
Refining the phenotype of Kaposi sarcoma: a comparative analysis of lymphatic and endothelial marker expression during histological progression
Lymphatic marker expression in Kaposi sarcoma
Authors
Abstract
Aim Kaposi sarcoma (KS) is a vascular neoplasm associated with human herpesvirus 8 (HHV-8). While conventional endothelial markers, such as CD31 and CD34, are well-established, the expression patterns of lymphatic markers (D2-40, Prox1) and the transcription factor FLI-1 across histological stages remain underexplored.
Methods Archival tissue from 80 HIV-negative KS patients was retrospectively analyzed. Lesions were staged as patch (n = 10), plaque (n = 25), or nodular (n = 45). Immunohistochemical staining for CD31, CD34, D2-40, FLI-1, Prox1, and HHV-8 was performed, with semi-quantitative assessment of staining extent (focal/diffuse) and intensity (weak/strong). Chi-square tests compared patterns across stages and markers (p<0.05).
Results All markers showed high sensitivity (95-100%). Staining extent and intensity were independent of stage for most markers (p>0.05), except D2-40 intensity, which increased significantly with progression (p=0.008). Nodular stage revealed significant discordances, where Prox1 extent was more frequently focal compared to the diffuse staining of HHV-8, CD31, D2-40, and FLI-1 (p<0.05).
Conclusion D2-40, Prox1, and FLI-1 are reliable diagnostic adjuncts, with D2-40 intensity correlating with advanced stages, suggesting a role in progression. These findings refine KS phenotyping and highlight potential pathogenic insights.
Keywords
Introduction
Kaposi sarcoma (KS) is a low-grade vascular tumor etiologically linked to infection with Kaposi sarcoma herpesvirus (KSHV), also known as human herpesvirus 8 (HHV-8).1 This angioproliferative tumor is characterized by KSHV-positive spindle cells of endothelial origin.2 KS is categorized into four main clinical-epidemiological forms: classic (sporadic), endemic (African), iatrogenic (transplant-related), and AIDS-associated (epidemic).3 Regardless of the clinical subtype, KS typically progresses through three histological stages: patch, plaque, and nodular.3
The pathological diagnosis of KS relies heavily on immunohistochemistry (IHC) to confirm endothelial nature and viral presence.4 Spindle cells consistently express pan- endothelial markers CD31 and CD34.4,5,6,7 HHV-8 detection via the Latency-Associated Nuclear Antigen-1 (LANA-1) is the gold standard, demonstrating high sensitivity/specificity as evidenced by stippled nuclear staining.3 Emerging evidence supports a lymphatic phenotype in KS.,5 with expression of lymphatic markers such as podoplanin (D2-40) and Prox1, a master regulator of lymphatic differentiation.5 HHV-8 induces Prox1, reprogramming cells toward lymphatic lineage.5 FLI-1, a nuclear transcription factor in vascular development, is consistently expressed in KS, aiding differential diagnosis of vascular tumors.7,8
While individual markers’ utility is established, comparative patterns across KS stages, especially in HIV-negative cohorts, are undercharacterized.9 The complex interplay between viral infection and endothelial reprogramming can result in heterogeneous marker expression, complicating the precise understanding of KS pathogenesis. Therefore, this study aims to systematically compare the expression of the lymphatic and vascular markers Prox1, D2-40, and FLI-1 against conventional markers (CD31, CD34) and HHV-8 across the patch, plaque, and nodular stages of KS.7 This comprehensive analysis seeks to refine their diagnostic utility and further elucidate their potential roles in the progression of this unique neoplasm.
Materials and Methods
Study Design and Patient CohortThis retrospective study analyzed archival tissue from the Department of Pathology at Ondokuz Mayıs University. Formalin-fixed, paraffin-embedded (FFPE) blocks from 80 cutaneous KS patients (January 2006-June 2018) were included.
Histopathological EvaluationAll original hematoxylin and eosin (H&E) stained slides were independently re-evaluated by two experienced pathologists to confirm the diagnosis and classify each case into one of three histological stages-patch, plaque, or nodular-based on established morphological criteria. Blocks with sufficient tissue and optimal histomorphology were selected for subsequent analysis.
Immunohistochemistry and ScoringFive-micron (5 µm) thick sections were cut from the selected FFPE blocks. Immunohistochemical staining was performed using a fully automated stainer (Ventana BenchMark ULTRA™, Ventana Medical Systems, Tucson, AZ). The panel of primary antibodies included: CD31 (Clone: JC70A, Cell Marque™), CD34 (Clone: QBEnd/10, Ventana™), D2-40 (Podoplanin, Cell Marque™), FLI-1 (Clone: G146-222, BioSB™), HHV-8 (LANA-1, Clone: 13B10, Cell Marque™) and Prox1 (Clone: EPR17448, Abcam™).
Appropriate positive control tissues were used for each antibody: tonsil for CD31, CD34 and D2-40; hemangioma for FLI-1; known KS tissue for HHV-8; and fetal heart muscle for Prox1. A non-immune serum was substituted for the primary antibody as a negative control.
All stained slides were assessed in a blinded fashion by two pathologists. The evaluation was performed semi-quantitatively based on staining extent and intensity. Staining extent in spindle cells was categorized as: negative (no staining), focal (<10% of cells stained), or diffuse (>10% of cells stained). Staining intensity was graded as weak or strong. For FLI-1, HHV-8, and Prox1, only nuclear staining was considered positive, with punctate staining graded as weak and homogenous staining as strong. For CD31, CD34, and D2-40, cytoplasmic and/or membranous staining was evaluated, with intensity based on the chromogen density.
Ethical ApprovalThis study was approved by the Ethics Committee of Ondokuz Mayıs University Clinical Research Ethics Committee (Date: 14.07.2017, Decision No: KAEK2017/271).
Statistical AnalysisStatistical analysis was performed using SPSS for Windows software. The Chi-square test was used to assess the association between the IHC staining patterns (extent and intensity) and the histological stages of KS. The same test was applied for inter-marker comparisons within each stage. A p-value of less than 0.05 was considered statistically significant.
Reporting GuidelinesThe study was reported in accordance with STROBE guidelines.
Results
Patient Characteristics
The study cohort included 80 patients diagnosed with cutaneous KS. The group was predominantly male (n = 48, 60.0%) with 32 female patients (40.0%). The age of the patients ranged from 36 to 89 years, with a mean age of 70.85. All patients with available serology data were negative for Human Immunodeficiency Virus (HIV). Histopathological classification of the lesions demonstrated a predominance of the nodular stage (n = 45, 56.3%), followed by the plaque stage (n = 25, 31.3%) and the patch stage (n = 10, 12.5%) (Table 1).
Overall Immunohistochemical ProfileAll six markers demonstrated high diagnostic sensitivity in the KS spindle cells. The pan-endothelial markers CD31 and CD34, along with the nuclear transcription factor FLI-1, showed 100% sensitivity. The viral antigen HHV-8 and the lymphatic marker Prox1 were also highly sensitive at 98.75%. The lymphatic marker D2-40 showed 95% sensitivity.
With one key exception, the staining parameters (extent and intensity) for the evaluated markers (HHV-8, Prox1, CD34, CD31, and FLI-1) did not significantly correlate with the histological stage of the lesion (p>0.05 for all comparisons).
D2-40 Staining Intensity Correlates with Stage Progression While the staining extent of D2-40 (focal vs. diffuse) did not differ significantly across the stages (p=0.420), its staining intensity showed a strong and statistically significant correlation with histological progression (p=0.008). Strong D2-40 immunoreactivity was a characteristic feature of advanced lesions, being present in 31 of the 45 nodular stage cases (68.9%). Conversely, weak D2-40 staining was more characteristic of the earlier plaque and patch stages (Table 2).
Inter-marker Expression PatternsNodular StageWithin the 45 nodular stage lesions, direct comparisons revealed significant discordances in the expression patterns of Prox1 relative to other markers. The staining distribution of Prox1 differed significantly from that of HHV-8, CD31, D2-40, and FLI-1 (p<0.05 for all). These statistical differences were driven by a small subset of cases with discordant patterns (e.g., focal Prox1 with diffuse HHV-8), indicating subtle heterogeneity in marker expression within advanced KS (Table 3).
Plaque and Patch StagesIn the 25 plaque stage cases, a significant difference was observed between the staining patterns of Prox1 and FLI-1 (p=0.006), as well as between FLI-1 and HHV-8 (p=0.022). No other inter-marker comparisons reached statistical significance in this stage. In the 10 patch stage lesions, all markers demonstrated uniform diffuse positivity and consequently, no significant differences were found in the inter-marker comparisons (Figure 1 and Figure 2).
Discussion
This study provides a comprehensive immunohistochemical (IHC) analysis of core vascular and lymphatic endothelial markers across the full histological spectrum of KS in a large, Human Immunodeficiency Virus (HIV)-negative cohort. This specific cohort, often representing classic or sporadic KS, offers a unique opportunity to evaluate the HHV-8-driven endothelial reprogramming without the profound systemic immunodeficiency associated with AIDS-related KS. KS is recognized as an angioproliferative tumor etiologically linked to Human Herpesvirus 8 (HHV-8).1,5,6 The consistently high overall sensitivity observed for FLI-1 (100%), Prox1 (98.75%) and D2-40 (95%) confirms their robust diagnostic utility.7 These markers prove equivalent to or in some contexts potentially superior to, established pan-endothelial markers like CD34 (100% sensitivity). Specifically, D2-40 and Prox1, which are highly regarded markers of lymphatic endothelium, affirm the well-supported concept that KS spindle cells display a lymphatic differentiation phenotype.5 This finding is significant given that the conventional vascular marker CD31 has been reported to show weaker or inconsistent staining in advanced KS lesions due to targeted viral immune evasion mechanisms.10
The widespread expression of D2-40 and Prox1 across all histological stages in our cohort strongly reinforces the model that KS spindle cells originate from or are reprogrammed toward a lymphatic endothelial cell (LEC) phenotype.5 However, the most significant finding of this study was the demonstration of a statistically significant shift in D2-40 staining intensity that correlated with histological progression (p=0.008), with strong immunoreactivity being highly prevalent in advanced nodular lesions. This dynamic change suggests that podoplanin expression is not merely a static lineage marker but is actively regulated during tumor progression.4 This upregulation may reflect the increasingly dense cellularity and proliferative nature of the nodular stage, possibly indicating a more fully developed, specialized lymphatic phenotype or a response to the complex microenvironment of advanced KS.5
Furthermore, the nuclear transcription factor Prox1, the master control gene specifying LEC fate, while highly sensitive, exhibited statistically significant discordances in its staining distribution compared to viral (HHV-8) and vascular (CD31, D2-40, FLI-1) markers within the nodular stage (p<0.05).11 This heterogeneity likely reflects Prox1’s complex, dual role in KS pathogenesis, which extends beyond merely identifying lineage. Advanced studies indicate that Prox1 is a critical viral cofactor: KSHV co-opts Prox1 activity to drive viral replication and tumorigenesis.12,13,14 KSHV infection promotes the expression of Prox1 in progenitor cells, inducing a mesenchymal- to-endothelial transition (MEndT) through epigenetic reprogramming, a process mediated by viral gene products like vIL-6 and vGPCR-VEGF-A signaling.14 Importantly, Prox1 activation enhances the expression of the lytic switch protein RTA (ORF50), sustaining the viral lytic replication needed to produce infectious particles and drive pathogenesis.13 Our clinical-pathological finding of heterogeneous Prox1 expression provides in vivo evidence supporting this emerging molecular paradigm, where Prox1 acts both as a lineage marker and as a critical host factor actively manipulated by KSHV to sustain its life cycle and promote sarcomagenesis.
The finding of 100% sensitivity for FLI-1 in the spindle cell component of this cohort underscores its exceptional reliability in confirming the endothelial lineage of KS.7 As demonstrated in seminal pathological literature, FLI-1, a nuclear transcription factor, is a highly sensitive marker for both benign and malignant vascular tumors, including KS.7 Its nuclear localization provides an interpretive advantage over membranous or cytoplasmic stains, making it less susceptible to artifacts. The uniform nuclear positivity reinforces FLI-1’s critical utility in the differential diagnosis against various spindle cell mimics.7 Similarly, the observed 100% sensitivity for both CD31 and CD34 confirms their established roles as standard, first- line endothelial markers, aligning with the vast body of existing literature.4,7 Although CD31 expression is sometimes reported as weaker or decreased in nodular lesions, potentially due to KSHV-mediated degradation by the K5 protein, the finding of strong overall positivity across all stages in this study reaffirms their consistent diagnostic value.4 The lack of significant statistical differences in the overall expression parameters for these pan-vascular markers across the patch, plaque and nodular stages suggests that these core endothelial differentiation antigens are constitutively expressed from the earliest phases of KS lesion development.
Limitations
This study was subject to several limitations inherent in its retrospective design, relying exclusively on archival formalin- fixed, paraffin-embedded tissue specimens.4 Furthermore, the investigation was confined to a single-institution cohort.[Materials and Methods], which may limit the generalizability of the findings. Critically, the cohort was composed entirely of Human Immunodeficiency Virus (HIV)-negative patients.[Results], which excludes the major, prevalent AIDS-related Kaposi sarcoma (AIDS-KS) variant globally.15 This exclusion prevents a comparative analysis of marker expression across different immunological backgrounds, a context known to fundamentally impact KSHV pathogenesis and tumor growth.9
Future research should address these shortcomings through prospective, multi-center studies utilizing larger cohorts, including a well-matched group of HIV-positive patients. While a semi-quantitative approach was employed here, the development and application of quantitative image analysis are highly recommended to objectively assess the differential staining intensity of markers, such as D2-40, potentially providing more accurate results for clinical practice.4 Ultimately, correlating these refined immunohistochemical expression patterns with clinical outcomes (e.g., recurrence, survival) and established prognostic staging criteria is necessary to solidify the translational value of D2-40 and Prox1 in Kaposi sarcoma management.5
Conclusion
This study provided a robust immunohistochemical analysis across the histological spectrum of KS in an HIV-negative cohort. We confirmed that lymphatic markers Prox1 and D2-40, alongside the vascular transcription factor FLI-1, demonstrated high diagnostic sensitivity, equivalent or superior to conventional endothelial markers.7 The most significant finding was the statistically significant association identified between D2-40 staining intensity and advanced histological stage (p=0.008), suggesting that D2-40 expression is dynamically regulated during KS progression and holds potential utility as an indicator of tumor advancement. Finally, the observed inter-marker discordances regarding Prox1 expression particularly in the nodular and plaque lesions underscored its potential dual role in KSHV-driven pathogenesis beyond simple lineage definition, thereby meriting intensified molecular and clinical investigation.7
Declarations
Ethics Declarations
The authors declare that all procedures performed in this study were conducted in accordance with institutional, national, and international ethical standards.
Animal and Human Rights Statement
All procedures involving human participants were conducted in accordance with the Declaration of Helsinki and its later amendments.
Informed Consent
Informed consent was waived due to the retrospective nature of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: F.T., S.G.
Methodology: F.T., S.G.
Data curation: F.T.
Formal analysis: F.T., S.G.
Investigation: F.T., S.G.
Writing – original draft: F.T.
Writing – review & editing: S.G.
Supervision: S.G.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
IDS: Acquired immunodeficiency syndrome
FFPE: Formalin-fixed, paraffin-embedded
H&E: Hematoxylin and eosin
HHV-8: Human herpesvirus 8
HIV: Human immunodeficiency virus
IHC: Immunohistochemistry
KS: Kaposi sarcoma
KSHV: Kaposi sarcoma herpesvirus
LEC: Lymphatic endothelial cell
LANA-1: Latency-associated nuclear antigen-1
MEndT: Mesenchymal-to-endothelial transition
SPSS: Statistical Package for the Social Sciences
References
-
da Silva J, Vieira J, de Oliveira Santos E. Associative study of human herpesvirus 8 and Kaposi’s sarcoma: mapping viral oncogenic properties and the clinical scenario in oncological patients. Immunol Res. 2025;73(1):136. doi:10.1007/s12026-025-09684-9
-
Gramolelli S, Elbasani E, Tuohinto K, et al. Oncogenic herpesvirus engages endothelial transcription factors Sox18 and Prox1 to increase viral genome copies and virus production. Cancer Res. 2020;80(15):3116-3129. doi:10.1158/0008-5472.CAN-19-3103
-
Plaza JA, Sangueza OP, Giubellino A, et al. Angiosarcoma-like Kaposi sarcoma: a distinctive histomorphologic variant representing an important diagnostic pitfall. Am J Surg Pathol. 2022;46(12):1732-1738. doi:10.1097/PAS.0000000000001946
-
Pantanowitz L, Otis CN, Dezube BJ. Immunohistochemistry in Kaposi’s sarcoma. Clin Exp Dermatol. 2010;35(1):68-72. doi:10.1111/j.1365-2230.2009.03707.x
-
Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137(2):289-294. doi:10.5858/arpa.2012-0101-RS
-
Dubina M, Goldenberg G. Positive staining of tumor-stage Kaposi sarcoma with lymphatic marker D2-40. J Am Acad Dermatol. 2009;61(2):276-280.
-
Rosado FG, Itani DM, Coffin CM, et al. Utility of immunohistochemical staining with FLI1, D2-40, CD31 and CD34 in the diagnosis of acquired immunodeficiency syndrome-related and non-acquired immunodeficiency syndrome-related Kaposi sarcoma. Arch Pathol Lab Med. 2012;136(3):301-304.
-
Cho U, Cha HJ, Kim HJ, et al. FLI-1 is expressed in a wide variety of hematolymphoid neoplasms: a special concern in the differential diagnosis. Clin Exp Med. 2024;24(1):18. doi:10.1007/s10238-023-01284-x
-
Ganem D. KSHV and the pathogenesis of Kaposi sarcoma: listening to human biology and medicine. J Clin Invest. 2010;120(4):939-949. doi:10.1172/JCI40567
-
Pantanowitz L, Moses AV, Fruh K. CD31 immunohistochemical staining in Kaposi sarcoma. Arch Pathol Lab Med. 2012;136(11):1329-1330. doi:10.5858/arpa.2012-0153-LE
-
Sivakumar R, Sharma-Walia N, Raghu H, et al. Kaposi’s sarcoma-associated herpesvirus induces sustained levels of vascular endothelial growth factors A and C early during in vitro infection of human microvascular dermal endothelial cells: biological implications. J Virol. 2008;82(4):1759-1776. doi:10.1128/JVI.00873-07
-
Naipauer J, Mesri EA. The Kaposi’s sarcoma progenitor enigma: KSHV-induced MEndT-EndMT axis. Trends Mol Med. 2023;29(3):188-200. doi:10.1016/j.molmed.2022.12.003
-
Choi D, Park E, Kim KE, et al. The lymphatic cell environment promotes Kaposi sarcoma development by prox1-enhanced productive lytic replication of Kaposi sarcoma herpes virus. Cancer Res. 2020;80(15):3130-3144. doi:10.1158/0008-5472.CAN-19-3105
-
Ding Y, Chen W, Lu Z, et al. Kaposi’s sarcoma-associated herpesvirus promotes mesenchymal-to-endothelial transition by resolving the bivalent chromatin of PROX1 gene. PLoS Pathog. 2021;17(9):e1009847. doi:10.1371/journal.ppat.1009847
-
Cesarman E, Damania B, Krown SE, et al. Kaposi sarcoma. Nat Rev Dis Primers. 2019;5(1):9. doi:10.1038/s41572-019-0060-9
Figures
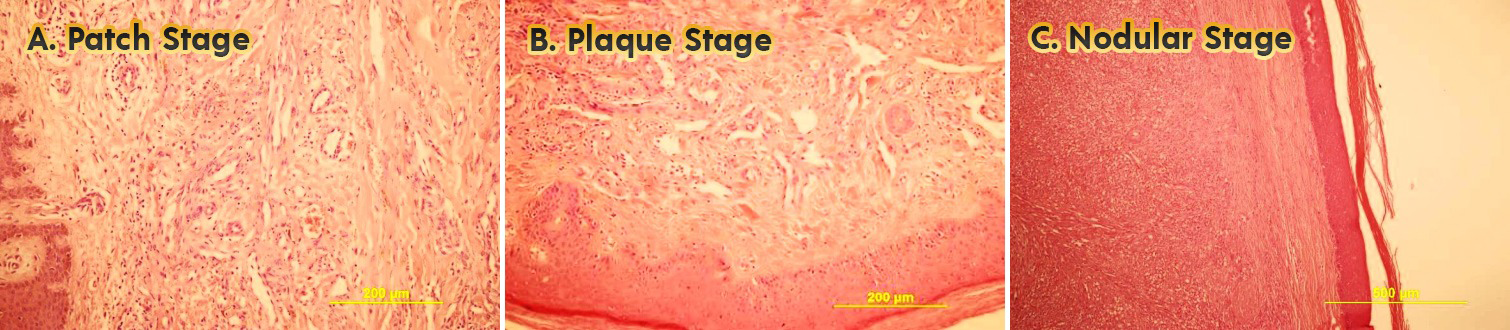
Figure 1. Histological progression of Kaposi sarcoma (H&E staining) Representative hematoxylin and eosin (H&E) images illustrating the histological stages of Kaposi sarcoma, highlighting progressive cellularity and architectural changes from patch to nodular stages. Scale bars: 100 µm (A, B), 200 µm (C). A. Patch Stage (H&E, x200): Early vascular proliferation with subtle spindle cell formation and inflammatory infiltrate. B. Plaque Stage (H&E, x200): Increased cellularity with prominent vascular slits and spindle cell aggregates. C. Nodular Stage (H&E, x100): Dense spindle cell nodules with hyaline globules and slit-like vascular spaces
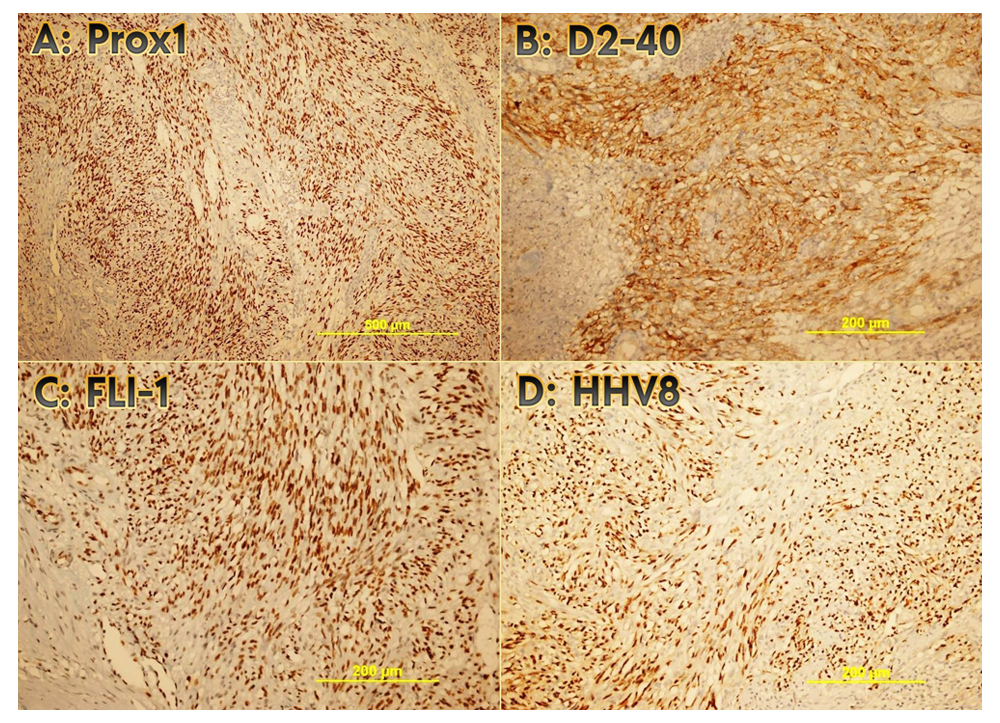
Figure 2. Immunohistochemical profiles of key markers in nodular stage Kaposi sarcoma. Representative immunohistochemical staining patterns in nodular stage Kaposi sarcoma, demonstrating high sensitivity of lymphatic (Prox1, D2-40) and endothelial (FLI-1) markers alongside the diagnostic gold standard (HHV-8). Scale bars: 200 µm (A), 100 µm (B–D). A. Prox1 (DAB, x100): Diffuse and strong nuclear positivity in spindle cells, highlighting lymphatic differentiation. B. HHV-8 (LANA-1, DAB, x200): Diffuse and strong stippled nuclear staining, confirming viral etiology. C. D2-40 (DAB, x200): Diffuse and strong membranous positivity, indicating lymphatic phenotype and progression. D. FLI-1 (DAB, x200): Diffuse and strong nuclear positivity, supporting endothelial origin
Tables
Table 1. Patient demographics and KS histological stage distribution
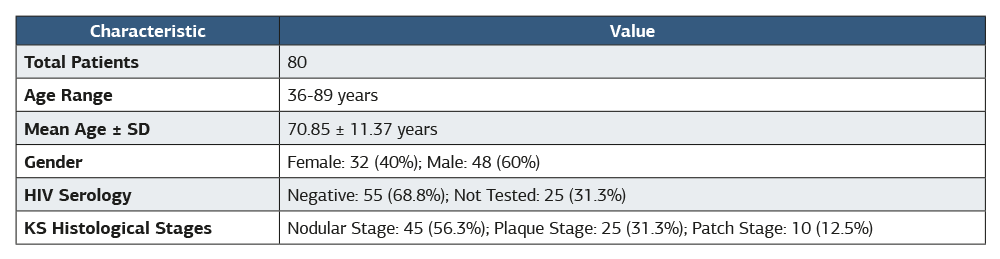
Footnotes: SD, standard deviation; KS, Kaposi sarcoma; HIV, human immunodeficiency virus. The study cohort consisted of 80 HIV-negative or HIV-untested patients with classical or endemic KS. HIV status was determined based on medical records; ‘Not Tested’ indicates the absence of a recorded serological test result in the patient’s file. Histological staging was performed ac- cording to established criteria for KS (patch, plaque, nodular).
Table 2. Immunohistochemical marker sensitivity and staining patterns across Kaposi sarcoma histological stages
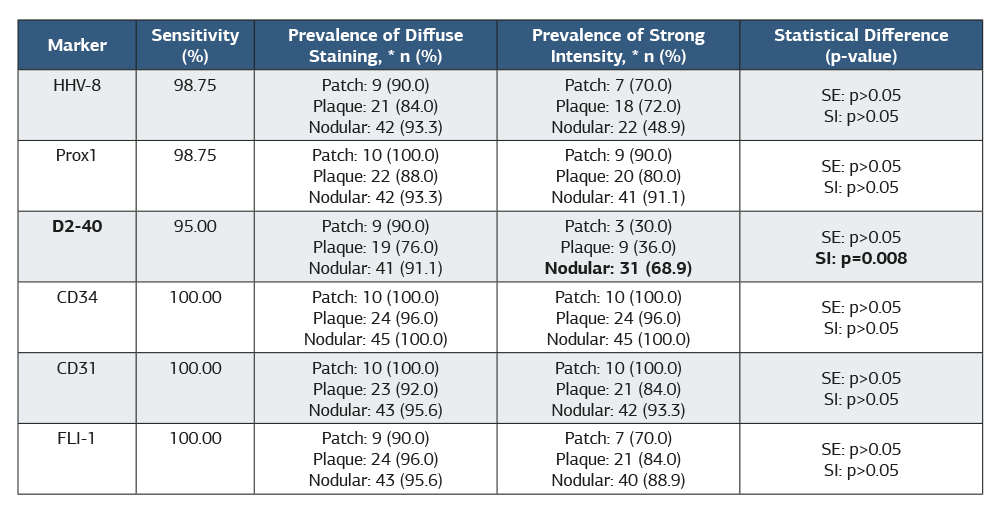
Footnotes: KS, Kaposi sarcoma; SE, Staining Extent; SI, Staining Intensity. Diffuse staining was defined as >10% of tumor cells positive. Strong intensity refers to the highest staining intensity score. P-values were derived from Chi-square tests comparing staining patterns across the three histological stages (patch, plaque, nodular). A significant difference (p<0.05) was only observed for the intensity of D2-40 staining, which increased with advancing histological stage.
Table 3. Significant inter-marker discordances in staining patterns across histological stages
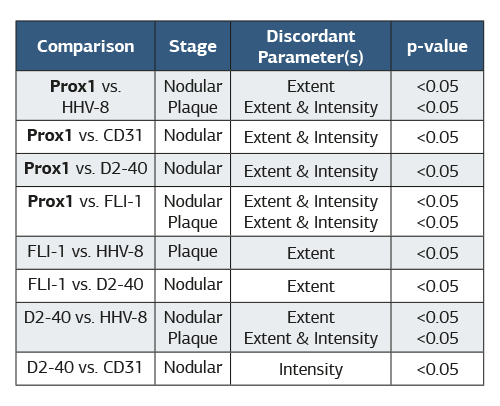
Footnotes: This table summarizes pairwise comparisons where a statistically significant difference (p<0.05) was found in immunohistochemical staining patterns between markers. Extent refers to the proportion of positive cells (focal vs. diffuse staining). Intensity refers to staining strength (weak vs. strong). The nodular stage exhibited the highest number of significant inter- marker discordances. No significant discordances were observed in the patch stage for any marker comparison. Prox1 was the marker most frequently involved in significant discordances, particularly in the nodular stage.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Fırat Tatlıdil, Seda Gün. Refining the phenotype of Kaposi sarcoma: a comparative analysis of lymphatic and endothelial marker expression during histological progression. Ann Clin Anal Med 2026;17(6):588-593. doi:10.4328/ACAM.22941
- Received:
- October 14, 2025
- Accepted:
- November 18, 2025
- Published Online:
- December 6, 2025
- Printed:
- June 1, 2026