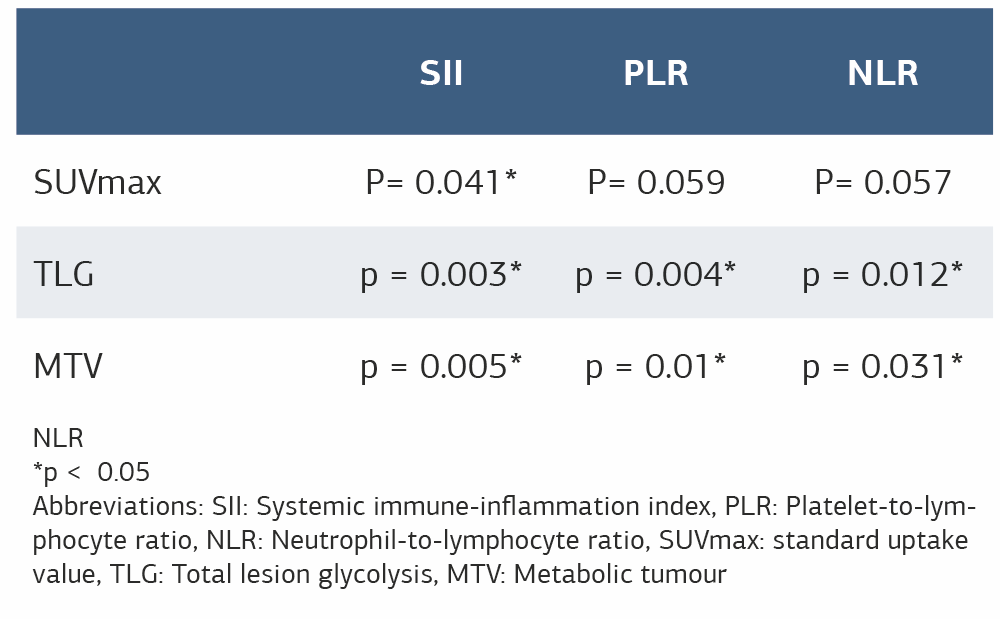
A significant positive correlation was found between the SUVmax value of the lung mass and SII (p = 0.041, r = 0.235), (Table 1). However, no significant correlation was observed between the SUVmax of the lung mass and PLR or NLR (p = 0.059, p = 0.057). There was also no significant correlation between the SUVmax value of the lung mass and smoking status (p = 0.775).
A significant positive correlation was observed between the TLG value of the lung mass and SII, NLR, and PLR (p = 0.003, p = 0.004, p = 0.012). Similarly, a significant positive correlation was found between the MTV value of the lung mass and SII, NLR, and PLR (p = 0.005, p = 0.01, p = 0.031). All 18F-FDG PET/CT parameters of the lung mass were most strongly associated with SII, with NLR being the second most strongly associated. Among metabolic parameters, inflammation markers were most strongly associated with TLG.
No significant correlation was found between systemic inflammatory markers and metabolic markers in early-stage cancers and diffuse-stage cancers. Additionally, no significant correlation was observed between smoking and SII, PLR, or NLR. Similarly, no significant correlation was found between age group and SII, PLR, or NLR.
Discussion
Recently, numerous studies have reported a relationship between tumour development and inflammation, highlighting the role of inflammation in both the initiation and progression of tumours. Neutrophils, lymphocytes, and platelets—key components of the inflammatory response—have been implicated in tumour cell proliferation, angiogenesis, and metastasis.11,12 Consequently, inflammation has been identified as a negative prognostic factor in many types of cancer. Moreover, semi-quantitative PET/CT parameters such as SUVmax, TLG, and MTV have also been shown to have prognostic value.13,14
A total of seven studies involving 2,070 patients have demonstrated that high systemic immune-inflammation index (SII) values, calculated at the time of diagnosis and before treatment, are associated with poor prognosis in patients with lung cancer.15 Several of these studies also reported that SII is superior to NLR and PLR in predicting prognosis. In our study, all metabolic markers of the lung tumour were most strongly associated with SII. As metabolic parameters increased, SII levels also rose. Elevated levels of these markers are indicative of poor prognosis. Following SII, the neutrophil-to-lymphocyte ratio (NLR) showed the second strongest correlation with metabolic activity.
In a meta-analysis of 17 studies involving 8,877 patients, high systemic immune-inflammation index (SII) values were associated with worse overall survival (OS) and progression-free survival (PFS) compared to low SII values.16 These studies did not find a significant relationship between pathological subtype and SII. Similarly, in our study, no significant association was observed between pathological subtype and SII.
Semi-quantitative PET/CT parameters, including SUVmax, TLG, and MTV, are prognostic indicators in cancer patients.15,16,17 Mirilli et al. reported that the neutrophil-to-lymphocyte ratio (NLR) was a prognostic factor and showed a significant positive correlation with both TLG and MTV.17 Consistently, our study also demonstrated a significant correlation between NLR and TLG and MTV values.
In a study of 132 patients, Göksel et al. found a significant association between MTV and TLG and systemic inflammation markers, while no such relationship was observed with SUVmax.18 Öner et al. reported that NLR could predict advanced-stage renal cell carcinoma, and Göksel et al. found that NLR and PLR levels were significantly higher in late-stage compared to early-stage lung cancer patients.18,19 However, in our study, we did not observe a significant association between disease stage (local vs. advanced) and either systemic inflammatory markers or PET/CT metabolic parameters.
Hu et al. reported that TLG and MTV were associated with both early and advanced stages in lung cancer patients in a study of 119 patients and that disease progression was accompanied by an increase in metabolic parameters.20 In line with our findings, a significant positive correlation was observed between TLG, MTV, and the systemic immune-inflammation index (SII), NLR, and PLR. Additionally, similar to our study, no significant correlation was found between smoking and either inflammatory or metabolic markers.
In contrast, a study by Çekici et al. found a significant positive correlation between smoking and NLR.21 The limitations of our study include its retrospective design, the differing sex ratio, the exclusion of patients with concomitant inflammatory lung diseases, and the relatively small sample size. Additionally, as we were unable to present the survival data of the patients, a prognosis analysis could not be performed.
Limitations
One of the limitations of our study was the relatively small sample size and its retrospective design. Additionally, it was not known whether the patients had concomitant benign inflammatory lung diseases.
Conclusion
According to the results of our study, metabolic parameters at baseline PET/CT were positively correlated with systemic inflammation markers. We suggest that both parameters contribute to a poorer prognosis in lung cancer and should be considered when monitoring such patients. Although we could not assess the prognosis due to the retrospective nature of our study, we plan to expand our research in the future to include a prognostic analysis. Additionally, we would like to emphasize that the possibility of an underlying malignancy should not be overlooked in patients with elevated inflammation levels, especially those admitted to the hospital for other clinical reasons.
While there has been considerable interest in inflammation markers in cancer patients recently, few publications have explored the relationship between inflammation markers and metabolic parameters in lung cancer, and studies on the systemic immune-inflammation index (SII) in lung cancer remain limited.
Declarations
Ethics Declarations
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Tokat Gaziosmanpasa University, Faculty of Medicine (Date: 2025-02-25, No: E-15235480-050.04-534232). Due to the retrospective design and anonymized data collection, informed consent was waived by the Ethics Committee.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Due to the retrospective design of the study and the use of anonymized patient data, the requirement for informed consent was waived by the Ethics Committee.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request. Due to institutional and ethical restrictions, the data are not publicly available.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None
Author Contributions (CRediT Taxonomy)
Conceptualization: O.U., Z.H.
Methodology: O.U.
Formal Analysis: O.U.
Investigation: O.U., Z.H.
Data Curation: O.U.
Writing – Original Draft Preparation: O.U.
Writing – Review & Editing: Z.H.
Supervision: Z.H.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
FDG: Fluorodeoxyglucose
MTV: Metabolic Tumor Volume
NLR: Neutrophil-to-Lymphocyte Ratio
PET/CT: Positron Emission Tomography/Computed Tomography
PLR: Platelet-to-Lymphocyte Ratio
ROI: Region of Interest
SII: Systemic Immune-Inflammation Index
SUVmax: Maximum Standardized Uptake Value
SUVmean: Mean Standardized Uptake Value
TLG: Total Lesion Glycolysis
References
-
Roxburgh CS, McMillan DC. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010;6(1):149-163.
-
Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clinic. 2021;71(3):209-249.
-
Holford TR, Levy DT, McKay LA, et al. Patterns of birth cohort–specific smoking histories, 1965–2009. Am J Prev Med. 2014;46(2):e31-7.
-
Bade BC, Cruz CSD. Lung cancer 2020: epidemiology, etiology, and prevention. Clin Chest Med. 2020;41(1):1-24.
-
RebuzziSE, PrelajA, FriedlaenderA, et al. Prognostic scores including peripheral blood-derived inflammatory indices in patients with advanced non-small-cell lung cancer treated with immune checkpoint inhibitors. Crit Rev Oncol Hematol. 2022;179:103806.
-
Tan, Z, XueH, Sun Y, et. al. The role of tumor inflammatory microenvironment in lung cancer. Front Pharmacol. 2021;2:688625.
-
Goksel S, Cengiz A, Ozturk H, et al. Prognostic impact of the 18F-fluorodeoxyglucose positron-emission tomography/computed tomography metabolic parameters and correlation with hematological inflammatory markers in lung cancer. J Cancer Res Ther. 2021;17(4):925-930.
-
Martucci F, Pascale M, Valli MC. Impact of 18F-FDG PET/CT in staging patients with small cell lung cancer: a systematic review and meta-analysis. Front Med. 2020;6:336.
-
WangY, Han R, Wang Q, et al. Biological significance of 18F-FDG PET/CT maximum standard uptake value for predicting EGFR mutation status in non- small cell lung cancer patients. Int J Gen Med. 2021;14:347-356.
-
Dolan RD, McLees NG, Irfan A, et al. The relationship between tumor glucose metabolism and host systemic inflammatory responses in patients with cancer: a systematic review. J Nuc Med. 2019;60(4):467-471.
-
Liao CP, Booker RC, Brosseau JP, et al. Contributions of inflammation and tumor microenvironment to neurofibroma tumorigenesis. J Clin Invest. 2018;128(7):2848-2861.
-
Caziuc A, Schlanger D, Amarinei G, et al. Neutrophils-to-lymphocytes, lymphocytes to-monocytes and platelets-to-lymphocytes ratios-predictive biomarkers for response to neoadjuvant chemotherapy in breast cancer. J BUON. 2020;25(1):182-187.
-
Cremonesi M, Gilardi L, Ferrari ME, et al. Role of interim 18 F-FDG-PET/ CT for the early prediction of clinical outcomes of non-small cell lung cancer (NSCLC) during radiotherapy or chemo-radiotherapy. A systematic review. EJNM. 2017;44:1915-1927.
-
Vokes EE, Govindan R, Iscoe N, et al. The impact of staging by positron- emission tomography on overall survival and progression-free survival in patients with locally advanced NSCLC. J Thorac Oncol. 2018;13(8):1183-1188.
-
Wang Y, Li Y, Chen P. Prognostic value of the pretreatment systemic immune- inflammation index (SII) in patients with non-small cell lung cancer: a meta- analysis. Ann Transl Med. 2019;7(18):433.
-
Huang W, Luo J, Wen J. The relationship between systemic immune- inflammatory index and prognosis of patients with non-small cell lung cancer: a meta-analysis and systematic review. Front Surg. 2022;9:898304.
-
Mirili C, Guney IB, Paydas S. Prognostic significance of neutrophil/lymphocyte ratio (NLR) and correlation with PET–CT metabolic parameters in small cell lung cancer (SCLC). Int J Clin Oncol. 2019;24:168-178.
-
Park SY, Lee JH, Kim HJ, et al. Relationship between systemic inflammatory markers and metabolic parameters on 18F-FDG PET/CT in patients with non-small cell lung cancer. Diagnostics (Basel). 2023;13(6):1013. doi:10.3390/diagnostics13061013
-
Oner I, Sackan F, Ozdemir D. Evaluation of the Preoperative Haematological Parameters Predicting the High T-Stage and Fuhrman Grade in Renal Cell Carcinoma. Age. 2022;60(15.4):60-67.
-
Hu Y, Sun J, Li D, et al. The combined role of PET/CT metabolic parameters and inflammatory markers in detecting extensive disease in small cell lung cancer. Front Oncol. 2022;12:960536.
-
Cekici Y, Yılmaz M, Seçen Ö. New inflammatory indicators: association of high eosinophil-to-lymphocyte ratio and low lymphocyte-to-monocyte ratio with smoking. J Int Med Res. 2019;47(9):4292-4303.
Tables
Table 1
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ozge Ulas, Zekiye Hasbek. The relationship between 18F-FDG PET/CT semi-quantitative values and systemic inflammation markers in lung cancer. Ann Clin Anal Med 2026;17(3):210-213
- Received:
- August 4, 2025
- Accepted:
- October 6, 2025
- Published Online:
- October 22, 2025
- Printed:
- March 1, 2026