
The role of hematological parameters in predicting high-risk human papillomavirus persistence after cervical excisional procedures: a retrospective study
Hematological parameters in post-cone HR-HPV persistence
Authors
Abstract
Aim We aim to assess the impact of hematological parameters on high-risk HPV persistence and cervical cytology outcomes after excisional treatment in patients with cervical preinvasive lesions.
Methods The study was conducted between January 2021 and January 2024 at the tertiary care center. A retrospective analysis was performed on 828 patients over the age of 24. The patients’ hematological markers before the cervical excisional procedure and hr-HPV persistence and cervical cytology results after the excisional procedure were analyzed.
Results There was no difference between the two groups with and without Hr-HPV persistence/smear abnormality in terms of hr-HPV DNA status, conization pathology results, and surgical margin status in the excisional procedure (p = 0.746, p = 0.462, p = 0.870, respectively). There was no difference in hemoglobin, neutrophil, lymphocyte, monocyte, platelet, NLR, PLR, MLR, and SIRI values between groups without and with hr-HPV persistence/smear abnormality (p = 0.240, p = 0.658, p = 0.433, p = 0.766, p = 0.198, p = 0.349, p = 0.477, p = 0.723, p = 0.545, respectively).
Conclusion In our study, no difference was detected between NLR, PLR, MLR, and SIRI values before the excisional procedure. The described hematological markers have also been shown in some studies to be valuable in predicting CIN recurrence after excisional procedures, but they have not yet been incorporated into our current practice. Comprehensive prospective studies are needed for hematological markers to be accepted in the current literature and take a place in our daily practice.
Keywords
Introduction
Despite a significant reduction in cervical cancer-related mortality rates following the introduction of the Pap smear test, cervical cancer remains one of the leading causes of death among women worldwide.
Human papillomavirus (HPV) is a DNA virus that infects the epidermis and mucous membranes and is transmitted through skin-to-skin contact. While most HPV infections resolve within two years, persistent high-risk HPV (hr-HPV) infections can lead to cervical cancer and preinvasive cervical lesions. Persistent infection with high-risk HPV (hr-HPV) is the most crucial risk factor for the development of cervical intraepithelial neoplasia (CIN), with HPV type 16 being responsible for the majority of invasive cancers, CIN 2, and CIN 3 1.
CIN is a preinvasive condition that precedes cervical cancer and is synonymous with the term “cervical dysplasia.” Cervical lesions with mitotic and immature cells limited to the lower third of the epithelium are classified as CIN 1, whereas involvement of the middle and upper thirds corresponds to CIN 2 and CIN 3, respectively 2,12. The American Society for Colposcopy and Cervical Pathology (ASCCP) recommends that women diagnosed with histologic CIN 2 or CIN 3 undergo ablative or excisional treatment to eliminate CIN and the associated HPV infection 3.
Several high-risk factors for hr-HPV persistence have been identified, including positive surgical margins, histologic CIN grade, pre- and post-treatment hr-HPV infection, glandular involvement, age, menopausal status, and immunosuppression 4,5. The causal relationship between inflammation and cancer development is well established. Increasing evidence suggests that systemic inflammatory activation by cancer cells promotes tumor progression by inducing cancer proliferation, metastasis, or angiogenesis. Chronic inflammation increases cancer risk and, even if undetectable, may play a critical role in carcinogenesis at any stage 6. Several easily measurable blood parameters reflecting systemic inflammatory response, such as increased leukocyte count, hypoalbuminemia, elevated C-reactive protein, and high cytokine levels, have been identified 7. Based on these factors, various inflammation- and immune- based prognostic scores, including the monocyte-to-lymphocyte ratio (MLR), neutrophil-to-lymphocyte ratio (NLR), platelet-to- lymphocyte ratio (PLR), and systemic inflammation response index (SIRI), have been developed to predict inflammatory responses associated with poor survival and recurrence in various cancer types 8,9,10.
This study aims to evaluate the impact of changes in hematologic parameters on hr-HPV persistence and cervical cytology outcomes following excisional procedures in patients with cervical preinvasive lesions.
Materials and Methods
Between January 2021 and January 2024, a retrospective analysis was conducted on 828 patients aged 24 years and older who underwent cervical excisional procedures due to high- risk cervical preinvasive lesions or hr-HPV DNA positivity at the Gynecologic Oncology Surgery Clinic. Patients with malignancy or carcinoma in situ confirmed by pathology, those vaccinated against HPV, and those with medical conditions or medication use that could impair immune responses were excluded.
A total of 914 patients were evaluated for eligibility. Eighty-six patients did not meet the inclusion criteria and were excluded. Among the remaining 828 patients, 176 were diagnosed with recurrent CIN 2 or CIN 3 within 12 months due to hr-HPV DNA positivity or cervical cytology abnormalities following excisional procedures. The patient selection process is illustrated in Figure 1.
Cervical excisional procedures were performed by a specialized surgical team in gynecologic oncology. Cytology and surgical specimens were evaluated by expert pathologists. Pathology and HPV DNA test results were assessed based on the 2019 ASCCP guidelines 15. Conization was performed using a scalpel (cold knife conization) or a needle-tip electrocautery device at the surgeon’s discretion. HPV DNA analysis was conducted using the Hybrid Capture 2 HPV DNA test (hc2; Qiagen, Hilden, Germany). HPV DNA and cervical cytology results at six months post-excisional procedure were compared with pre-procedure results. Patient data were obtained from the national electronic medical record database, patient files, and direct interviews. All patients underwent HPV genotyping and smear testing during gynecological examinations following excisional procedures. Besides HPV 16 and 18, HPV types 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68 were considered high-risk. A patient was classified as having HPV persistence if the control HPV DNA test at 12 months post-procedure was positive for the same HPV type detected before the procedure. Infection with a different HPV type was not considered persistent. Cervical cytopathological findings were reported according to the Bethesda System 12. In the smear, cytological abnormalities were defined as atypical squamous cells of undetermined significance (ASC-US), low-grade squamous intraepithelial lesion (LSIL), high-grade squamous intraepithelial lesion (HSIL), atypical squamous cells—cannot exclude HSIL (ASC-H), atypical glandular cells not otherwise specified (AGC-NOS), atypical glandular cells suspicious for neoplasia (AGC-neoplastic), and squamous cell carcinoma.
Prior to HPV diagnosis, complete blood counts and relevant hematologic parameters were obtained from patients’ peripheral blood. An automated hematology analyzer counted peripheral neutrophils, lymphocytes, platelets, and monocytes. The NLR was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count; the PLR was calculated by dividing the absolute platelet count by the absolute lymphocyte count; the MLR was calculated by dividing the absolute monocyte count by the absolute lymphocyte count; and the SIRI was determined using the formula: (SIRI = N x M/L).
Statistical AnalysisDescriptive statistics were presented as frequencies and percentages for categorical variables and as means ± standard deviation (SD) for continuous variables. The cutoff value for the SIRI score was calculated using receiver operating characteristic (ROC) curve analysis. Categorical variables were analyzed using the chi-square test, while continuous variables were compared using the Student’s t-test. Statistical analyses were conducted using IBM SPSS Statistics 21.0 (IBM Corp., Armonk, NY, USA) and MS Excel 2007. A p-value < 0.05 was considered statistically significant.
Ethical ApprovalThis study was approved by the Ethics Committee of Necmettin Erbakan University (Date: 2025-01-24, No: 5498).
Results
The mean age of 652 patients without hr-HPV persistence/cytological abnormalities was 38.5 ± 3.22 years, with a mean parity of 1.98 ± 0.70. Among these patients, 63.2% were smokers, and 53.7% used oral contraceptives. In contrast, the mean age of 176 patients with hr-HPV persistence/cytological abnormalities was 35.8 ± 4.47 years, with a mean parity of 2.11 ± 0.94. Among these patients, 66.5% were smokers, and 59.6% used oral contraceptives. No significant differences were observed between the two groups regarding age, parity, smoking status, or oral contraceptive use (p = 0.381, p = 0.687, p = 0.505, p = 0.320, respectively). Furthermore, there were no significant differences between the two groups in terms of hr-HPV DNA status, conization pathology results, or surgical margin status in excisional procedures (p = 0.746, p = 0.462, p = 0.870, respectively). The demographic and clinicopathological data of the patients are summarized in Supplementary Table S1.
In the group without hr-HPV persistence/cytological abnormalities, the mean hemoglobin level was 11.6 g/dL, the mean lymphocyte count was 1.9 x 10³/mm³, the mean neutrophil count was 4.5 x 10³/mm³, the mean monocyte count was 0.5 x 10³/mm³, and the mean platelet count was 245 x 10³/mm³. In the group with hr-HPV persistence/cytological abnormalities, the mean hemoglobin level was 12.3 g/dL, the mean lymphocyte count was 1.7 x 10³/mm³, the mean neutrophil count was 4.3 x 10³/mm³, the mean monocyte count was 0.5 x 10³/mm³, and the mean platelet count was 227 x 10³/mm³.
The cutoff values determined in our study were 2.5 for NLR, 130 for PLR, 0.31 for MLR, and 1.22 for SIRI. No significant differences were found between the two groups in terms of hemoglobin, neutrophil, lymphocyte, monocyte, platelet, NLR, PLR, MLR, or SIRI values (p = 0.240, p = 0.658, p = 0.433, p = 0.766, p = 0.198, p = 0.349, p = 0.477, p = 0.723, p = 0.545, respectively) (Table 1).
Discussion
HPV is one of the most common causes of sexually transmitted infections in both women and men. The etiological role of persistent high-risk (hr) HPV infection in cervical preinvasive lesions and cervical cancer is well established. Therefore, identifying high-risk HPV types and monitoring persistence is crucial for diagnosing cancer and, if possible, enabling early treatment. However, challenges remain in identifying reliable and cost-effective biomarkers to determine which patients are at higher risk of developing cervical cancer and which patients require treatment beforehand.
The etiological role of persistent hr-HPV infection in premalignant lesions and cervical cancer is well established. In our study, no significant differences were observed between the groups with and without hr-HPV persistence/cytological abnormalities in terms of pre-excisional neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), and systemic immune-inflammation index (SIRI). The systemic immune-inflammation index is a novel biomarker calculated using peripheral blood neutrophil, monocyte, and lymphocyte counts. In the study by Chao et al., SIRI was found to be correlated with cervical cancer prognosis, and high NLR, PLR, and MLR values were significantly associated with decreased overall survival in cervical cancer 10. In another study by Bilir et al., SIRI was proposed as a simple and cost- effective method for predicting hr-HPV persistence. Their study also found that NLR, PLR, and MLR were significant predictors of hr-HPV persistence. However, unlike our study, Bilir et al. included hr-HPV-positive patients who had not undergone excisional procedures 11.
In the study by Chun et al., NLR was identified as an independent prognostic factor for recurrence-free survival in patients with cervical intraepithelial neoplasia (CIN) after excisional procedures. However, unlike our study, Chun et al. focused on CIN recurrences following excisional treatment 13.
Tavares-Murta et al. conducted a study evaluating peripheral blood white blood cell counts in patients with cervical cancer and CIN. Compared to patients with CIN and early-stage cervical cancer, those with advanced-stage cervical cancer exhibited higher rates of leukocytosis, neutrophilia, lymphopenia, and NLR ≥ 5 14.
Our study is among the few in the literature that investigated the predictive value of hematological markers in hr-HPV persistence or cytological abnormalities after excisional procedures. However, its retrospective design and limited sample size are limitations. Further comprehensive studies are needed to validate our findings.
Limitations
The relatively small sample size and limited follow-up period remain notable limitations of the study.
Conclusion
Previous studies have demonstrated that hematological parameters may provide additional prognostic value beyond standard clinical and pathological parameters. However, in our study, hematological markers were not found to be predictive of hr-HPV persistence or cytological abnormalities after excisional procedures. Large-scale studies are needed for these markers to be widely accepted by clinicians and integrated into current clinical practice.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Necmettin Erbakan University (Date: 2025-01-24, No: 5498)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
References
-
Teng P, Hao M. A population‐based study of age‐related associations between vaginal pH and the development of cervical intraepithelial neoplasia. Cancer Med. 2020;9(5): 1890-902. doi:10.1002/cam4.2845.
-
Zhao XL, Xu XQ, Duan XZ, et al. Comparative performance evaluation of different HPV tests and triaging strategies using self‐samples and feasibility assessment of thermal ablation in ‘colposcopy and treat’ approach: a population‐ based study in rural China. Int J Cancer. 2020;147(5):1275-85. doi:10.1002/ijc.32881.
-
Lorincz AT, Reid R, Jenson BA, Greenberg MD, Lancaster W, Kurman RJ. Human papillomavirus infection of the cervix: relative risk associations of 15 common anogenital types. Obstet Gynecol. 1992;79(3):328-37. doi:10.1097/00006250-199203000-00002.
-
Jin J, Li L, Zhang F. Meta-analysis of high risk factors of residue or relapse of cervical intraepithelial neoplasia after conization. J Biol Regul Homeost Agents. 2015;29(2):451-8.
-
Lodi CT, Michelin MA, Lima MI, et al. Factors associated with recurrence of cervical intraepithelial neoplasia after conization in HIV-infected and noninfected women. Arch Gynecol Obstet. 2011;284(1):191-7. doi:10.1007/s00404-010-1611-1.
-
Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. CelL. 2010;140(6):883-99. doi:10.1016/j.cell.2010.01.025.
-
Templeton AJ, McNamara M, Seruga B, et al. Prognostic role of neutrophil-to- lymphocyte ratio in solid tumors: a systematic review and meta-Analysis. J Natl Cancer Inst. 2014;106(6):dju124. doi:10.1093/jnci/dju124.
-
Zahorec R. Ratio of neutrophil to lymphocyte counts--rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001;102(1):5-14.
-
Nakashima C, Kato M, Otsuka A. Cutaneous manifestations of COVID-19 and COVID-19 vaccination. J. Dermatol. 2023;50(3):280-9. doi:10.1111/1346-8138.16651.
-
Chao B, Ju X, Zhang L, Xu X, Zhao Y. A Novel prognostic marker systemic inflammation response index (SIRI) for operable cervical cancer patients. Front. Oncol. 2020;10:766-7. doi:10.3389/fonc.2020.00766.
-
Bilir F, Chkhikvadze M, Yilmaz AY, Kose O, Arıöz DT. Prognostic value of systemic inflammation response index in patients with persistent human papillomavirus infection. Ginekol Pol. 2022;93(9):705-9. doi:10.5603/GP.a2021.0200.
-
Solomon D. The 2001 bethesda systemterminology for reporting results of cervical cytology. JAMA. 2002;287(16):2114-9. doi:10.1001/jama.287.16.2114.
-
Chun S, Shin K, Kim KH, et al. The neutrophil-lymphocyte ratio predicts recurrence of cervical intraepithelial neoplasia. J. Cancer. 2017;8(2):2205-11. doi:10.7150/jca.19173.
-
Tavares-Murta BM, Mendonça MA, Duarte NL, et al. Systemic leukocyte alterations are associated with invasive uterine cervical cancer. Int J Gynecol Cancer. 2010;20(7):1154-9. doi:10.1111/igc.0b013e3181ef8deb.
-
Perkins RB, Guido RS, Castle PE, et al. 2019 ASCCP risk-based management consensus guidelines: updates through 2023. J Low Genit Tract Dis. 2024;28(1):3-6. doi:10.1097/LGT.0000000000000788.
Figures
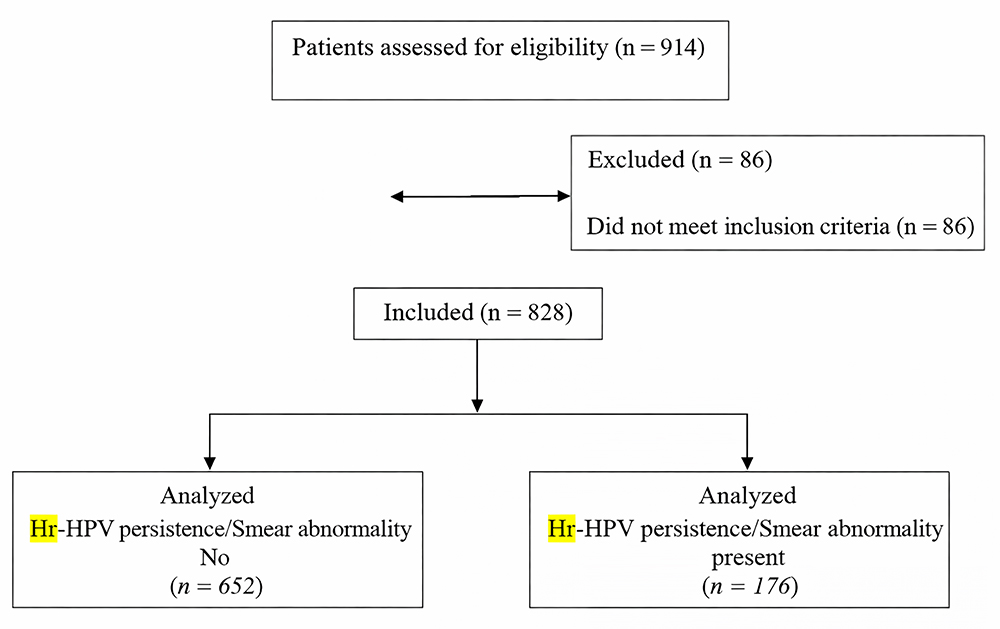
Figure 1. Illustrates the patient selection process. A total of 914 patients were assessed for eligibility. Among them, 86 patients were excluded because they did not meet the inclusion criteria. The remaining 828 eligible patients were included in the study and analyzed based on the presence or absence of HR- HPV persistence and/or smear abnormalities. Abbreviations: n = number of patients; Hr-HPV = high-risk human papillomavirus
Tables
Table 1. Status of hr-HPV persistence and cytological abnormalities after excisional procedure
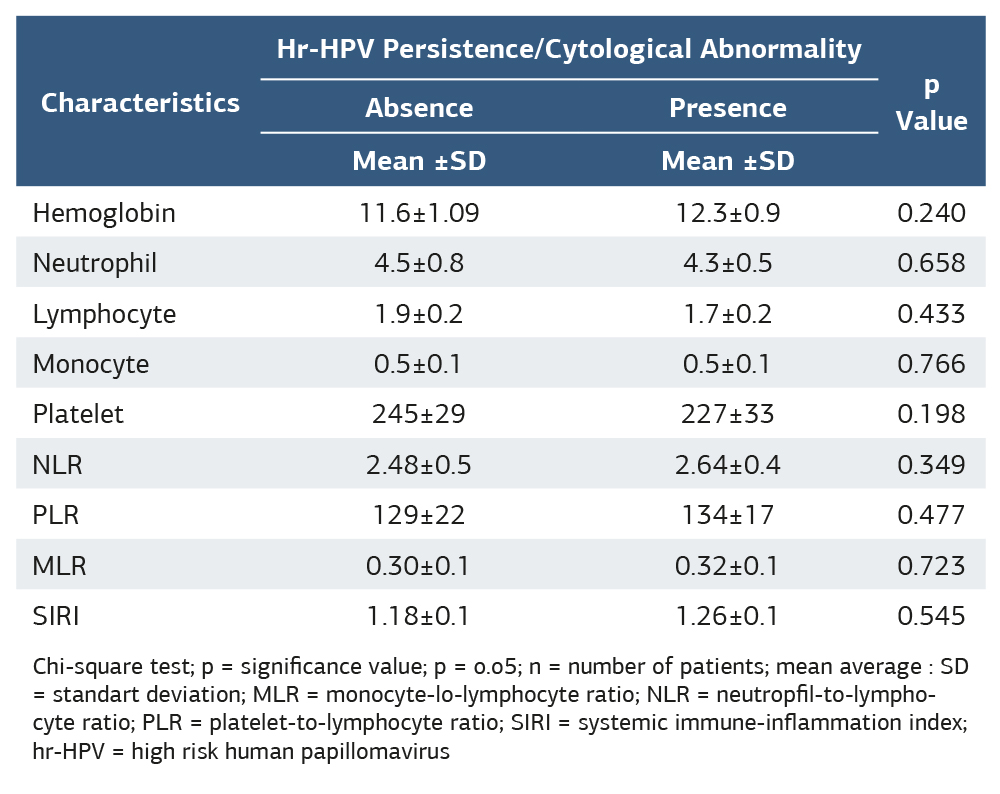
Chi-square test; p = significance value; p = o.o5; n = number of patients; mean average : SD = standart deviation; MLR = monocyte-lo-lymphocyte ratio; NLR = neutropfil-to-lympho- cyte ratio; PLR = platelet-to-lymphocyte ratio; SIRI = systemic immune-inflammation index; hr-HPV = high risk human papillomavirus
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Mustafa Şahin, Sıtkı Özbilgeç. The role of hematological parameters in predicting high-risk human papillomavirus persistence after cervical excisional procedures: a retrospective study. Ann Clin Anal Med 2026;17(2):148-151
- Received:
- October 24, 2025
- Accepted:
- December 2, 2025
- Published Online:
- December 16, 2025
- Printed:
- February 1, 2026