
Complex regional pain syndrome in a patient with an idiopathic lumbosacral radiculoplexus lesion: A Case Report
Idiopathic lumbosacral radiculoplexus lesion
Authors
Abstract
Introduction Complex regional pain syndrome (CRPS) of the lower extremity can occasionally occur without an obvious precipitating cause.
Case presentation A 59-year-old female developed swelling, pain, and motor weakness in the left ankle without any trauma or systemic illness. Initial workup for musculoskeletal and infectious causes was unremarkable. The patient’s symptoms fulfilled the Budapest criteria for CRPS, and she was treated conservatively with no improvement. Neurological examination revealed proximal weakness, prompting EMG, which showed neurogenic involvement from L4–S1. Subsequent contrast-enhanced lumbosacral MRI (neurography) demonstrated thickening and enhancement of the left L5 nerve root, consistent with plexitis. An idiopathic lumbosacral radiculoplexus lesion was diagnosed. The patient’s symptoms gradually improved with gabapentin and a tramadol-paracetamol regimen.
Conclusion This case highlights a rare coexistence of CRPS with idiopathic lumbosacral radiculoplexopathy. In CRPS patients refractory to standard treatments, clinicians should consider proximal nerve lesions. EMG can localize such lesions, and targeted MRI can confirm inflammatory radiculoplexus neuropathy.
Keywords
Introduction
Complex regional pain syndrome (CRPS) is a chronic pain condition usually precipitated by trauma or surgery, but in some patients, no clear etiology is identified. In cases of lower extremity CRPS without a specific cause, a detailed neurological workup can be crucial. Electromyography (EMG) may contribute to the diagnosis, especially if motor deficits are present on examination.1 Identifying an underlying neuropathic process is important because it can change the management and prognosis. We present a patient who was initially managed as idiopathic CRPS of the leg but was subsequently found to have an underlying idiopathic lumbosacral radiculoplexus neuropathy (also known as idiopathic lumbosacral plexopathy), a very rare disorder.
Case Presentation
A 59-year-old female presented with swelling and pain in her left foot and ankle that had begun insidiously three months prior. There was no history of trauma, surgery, or systemic illness. She reported progressive difficulty walking due to pain and weakness.
Initial investigations for her persistent ankle pain were largely unremarkable. An ankle MRI revealed only soft tissue edema in the first and second tarsometatarsal regions, without fractures or significant arthropathy. Lumbar MRI showed mild degenerative disc disease at the L3–L4 and L5–S1 levels, but no nerve root compression. A bone scintigraphy demonstrated increased perfusion, hyperemia, and osteoblastic activity in the left foot’s tarsal region, which was interpreted as possibly consistent with osteomyelitis; however, no clinical or laboratory evidence of infection was present (inflammatory markers were within normal limits). Routine laboratory tests, including markers for rheumatologic or metabolic disease, were all within normal limits.
The patient was initially treated with a plaster splint immobilization of the ankle for three weeks and given analgesic medications. Despite conservative therapy, her symptoms did not improve. On follow-up physical examination, there was noticeable glossy (shiny) discoloration of the left foot skin with mild edema. The left ankle joint had a terminal limitation in range of motion. Manual muscle testing revealed weakness in left ankle dorsiflexion and great toe extension. Sensory examination showed allodynia and hyperalgesia in the left foot. These findings met the Budapest clinical criteria for CRPS (including continuing pain disproportionate to any inciting event, plus signs of sensory changes, vasomotor and sudomotor changes, edema, and motor/trophic changes).
Given the presence of motor deficits (weak dorsiflexion) not typical in uncomplicated CRPS, an electrodiagnostic evaluation was performed to search for an underlying neuropathic process. EMG study of the left lower limb showed evidence of neurogenic denervation changes in muscles corresponding to the L4–S1 myotomes. The pattern of findings indicated involvement both proximal and distal to the dorsal root ganglion at those levels, which suggested a polyradiculopathy or plexus lesion rather than an isolated radiculopathy. Based on the EMG results, a lumbosacral plexopathy was suspected.
To further evaluate the suspected plexus lesion, a contrast-enhanced lumbosacral MRI (MR neurography) was obtained. On a 3D STIR (Short Tau Inversion Recovery) sequence focused on the lumbosacral plexus, there was mild fusiform thickening and contrast enhancement observed along approximately a 3 cm segment of the left L5 nerve, distal to the neural foramen (Figure 1). These MRI findings were consistent with an inflammatory plexus lesion (plexitis) affecting the lumbosacral plexus, specifically the L5 component. Post-contrast T1-weighted MRI showed enhancement of the left L5 nerve/root (Figure 2). No compressive mass or structural lesion was seen. Based on the combination of EMG and MRI findings, the patient was diagnosed with idiopathic lumbosacral radiculoplexus neuropathy coexisting with CRPS of the left lower extremity.
In light of the new diagnosis, gabapentin (600 mg orally twice daily) was initiated for neuropathic pain, along with an analgesic combination of tramadol (50 mg) and paracetamol (500 mg) given twice daily. Physical therapy was also started. Over the subsequent weeks, she reported gradual improvement in her pain and an increase in ankle strength. At the three-month follow-up, her CRPS symptoms were significantly reduced, and she was ambulating with minimal discomfort.
Ethical ApprovalWritten informed consent was obtained from the patient for publication. Formal ethics committee approval was not required.
Reporting GuidelinesThis case is reported in accordance with the CARE guidelines.
Discussion
CRPS and lumbosacral plexopathy are both primarily clinical diagnoses, established by history and physical examination. CRPS typically features severe limb pain with sensory, autonomic, and motor changes after limb injury, whereas lumbosacral plexopathy often presents with acute or subacute onset of back and/or leg pain followed by motor weakness and sensory loss in the affected nerve distribution.2 In our patient, the clinical picture initially fulfilled the criteria for CRPS (allodynia, hyperalgesia, skin shininess, edema, and motor weakness in the affected limb). However, the presence of a notable motor deficit (foot drop) prompted further investigation for a neurological lesion.
Lumbosacral radiculoplexus neuropathy (also called lumbosacral plexopathy or, in diabetic patients, diabetic amyotrophy) is far less common than its upper extremity counterpart, brachial plexopathy, and can pose a diagnostic challenge. Coexistence of lumbosacral plexus injury with common degenerative changes (such as lumbar discopathy) may further complicate the differential diagnosis. Idiopathic lumbosacral plexopathy is extremely rare, with an incidence estimated below 1/100,000 in the general population.3 By definition, idiopathic cases are diagnosed only after known etiologic factors such as diabetes, trauma, neoplasm, infection, or prior radiation are excluded.4,5 In our patient, extensive evaluation revealed no such underlying causes, qualifying the plexus lesion as idiopathic. Notably, the painful onset and subacute proximal weakness in idiopathic lumbosacral radiculoplexus neuropathy can resemble diabetic amyotrophy; both are thought to share an immune-mediated microvasculitic pathogenesis.6
Electrophysiological studies are crucial for localizing and characterizing neuropathic lesions in cases like this. In our case, EMG helped differentiate a plexus-level injury from a simple radiculopathy or peripheral neuropathy by showing a pattern of denervation extending across multiple root levels both proximally and distally. EMG is especially valuable in identifying occult radiculoplexus neuropathies and guiding further imaging.1 Once a radiculoplexus lesion was suspected, advanced neuroimaging confirmed the diagnosis. MRI of the plexus, particularly with contrast and STIR sequences, can visualize nerve inflammation or enlargement. In this patient, the increased signal intensity on STIR and contrast enhancement along the L5 nerve course was interpreted as evidence of active plexitis, consistent with reports in the literature on imaging of plexopathies.7
This case underlines that CRPS, usually a diagnosis of exclusion, may sometimes coincide with an unrecognized proximal nerve lesion. While CRPS itself can cause motor impairment due to disuse or pain, pronounced weakness should prompt consideration of a neurological injury. Only a few cases in the literature have discussed such a coexistence of CRPS with lumbosacral plexopathy, making this report an important addition. Early recognition of the underlying radiculoplexus neuropathy in a patient with apparent CRPS is critical, as it directs treatment toward neuropathic pain management and potentially immunotherapies in severe cases, rather than solely focusing on symptomatic relief of CRPS.
Limitations
This report describes a single patient, which limits generalizability and precludes causal inferences. The CRPS diagnosis relied on the Budapest clinical criteria without objective autonomic testing.
Conclusion
Although very rare, an idiopathic lumbosacral radiculoplexus neuropathy can present alongside (or masquerade as) complex regional pain syndrome. In a patient diagnosed with CRPS who does not respond to standard therapies, clinicians should maintain a high index of suspicion for an occult proximal nerve lesion. Careful neurological examination and EMG can reveal signs of radiculoplexus involvement, and contrast-enhanced MRI can then be utilized to confirm plexus inflammation. This case highlights a rare overlap of two conditions and emphasizes the importance of considering a broad differential diagnosis in refractory CRPS, as identifying an underlying neuropathy can significantly alter the management and improve patient outcomes.
Ethical Approval and Informed Consent: Written informed consent was obtained from the patient for publication of this case report, and formal ethics committee approval was not required in accordance with institutional and national guidelines.
Declarations
Ethics Declarations
This case report was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the patient.
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None
Author Contributions (CRediT Taxonomy)
Conceptualization: A.H.G.
Investigation: A.H.G., M.Z.
Resources: A.H.G.
Data curation: A.H.G., D.E.G.D.
Visualization: D.E.G.D.
Writing – original draft: A.H.G.
Writing – review & editing: A.H.G., D.E.G.D., M.Z.
Supervision: A.H.G.
Scientific Responsibility Statement
The authors declare full responsibility for the scientific content and integrity of this manuscript.
Abbreviations
CRPS: Complex Regional Pain Syndrome
EMG: Electromyography
MRI: Magnetic Resonance Imaging
STIR: Short Tau Inversion Recovery
References
-
Kimura J. Electrodiagnosis in Diseases of Nerve and Muscle: Principles and Practice. 4th ed. Oxford University Press; 2013:383-387.
-
Ehler E, Vyšata O, Včelák R, Pazdera L. Painful lumbosacral plexopathy: a case report. Medicine (Baltimore). 2015;94(17):e766. doi:10.1097/MD.0000000000000766
-
Tarulli A, Rutkove SB. Lumbosacral plexitis. J Clin Neuromuscul Dis. 2005;7(2):72-78. doi:10.1097/01.cnd.0000191290.19671.6b
-
Ng PS, Dyck PJ, Laughlin RS, Thapa P, Pinto MV, Dyck PJB. Lumbosacral radiculoplexus neuropathy: incidence and association with diabetes mellitus. Neurology. 2019;92(11):e1188-e1194. doi:10.1212/WNL.0000000000007020
-
Dyck PJ, Norell JE. Non-diabetic lumbosacral radiculoplexus neuropathy: natural history and comparison with diabetic variety. Brain. 2001;124(pt 6):1197-1207. doi:10.1093/brain/124.6.1197
-
Dyck PJ, Windebank AJ. Diabetic and nondiabetic lumbosacral radiculoplexus neuropathies: insights into pathophysiology. Muscle Nerve. 2002;25(4):477-491. doi:10.1002/mus.10080
-
Maravilla K, Bowen C. Imaging of the peripheral nervous system: evaluation of plexopathy. AJNR Am J Neuroradiol. 1998;19(6):1011-1023.
Figures
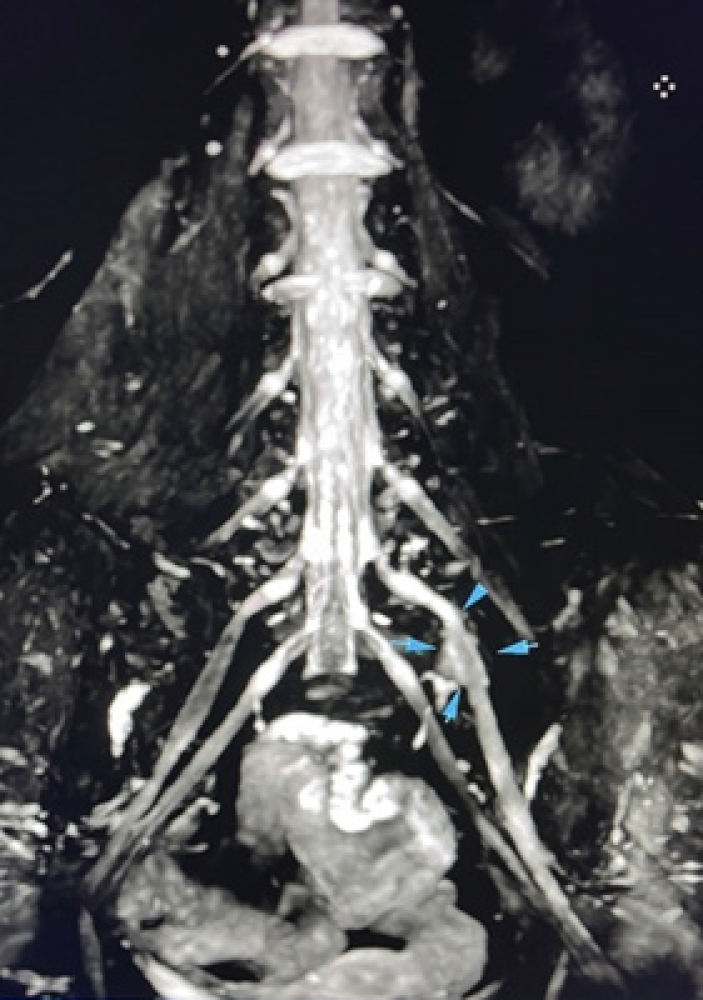
Figure 1. 3D MR neurography image illustrating mild thickening and enhancement of the left L5 nerve (arrow) distal to the neural foramen, consistent with an idiopathic plexitis
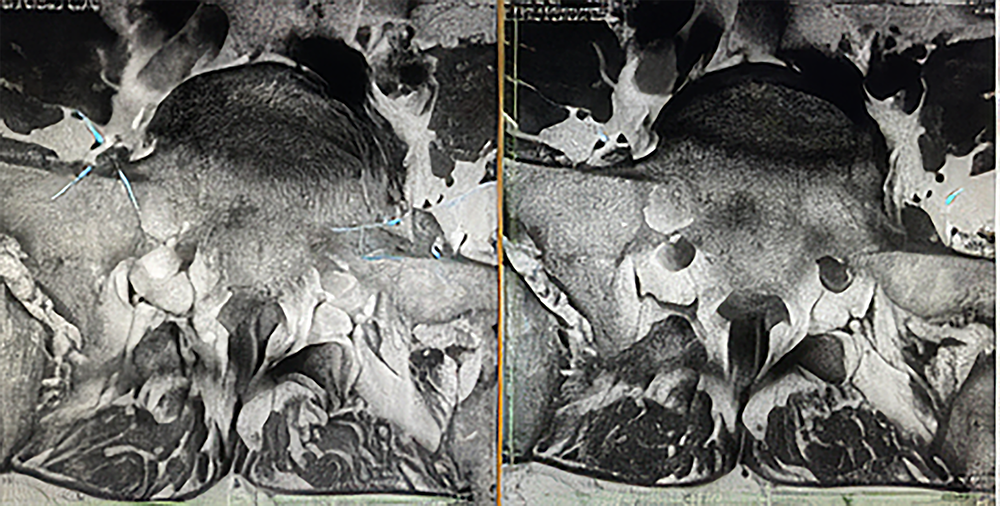
Figure 2. T1-weighted MRI of the lumbosacral region with (left) and without (right) contrast. The post-contrast image shows clear enhancement of the left L5 nerve root (arrow), confirming the presence of active inflammation (plexus neuritis) that is not visible on the non-contrast image
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ahmet Hilmi Günüç, Dilan Ece Geylan Durgun, Murat Zinnuroğlu. Complex regional pain syndrome in a patient with an idiopathic lumbosacral radiculoplexus lesion: A Case Report. Ann Clin Anal Med 2026;17(3):265-268
- Received:
- October 6, 2025
- Accepted:
- November 10, 2025
- Published Online:
- December 7, 2025
- Printed:
- March 1, 2026