
Detection of carbapenem resistance in ESBL-positive and carbapenemase-producing Klebsiella pneumoniae strains using phenotypic and molecular methods
Carbapenem resistance in K. pneumoniae
Authors
Abstract
AimAntimicrobial resistance is a major global and national health concern. Carbapenem-resistant Klebsiella pneumoniae (CRKP) ranks at the top of the WHO 2024 list. K. pneumoniae causes significant morbidity and mortality among ICU patients. This study aimed to detect carbapenemase enzymes (KPC, NDM, OXA-48, and VIM) in carbapenem-resistant and ESBL-positive K. pneumoniae strains isolated from respiratory and blood samples using PCR.
MethodsSamples from 75 ICU patients hospitalized at Cerrahpaşa Medical Faculty Hospital in 2023 were analyzed. Respiratory tract (BAL, ETA, sputum) and blood cultures were processed using conventional methods (Blood agar, Chromoagar, MIO medium) and automated systems (Vitek 2 Compact, MALDI-TOF). Isolates were stored at -80 °C, subcultured, and subjected to DNA extraction. Carbapenemase genes (KPC, NDM, OXA-48, VIM) were identified by Real-Time PCR.
ResultsOf the 75 patients, 62.7% were male, with a mean age of 62.6 ± 18.3 years. Respiratory tract samples comprised 56%, and blood cultures 44%. Resistance rates were 52% for imipenem and 90.7% for meropenem. Gene prevalence was NDM 92%, OXA-48 84%, KPC 81.3%, and VIM 78.7%. Coexistence patterns included KPC + OXA-48 + NDM + VIM (70.7%) and OXA–48 + NDM (8%). No carbapenemase genes were detected in 5.3% of isolates. No significant differences were found by gender, age, or ICU type (p>0.05).
ConclusionICU infections caused by carbapenemase-producing K. pneumoniae pose a serious risk. Regular surveillance of carbapenemase-producing bacteria is crucial for infection control and antimicrobial stewardship.
Keywords
Introduction
Antimicrobial resistance has become a critical global and national public health issue.1 In the 2024 World Health Organization (WHO) priority list, carbapenem-resistant K. pneumoniae ranks first.2 K. pneumoniae is a major cause of severe nosocomial infections in intensive care units (ICUs), including sepsis, pneumonia, urinary tract infections, catheter-associated infections, and surgical site infections. The greatest concern is its multidrug resistance, which increases morbidity and mortality among ICU patients.1,3
In Türkiye, carbapenem-resistant Enterobacteriaceae began emerging after 2010, initially as localized outbreaks, but became endemic by 2014–2015.1 According to the 2020 CAESAR (Central Asian and European Surveillance of Antimicrobial Resistance) surveillance report, the carbapenem resistance rate in K. pneumoniae isolates in Türkiye reached 39%.4
Within Enterobacteriaceae, Klebsiella spp. are opportunistic pathogens, with K. pneumoniae responsible for about 70% of infections.1 Normally a part of the human microbiota, it can colonize the gastrointestinal tract and other body sites.5 In ICUs, it is one of the most frequently isolated pathogens, causing respiratory, urinary, bloodstream, and wound infections.3
Treatment usually involves aminoglycosides and beta-lactam antibiotics; however, the emergence of extended-spectrum beta-lactamases (ESBLs) has limited their effectiveness.6 Although beta-lactam/beta-lactamase inhibitor combinations (e.g., ampicillin–sulbactam, amoxicillin–clavulanic acid) were developed, K. pneumoniae has also developed resistance to these agents. Consequently, carbapenems such as imipenem and meropenem became widely used, but overuse has led to rapidly increasing carbapenem resistance.7
Carbapenem resistance may result from intrinsic or plasmid-mediated mechanisms, including enzymatic inactivation, target-site modification, and efflux pumps.8
Carbapenemases are key resistance mechanisms that hydrolyze carbapenems, making them ineffective. These enzymes are often plasmid-encoded and highly transmissible. According to the Ambler classification, carbapenemases are divided into three classes: A, B, and D. Classes A and D are serine carbapenemases with serine at their catalytic sites, while Class B enzymes are metallo-β-lactamases containing zinc.9 The most common Class A enzyme is KPC (Klebsiella pneumoniae carbapenemase). Class B includes NDM (New Delhi metallo-β-lactamase), IMP (Imipenemase Metallo-β-lactamase), and VIM (Verona integron-encoded metallo-lactamase), while Class D includes oxacillinases such as OXA-48 (Oxacillin-hydrolyzing carbapenemase), first reported in K. pneumoniae isolates from Türkiye.10
This study aimed to investigate carbapenemase enzymes in K. pneumoniae isolates from respiratory and blood samples of ICU patients at Cerrahpaşa Medical Faculty Hospital between January 1 and December 31, 2023. The presence of the most frequently detected carbapenemases—KPC, NDM, VIM, and OXA-48—was evaluated using PCR.
Materials and Methods
Bacterial IsolatesThe study included isolates obtained from 75 patients hospitalized in the Intensive Care Unit (ICU) at İstanbul University–Cerrahpaşa, Cerrahpaşa Faculty of Medicine, Prof. Dr. Murat Dilmener Hospital, between January 1, 2023, and December 31, 2023. A total of 42 respiratory tract specimens (sputum, endotracheal aspirate, bronchoalveolar lavage) and 33 blood culture specimens submitted to the Medical Microbiology Laboratory were processed. Klebsiella pneumoniae strains isolated from these samples and confirmed as ESBL-positive were included in the study. The isolates were stored in Eppendorf tubes containing 10% glycerol (HiMedia, India) and kept at –80 °C until the day of the study.
Identification of Bacteria: The isolates stored in TSB medium (Tryptic Soy Broth, Hi Media, India) at -80 °C were subcultured at Chromogenic Agar (Across Bio, Türkiye) and incubated 37 °C for 24 hours.11 Colonies showing a mucoid, metallic-blue appearance were identified as K. pneumoniae. These colonies were further cultured on 5% sheep blood agar and incubated for 18–20 hours. Grown colonies were tested in Indole Motility Ornithine (MIO) medium, and isolates that were negative for motility, ornithine decarboxylase, and indole were confirmed as K. pneumoniae. Additional confirmation was performed using automated identification systems from bioMérieux (France) and Bruker MALDI Biotyper Sirius (Bruker, USA).
Detection of Antibiotic Resistance: A total of 75 K. pneumoniae isolates were tested. For antimicrobial susceptibility testing, isolates were inoculated onto Mueller–Hinton (MH) agar medium, and the Kirby–Bauer disk diffusion method was used. MH agar plates were incubated at 37 °C for 18–20 hours. The following day, inhibition zone diameters around the antibiotic disks were measured, and susceptibility was interpreted according to EUCAST criteria. Using this method, both ESBL production and carbapenemase activity were also investigated. To detect ESBL production, cephalosporin group antibiotics such as cefuroxime, cefoxitin, ceftazidime, cefotaxime, and cefepime were tested, while carbapenemase activity was assessed using carbapenems, namely imipenem and meropenem.
The presence of ESBL was evaluated by the double-disk synergy test. Enhancement of the inhibition zone around cefepime (FEP) and ceftazidime (CAZ) disks in the vicinity of the amoxicillin– clavulanate (AMC) disk, due to the effect of clavulanic acid, was interpreted as ESBL positivity.12,13
Meropenem is considered the most reliable antibiotic for detecting carbapenemase production, with high sensitivity and specificity. The EUCAST screening breakpoints for carbapenemase-producing Enterobacteriaceae are used in this study.12
Detection of Antibiotic Resistance by Molecular MethodsColonies of K. pneumoniae grown on 5% sheep blood agar were transferred into Eppendorf tubes containing 1 mL of physiological saline and stored at +4 °C for 24 hours for isolation. DNA extraction was performed using the MikroLine Pathogen DNA/RNA Purification Kit (Türkiye). The primer dilution ratios, annealing temperatures, and melting temperatures of the targeted gene regions were used as described by Doğan et al.14 The primers were synthesized by Sentromer DNA Technologies (Türkiye). For RT-PCR reactions, qPCR BIO SyGreen® Blue Mix was used, and amplification and analysis were performed on the Gentier 96E Real-Time PCR system. According to a study by Doğan et al., primers initially prepared as 100 µM stock solutions were diluted 1:10 to obtain 10 µM intermediate stocks. These 10 µM primer stocks were used to prepare RT-PCR reaction mixtures.14
Using the commercial kit “Antibacterial Resistance Panel Real-Time PCR (KPC, NDM, VIM, IMP, OXA-48, CTX-M)” (Bioeksen, Türkiye), the presence of KPC, NDM, OXA-48, and VIM was demonstrated. These isolates were used as positive controls for PCR experiments.
Ethical ApprovalThe study was approved by the Ethics Committee of İstanbul University-Cerrahpaşa (Date: 17.04.2024, Decision No: 2024/73).
Statistical AnalysisData analysis was performed using the software package “SPSS for Windows 23.” The significance of differences between categorical variables was assessed using the Pearson Chi-square test, Fisher’s exact test, and Student’s t-test. Results were considered statistically significant at p<0.05.
Reporting GuidelinesThis study is reported in accordance with the STROBE guideline.
Results
The K. pneumoniae isolates were found to be 96.0% resistant and 4.0% intermediately susceptible to cefepime, a fourth- generation cephalosporin used to determine ESBL positivity. The percentage distribution (%) of antibiotic susceptibility in ESBL- positive and carbapenemase-positive Klebsiella pneumoniae isolates is shown in Table 1. Among carbapenem antibiotics, resistance to imipenem was 52.0%, while susceptibility was 48.0%; resistance to meropenem was 90.7%, while susceptibility was 9.3% (Table 1).
According to the Real-Time PCR study results, the detection rates of carbapenemase enzymes in 75 K. pneumoniae strains were determined as follows: 92% NDM, 84% OXA-48, 81.3% KPC, and 78.7% VIM (Table 2).
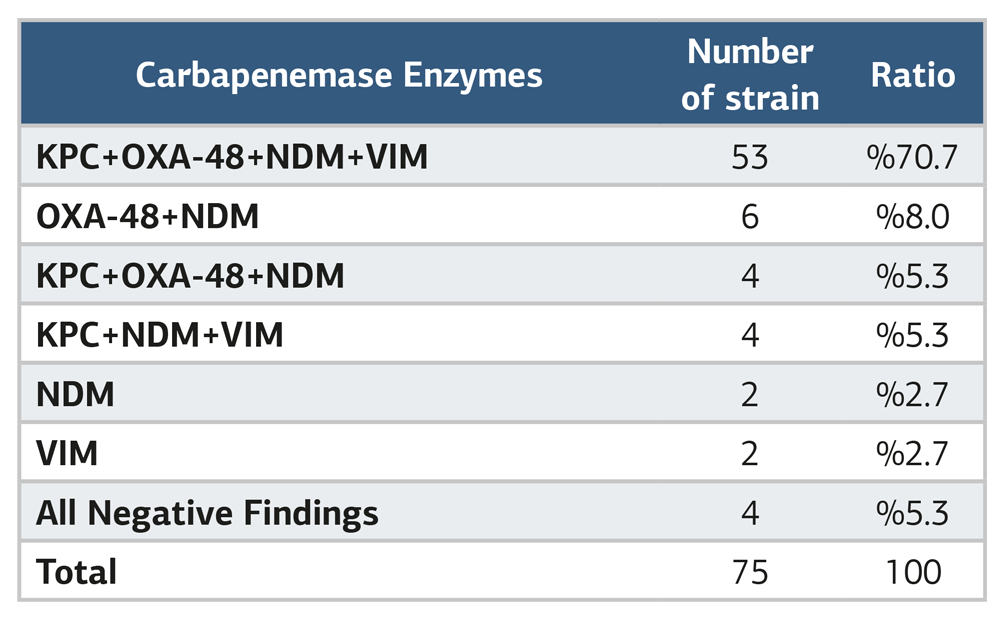
According to the Real-Time PCR results, the coexistence patterns of carbapenemase enzymes responsible for carbapenem resistance in K. pneumoniae isolates are shown in Table 3. In total, among 75 K. pneumoniae strains, four enzymes (KPC + OXA-48 + NDM + VIM) were detected together in 70.7%, two enzymes (OXA-48 + NDM) in 8.0%, three enzymes (KPC + OXA-48 + NDM) in 5.3%, three enzymes (KPC + NDM + VIM) in 5.3%, NDM alone in 2.7%, VIM alone in 2.7%, and all enzymes were negative in 5.3% of the isolates (Table 3).
This study investigated the distribution of carbapenemase enzymes by gender, age group (above and below 60 years), ICU unit, and sample type (blood culture samples and respiratory tract samples). Among these parameters, the only statistically significant differences were observed in the distribution of sample types (respiratory tract vs. blood culture) for the presence of KPC (p=0.022) and VIM (p=0.025) enzymes. When the distribution of carbapenemase enzymes was examined by sample type, KPC (90.5%) and VIM (88.1%) enzymes in respiratory tract samples were significantly higher than KPC (69.7%) and VIM (66.7%) in blood culture samples (p<0.05).
Discussion
In this study, enzymatic resistance, one of the most important mechanisms of antibiotic resistance, was considered, and the carbapenemase enzymes KPC, NDM, VIM, and OXA-48, which cause resistance in K. pneumoniae, can be transmitted via horizontal gene transfer and are the most commonly detected, were examined.15 A total of 75 patient samples and data, obtained from respiratory and blood culture specimens of patients in the ICU and found positive for carbapenemase and ESBL resistance, were included in this study. Of the 75 patients included, 47 (62.7%) were male, and 28 (37.3%) were female. In studies conducted in our country, the gender distribution of patients with K. pneumoniae was similarly reported as 38.8–59% male and 41–60.2% female.3,5,16 The age range of the patients varied between 20 and 93 years, with a mean value of 62.56 ± 18.29 years. Of the cases included in the study, 37.3% were female. When the data were examined, although the percentage of positivity (%) for the four enzymes was higher in females than in males, the difference was not statistically significant (p>0.05).
Interestingly, in our study, all K. pneumoniae isolates that were carbapenemase- and ESBL-positive, obtained from respiratory samples of ICU patients, were from female patients. However, when the distribution of carbapenemase enzymes by gender, age (above vs. below 60), ICU units, and within the respiratory samples themselves was examined, no statistically significant differences were found (p>0.05).
In our study, antibiotic resistance was determined as follows: cefepime, a fourth-generation cephalosporin, was 96.0% resistant; imipenem, a carbapenem antibiotic, was 52.0% resistant and 48.0% sensitive; meropenem was 90.7% resistant and 9.3% sensitive. Studies conducted in our country on K. pneumoniae isolates from ICUs reported similar resistance rates: Genişel et al. found cefepime resistance at 87.88%, imipenem resistance at 60.61%, and meropenem resistance at 84.85% in their 2021 study.5 These results were similar to the resistance rates of K. pneumoniae isolates from our hospital ICU. In another study conducted by Uyanık et al. in 2021, imipenem resistance was 26.0% and meropenem resistance 24.4%, with 46% ESBL positivity, which was relatively low.17
The Real-Time PCR results revealed the percentages of carbapenemase enzymes as follows: NDM 92%, OXA-48 84%, KPC 81.3%, and VIM 78.7%. In a study by Telli et al., the distribution of resistance enzymes was reported as OXA-48, NDM, KPC, and VIM, with counts of 113 (38.8%), 32 (11.0%), 7 (2.4%), and 5 (1.7%), respectively.1 The distribution of strains carrying multiple resistance genes was as follows: OXA-48 + NDM 123 (42.3%), OXA-48 + KPC two strains, OXA-48 + VIM one strain, NDM + KPC one strain, and NDM + IMP one strain. In a study by Genç et al., the most frequent single resistance gene was OXA-48 (81.05%), followed by NDM (38.9%), while multiple resistance genes were reported as OXA-48 + KPC and KPC + NDM.18 Since our study included ESBL-positive and carbapenem-resistant K. pneumoniae strains, the presence of carbapenemase enzymes causing resistance was expected. Determining the prevalence of frequently observed resistance-causing enzymes (OXA-48, NDM, KPC, and VIM) was our primary objective, and their presence was indeed high. In our study, the NDM, OXA-48, KPC, and VIM enzymes were negative in 4 samples (5.3%) (see Table 3). Based on the antibiogram of these samples, carbapenem resistance was detected, suggesting that other enzymes (e.g., OXA-181) may be responsible.
Interestingly, all four negative samples (resistance-causing enzymes; OXA-48, NDM, KPC, and VIM) were from blood cultures. The carbapenemase enzymes showing statistically significant differences between blood and respiratory samples were KPC and VIM (p<0.05).
Studies on resistance genes of K. pneumoniae isolates from ICUs have reported the following results: Moussa et al. reported NDM, OXA-48, and VIM at 2.5%, 81%, and 6.3%, respectively, in all K. pneumoniae strains isolated from ICU patients between 2019 and 2022.19 Demir and Nakipoglu reported NDM and OXA-48 at rates of 43.2% and 18.2%, respectively, among 2021 ICU isolates with carbapenemase, while KPC and VIM were not detected.20 They found co-occurrence of NDM and OXA-48 at 36.4%. In this study, the enzymes we investigated (NDM, OXA-48, KPC, and VIM) were found at higher rates in respiratory samples. In respiratory samples, NDM was 97.6%, OXA-48 90.5%, KPC 90.5%, and VIM 88.1%, whereas in blood samples, NDM was 84.8%, OXA-48 75.8%, KPC 69.7%, and VIM 66.7%. KPC (90.5%) and VIM (88.1%) in respiratory samples were significantly higher than KPC (69.7%) and VIM (66.7%) in blood cultures (p<0.05). Overall, enzyme prevalence was lower in blood samples compared to respiratory samples.
The IMP enzyme was excluded from this study because its detection probability in studies conducted in our country was low or nearly absent.14,21,22,23
According to Real-Time PCR results, the co-occurrence of carbapenemase enzymes in K. pneumoniae isolates was as follows: four enzymes (KPC + OXA-48 + NDM + VIM) together in 70.7%, OXA-48 + NDM in 8.0%, KPC + OXA-48 + NDM in 5.3%, KPC + NDM + VIM in 5.3%, NDM alone in 2.7%, VIM alone in 2.7%, and negative for all enzymes in 5.3% of the 75 isolates (Table 3). The four-enzyme combination (KPC + OXA-48 + NDM + VIM) was notably high at 70.7% (Table 3).
Previous studies reported co-occurrence of resistance genes as follows: Demir and Nakipoglu found NDM + OXA-48 together at 36.4%; Telli et al. reported multiple resistance genes at 42.3% for OXA-48 + NDM, two strains for OXA-48 + KPC, one strain for OXA-48 + VIM, one strain for NDM + KPC, and one strain for NDM + IMP. Okalin et al. reported OXA-48 + NDM at 15.5%. Süzük Yıldız et al. found OXA-48 + NDM-1 at 12.6%, KPC + NDM-1 at 2.8%, and OXA-48 + VIM at 0.5%.1,15,20,23
The inclusion criteria for the study were as follows: a) The patient being hospitalized in the Intensive Care Unit (ICU), b) The submitted specimen being a respiratory tract sample or a blood culture, and c) The isolation of K. pneumoniae strains showing extended-spectrum β-lactamase (ESBL) positivity and carbapenem resistance. Patients of all age groups and both sexes were included in the study.
The exclusion criteria were as follows: a) Hospitalization in a service other than the ICU, b) Specimens other than respiratory tract or blood culture samples (e.g., wound, urine, etc.), and c) Isolation of K. pneumoniae strains that were ESBL-negative and susceptible to carbapenems.
Limitations
This study was conducted at a single center with a relatively limited sample size. Only KPC, NDM, OXA-48, and VIM carbapenemase genes were investigated, while other carbapenemase genes and resistance mechanisms were not evaluated. Therefore, the findings may not be generalizable to other healthcare settings.
Conclusion
Detection of ESBL in clinical isolates and monitoring antibiotic resistance patterns are crucial for preventing hospital- and community-acquired infections and guiding appropriate antibiotic therapy.24 In conclusion, the resistance profiles of K. pneumoniae strains, which are prominent in hospital infections and associated with morbidity and mortality, should be monitored by microbiology and hospital infection control laboratories, and tracking resistance-causing enzymes is of significant importance.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments, or comparable ethical standards.
Informed Consent
Informed consent was waived.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare no conflict of interest.
Funding
This study was supported by the Research Support Unit (BAP) of İstanbul University-Cerrahpaşa, project no: TYL-2024-37881.
Author Contributions (CRediT Taxonomy)
Conceptualization: B.K., Y.U., Ö.K.
Methodology: B.K., Y.U., G.A.
Investigation: B.K., H.Y.A.
Data Curation: B.K.
Formal Analysis: G.C., B.K.
Writing – Original Draft: B.K.
Writing – Review & Editing: Y.U., G.A., Ö.K.
Supervision: Y.U., Ö.K.
AI Usage Disclosure
The authors declare that artificial intelligence (AI) was not used in any stage of the preparation, analysis, or writing of this manuscript.
Abbreviations
BAL: Bronchoalveolar lavage
CAESAR: Central asian and European Surveillance of Antimicrobial Resistance
ESBL: Extended-spectrum beta-lactamase
ETA: Endotracheal aspirate
EUCAST: European committee on antimicrobial susceptibility testing
ICU: Intensive care unit
KPC: Klebsiella pneumoniae carbapenemase
MALDI-TOF: Matrix-assisted laser desorption/ionization time-of-flight
MIO: Motility indole ornithine
NDM: New Delhi metallo-β-lactamase
OXA-48: Oxacillinase-48
PCR: Polymerase chain reaction
TSB: Tryptic soy broth
VIM: Verona integron-encoded metallo-β-lactamase
WHO: World Health Organization
References
-
Telli M, Çoban A. Bir üniversite hastanesinde bazı karbapenem dirençli Enterobacterales türlerinde direnç enzimlerinin ve klonal ilişkilerinin belirlenmesi [Determining the resistance enzymes and clonal diversity of various carbapenem-resistant Enterobacterales strains in a tertiary care hospital]. Turk Mikrobiyol Cemiy Derg. 2024;54(3):201-207. doi:10.54453/tmcd.2024.26680
-
World Health Organization. WHO bacterial priority pathogens list, 2024: bacterial pathogens of public health importance to guide research, development and strategies to prevent and control antimicrobial resistance. Published May 17, 2024. Accessed October 27, 2025. https://www.who.int/publications/i/item/9789240093461. doi:10.1097/01.naj.0001027648.46160.ae
-
Büyüktuna SA, Hasbek M, Çelik C, et al. Klebsiella pneumoniae infections in the intensive care unit: risk factors related to carbapenem resistance and patient mortality. Mikrobiyol Bul. 2020;54(3):378-391.
-
World Health Organization Regional Office for Europe. Annual report 2020. Central Asian and European Surveillance of Antimicrobial Resistance. Published October 1, 2020. Accessed October 27, 2025. https://www.who.int/europe/publications/i/item/WHO-EURO-2020-3469-43228-60585. doi:10.2471/b09585
-
Genişel N, Özcan N, Gül K, et al. Molecular investigation of carbapenem and colistin resistance mechanisms in Klebsiella pneumoniae bloodstream isolates. FABAD J Pharm Sci. 2021;46(3):289-298.
-
Kahraman EP, Karakeçe E, Erdoğan F, Uluyurt H, Köroğlu M, Çiftci İH. Klebsiella pneumoniae izolatlarının antibiyotiklere direnç durumlarının değerlendirilmesi [Evaluation of antimicrobial resistance rates of Klebsiella isolates]. Ortadogu Tip Derg. 2017;9(1):12-18. doi:10.21601/ortadogutipdergisi.291133
-
Arato V, Raso MM, Gasperini G, Berlanda Scorza F, Micoli F. Prophylaxis and treatment against Klebsiella pneumoniae: current insights on this emerging antimicrobial-resistant global threat. Int J Mol Sci. 2021;22(8):4042. doi:10.3390/ijms22084042
-
Codjoe FS, Donkor ES. Carbapenem resistance: a review. Med Sci (Basel). 2017;6(1):1. doi:10.3390/medsci6010001
-
Nordmann P, Poirel L. Epidemiology and diagnostics of carbapenem resistance in gram-negative bacteria. Clin Infect Dis. 2019;69(suppl 7). doi:10.1093/cid/ciz824
-
Gümüş HH, Köksal F. Carbapenem-resistant Klebsiella pneumoniae: resistance mechanisms, epidemiology, and mortality. Flora. 2023;28(2):131-143. doi:10.5578/flora.20239913
-
Abdullah AM, Abdullah RM, Salman SL. Use of chromogenic agar in detection of urinary tract pathogens and use of chromogenic agar in detection of urinary tract pathogens and antimicrobial susceptibility. J Fac Med Baghdad. 2009;51(1):39-42. doi:10.32007/jfacmedbagdad.5111168
-
European Committee on Antimicrobial Susceptibility Testing. EUCAST guideline for the detection of resistance mechanisms and specific resistances of clinical and/or epidemiological importance. Published July 2017. Accessed October 27, 2025. https://www.eucast.org/resistance_mechanisms.
-
Hoşgör M, Özkan F, Yapar N, Tünger A, Özinel MA. Genişlemiş spektrumlu beta-laktamazların belirlenmesinde çift diskli sinerji testi ile üç boyutlu yöntemin karşılaştırılması [Comparison of double-disk synergy and three-dimensional tests in detection of extended spectrum beta-lactamases]. Klimik Derg. 1998;11(2):59-60.
-
Dogan M, Ugrakli S. Phenotypic and genotypic identification of carbapenem-resistant Klebsiella pneumoniae and determination of antibiotic susceptibility. Selcuk Med J. 2023;39(2):75-83. doi:10.30733/std.2023.01639
-
Okalin ŞŞ, Sarı Kaygısız AN, Ergon MC, Öktem İMA. Karbapenem dirençli Enterobacterales izolatlarında karbapenemaz genlerinin araştırılması: Dokuz Eylül Üniversitesi Hastanesi’nden ilk KPC bildirimi [Investigation of carbapenemase genes in carbapenem-resistant Enterobacterales isolates: first KPC report from Dokuz Eylul University Hospital]. Turk Mikrobiyol Cemiy Derg. 2021;51(4):375-381. doi:10.5222/tmcd.2021.94899
-
Yürek M, Cevahir N. Investigation of virulence genes and carbapenem resistance genes in hypervirulent and classical isolates of Klebsiella pneumoniae isolated from various clinical specimens. Mikrobiyol Bul. 2023;57(2):188-206. doi:10.5578/mb.20239915
-
Uyanık Parlak A, Güdücüoğlu H, Parlak M, Bayram Y, Otlu B. Klebsiella pneumoniae suşlarında OXA-48 ve alt türevlerinin araştırılması ve fenotipik yansıma [The investigation of OXA-48 and sub-derivatives in Klebsiella pneumoniae strains and phenotypic reflection]. ANKEM Derg. 2021;35(1):1-8. doi:10.5222/ankem.2021.001
-
Genç S, Kolaylı F, Özçelik EY. Molecular characterization of carbapenemase-producing Klebsiella pneumoniae strains by multiplex PCR and PFGE methods: the first K pneumoniae isolates co-producing OXA-48/KPC and KPC/NDM in Türkiye. J Infect Chemother. 2022;28(2):192-198. doi:10.1016/j.jiac.2021.10.009
-
Moussa B, Hmami F, Arhoun B, et al. Intense intestinal carriage of carbapenemase-producing Klebsiella pneumoniae co-harboring OXA-48, KPC, VIM, and NDM among preterm neonates in a Moroccan neonatal intensive care unit. Cureus. 2023;15(12). doi:10.7759/cureus.50095
-
Demir HK, Nakipoglu Y. Investigation of the prevalence of carbapenem resistance genes in faecal carriage of carbapenem-resistant Klebsiella spp isolates by multiplex real-time PCR method. J Infect Dev Ctries. 2023;17(11):1606-1612. doi:10.3855/jidc.17892
-
Cetinkol Y, Yildirim AA, Telli M, Calgin MK. The investigation of oxacillinase/metallo-beta-lactamase genes and clonal analysis in carbapenem-resistant Klebsiella pneumoniae. Infez Med. 2016;24(1):48-53.
-
Kutlu HH, Us E, Tekeli A. Investigation of carbapenemase genes and molecular epidemiology of Enterobacteriaceae strains isolated between 2010 and 2014 in a university hospital. Mikrobiyol Bul. 2018;52(1):1-12.
-
Süzük Yıldız S, Şimşek H, Bakkaloğlu Z, et al. The epidemiology of carbapenemases in Escherichia coli and Klebsiella pneumoniae isolated in 2019 in Türkiye. Mikrobiyol Bul. 2021;55(1):1-16. doi:10.5578/mb.20124
-
Temiz H, Özbek E, Gür Vural D, Özekinci T. Evaluation of antimicrobial resistance rates of Klebsiella isolates. Turk Mikrobiyol Cem Derg. 2015;45(2):68-74.
Tables
Table 1. Percentage distribution (%) of antibiotic susceptibility in ESBL-positive and carbapenemase-positive Klebsiella pneumoniae isolates
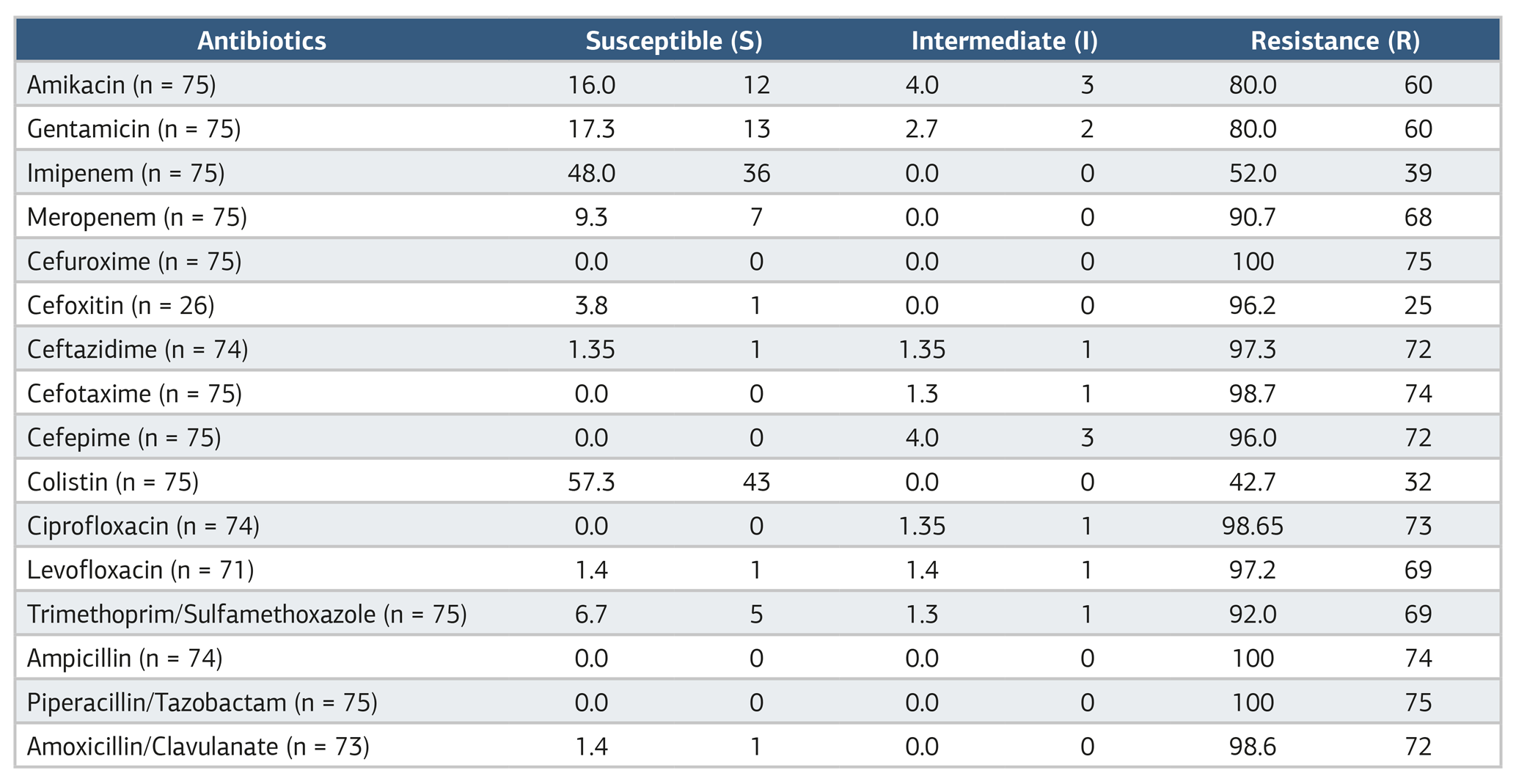
Table 2. Percentage distribution (%) of carbapenemase enzymes in ESBL-positive and carbapenem-resistant Klebsiella pneumoniae isolates
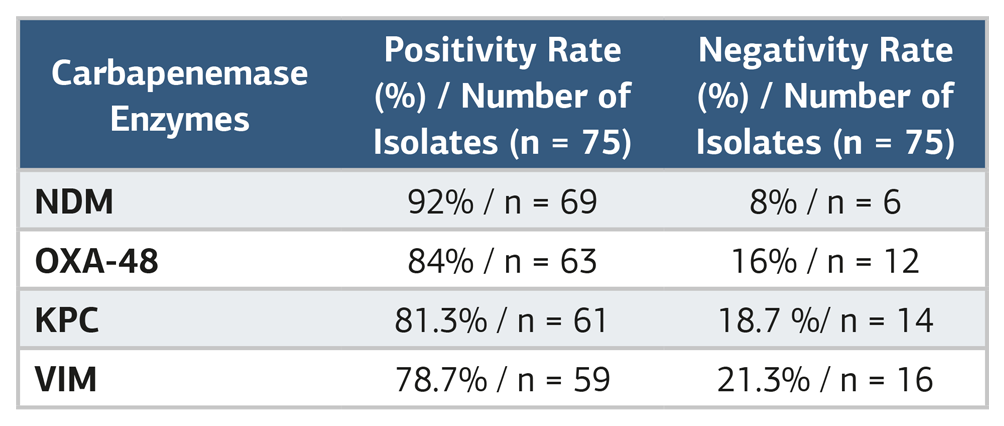
Table 3. The presence of carbapenemase enzymes alone or in combination in Klebsiella pneumoniae isolates
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Büşra Kayın, Yavuz Uyar, Gökhan Aygün, Hatice Yaşar Arsu, Günay Can, Ömer Küçükbasmacı. Detection of carbapenem resistance in ESBL-positive and carbapenemase-producing Klebsiella pneumoniae strains using phenotypic and molecular methods. Ann Clin Anal Med 2026;17(7):676-680. doi:10.4328/ACAM.22964
- Received:
- October 31, 2025
- Accepted:
- December 2, 2025
- Published Online:
- January 3, 2026
- Printed:
- July 1, 2026