
Morphometric analysis, prevalence, and positional relationships of the accessory mental foramen using multi-detector computed tomography
Morphometry of the accessory mental foramen
Authors
Abstract
AimKnowledge of the mental foramen (MF) and accessory mental foramen (AMF) is crucial for preventing complications such as paresthesia, bleeding, and anesthesia failure during dental implant placement and surgical procedures. This study aimed to analyze the morphometric measurements of the MF and AMF, as well as the prevalence and location of the AMF in detail.
MethodsIn this study, multi-detector computed tomography (MDCT) images of 350 patients (700 mandibles) were retrospectively examined. Measurements included the heights, widths, and distances between the MF and AMF. The positions of the AMF relative to the teeth and MF were also examined.
ResultsA total of 16 AMFs were detected in 15 patients (one bilateral), with a prevalence of 2.29%. The height and width of the MF were statistically significantly greater in men than in women (p<0.05). The mean AMF height was 1.23±0.40 mm, the width was 1.51±0.45 mm, and the AMF-MF distance was 2.39±2.08 mm. AMFs were most commonly located between the first and second premolar teeth (37.50%). The most common locations relative to the MF were infero-posterior (31.25%) and supero-anterior (31.25%).
ConclusionAlthough AMF prevalence is low (2.29%), it is clinically significant due to its relationship with neurovascular structures. The notable frequency of superior-anterior locations, in particular, requires attention in implant and maxillofacial surgical planning. Therefore, the use of three-dimensional (3D) imaging methods prior to surgery may help reduce the risk of complications.
Keywords
Introduction
The mental foramen (MF) is an important anatomical structure located on both sides of the mandible through which the inferior alveolar nerve and vessels exit the mandible. This structure provides sensory innervation to the lower lip, chin skin, buccal mucosa, and gums.1,2 The location and morphometric characteristics of the MF are critically important in dental implant surgery, endodontic treatments, orthognathic surgery, and neurovascular block applications.3,4
Smaller accessory openings may sometimes be found around the MF; these are called accessory mental foramen (AMF). The AMF may contain accessory nerve fibers originating from branches of the mandibular canal, and this can lead to surgical complications such as failure of local anesthesia, bleeding, neuropathic pain, or paresthesia.5,6 Therefore, the presence and location of the AMF must be accurately determined prior to any intervention, as this is of vital importance in surgical planning.7,8
The prevalence of AMF varies considerably depending on the imaging method used and the population studied; rates ranging from 2% to 30% have been reported in the literature.9,10 Conventional two-dimensional (2D) imaging methods (panoramic and periapical radiography) cannot reflect all of these small structures, whereas high-resolution multidetector computed tomography (MDCT) and cone beam computed tomography (CBCT) enable three-dimensional evaluation and are considered more reliable methods for AMF detection.7,11,12
The AMF is generally located in the postero-inferior region of the MF, although it has been reported that in some individuals it may be superior, medial, or anterior.2,8,13 Furthermore, the diameter of the AMF is usually smaller than that of the MF, and the diameter ratio between the two structures has been reported to be approximately 0.4.2,9 This morphometric diversity highlights both inter-population anatomical differences and the surgical significance of individual variations.
This study aims to evaluate the morphometric and topographic characteristics of the mental and accessory mental foramen using a computed tomography-based analysis method and to provide anatomical references that will contribute to a better understanding of clinical risk areas for the prevention of neurovascular complications in maxillofacial surgery, dental implantology, and anesthesia applications based on the findings obtained.
Materials and Methods
This study was designed as a retrospective descriptive study. A total of 414 maxillofacial computed tomography (CT) images from May 2024 to June 2025 were reviewed from the Department of Radiology’s Picture Archiving and Communication Systems (PACS) archive. All images were obtained using a multi-detector CT scanner (Siemens Somatom Flash, Erlangen, Germany). The scanning parameters were 120 kV, 160 mA, a rotation time of 0.5 s, collimation of 64×0.625 mm, and a field of view (FOV) of 220 mm. A total of 64 patients with mandibular trauma, pathology, missing teeth in the relevant area, a history of surgical intervention, or image artifacts were excluded from the evaluation. The CT images of 350 patients (175 women, 175 men) aged 18-70 years included in the study were examined in three dimensions (3D) using the SyngoVia workstation (Siemens, Germany).
In the obtained 3D images, the heights (short axis), widths (long axis), and distances between the ellipsoid-shaped MF and AMF were measured and recorded (Figure 1). Additionally, the positions of the AMF relative to the MF and teeth were recorded separately (Figure 2). The images were measured twice by an anatomist accompanied by an experienced radiologist, and the average values were recorded.
Ethical ApprovalThis study was approved by the Ethics Committee of Selcuk University Non-Interventional Clinical Research (Date: 29.07.2025, Decision No: 2025/459).
Statistical AnalysisThe data obtained were analyzed using SPSS 25.0 for Windows (IBM, Chicago, IL). The Shapiro-Wilk test results for continuous variables and the skewness and kurtosis values indicated that the data were normally distributed. The comparison of genders was performed using the Independent Samples t-Test, and the comparison of the right and left sides was performed using the Paired Samples t-Test. A p-value <0.05 was considered statistically significant in the tests.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
The mandibles of 350 patients with a mean age of 31.88±11.77 were evaluated bilaterally (700 sides). A total of 16 (2.29%) AMFs were detected in 7 males and 8 females, one of whom had bilateral involvement. The age difference between genders was not significant (p>0.05). The height and width of the MF were significantly larger in males than in females (p<0.05). Due to the insufficient number of AMFs, no comparison could be made, and the descriptive statistical results are presented in Table 1. The height of the MF was 3.27±0.61 mm on the right and 3.22±0.70 mm on the left (p=0.137); the width was 3.16±0.80 mm on the right and 3.18±0.85 mm on the left, and the difference between them was not statistically significant (p=0.764).
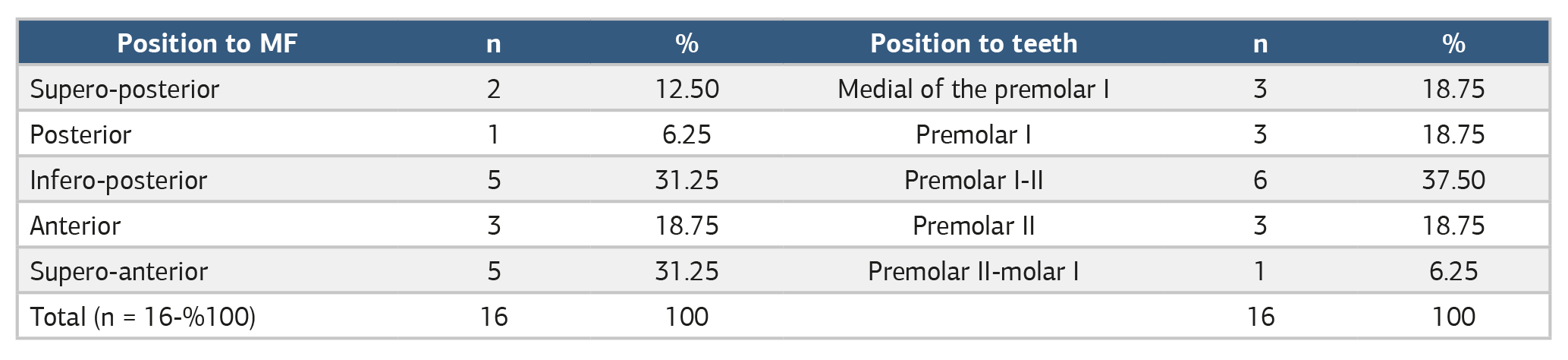
AMFs were located between the first and second premolar teeth, with a maximum of 6, and were positioned at the infero-posterior and supero-anterior aspects of the MF. No AMFs were observed on the first molar tooth and its lateral aspect (Table 2).
Discussion
In our study, the prevalence of AMF was 2.29%, at the lower end of the wide range of 1.8% to 30% reported in the literature across different populations.14 Another example of the lower limit is found in CBCT studies conducted in Brazilian and Korean populations, which reported prevalence rates of 3% and 1.8%, respectively.2,15 Other large-scale studies conducted in the Turkish population using CBCT have mostly reported higher prevalence rates. These studies detected AMF at rates of 11.9%, 12.23%, and 13%.8,9,12 Another study using MDCT detected AMF at a rate of 11%.16 The prevalence in our study is quite low compared with other studies in the Turkish population, which may be due to ethnic differences across population subgroups or variability in imaging/evaluation protocols. Furthermore, bilateral AMF was observed in only one patient (0.29%), and the prevalence of this rare condition has been reported in the literature to range from 0.59% to 3%.2,8
The average diameters of the detected AMFs generally ranged from 0.8 mm to 1.74 mm, consistent with the literature.2,9 In our study, MF height and width were found to be significantly larger in males than in females (p<0.05). This result is consistent with the generally larger mandibular dimensions in males.5,8,17 Many studies in the literature also report that MF measurements are statistically higher in males.8,16 Although the difference between genders is statistically significant, the average difference of 0.3 mm may limit its clinical significance. However, these gender differences can be considered as an additional radiographic method for gender determination in forensic dentistry. Furthermore, the absence of a significant difference in MF height and width between the right and left sides supports the tendency for bilateral symmetry.
The position of the AMF relative to the MF is one of the most critical parameters in surgical planning.14 In our study, AMFs were most commonly found in the postero-inferior (31.25%) and supero-anterior (31.25%) positions. The literature also reports that the most common position of AMF relative to MF is postero-inferior.8,9,16 For example, in the Turkish population, it has been reported that AMFs are most frequently located in the postero-inferior position at 35% and 35.5%.8,9 The AMF detected in the supero-anterior position in our study (31.25%) indicates that these accessory canals should not be overlooked, especially in surgical procedures around the MF, such as implant placement or root-end resection. AMFs in the superior position may increase the risk of injury to neurovascular bundles during flap elevation.14
When examining the location of AMF relative to the teeth, it most frequently occurred between the first and second premolar teeth (37.50%). This finding is consistent with other studies indicating that AMF is frequently located between premolar teeth.2
The average distance between the AMF and MF was measured as 2.39 ± 2.08 mm in this study. This value is close to the reported distance of 2.3 mm and falls within the lower range of wider average distances reported in other studies, such as 3.15 mm and 7.83 mm.2,8,9 The literature reports that this distance varies between 0.64 and 19.55 mm.8
Traditional two-dimensional (2D) radiographs are inadequate for showing anatomical variations of the maxillary sinus due to overlapping and magnification effects. In contrast, CBCT and MDCT enable three-dimensional (3D) and high-resolution evaluation of bone structures in the maxillofacial region, allowing for accurate detection of variations such as AMF.2,3,8,9 The literature reports that reliable results are obtained thanks to the high resolution of MDCT, and some researchers have suggested that it may be superior to CBCT for detecting AMF.17
Limitations
The main limitation of our study examining AMF on the mandible is that we were unable to support our findings with clinical results. A prospective study in which researchers investigate complications associated with the presence of AMF during anesthesia, dental implant placement, and surgery could help overcome this limitation.
Conclusion
Although AMF prevalence is low (2.29%), it has the potential to cause local anesthesia failure or surgical complications (bleeding, paresthesia) due to its function as a branching pathway for related neurovascular structures. The finding that mandibular measurements are significantly larger in males confirms the effect of gender on anatomical morphology. The observation of AMF particularly in the supero-anterior position emphasizes the importance of surgeons carefully evaluating these variations using three-dimensional (3D) imaging methods (MDCT/CBCT) before surgery. These data may contribute to safe surgical planning that reduces the risk of complications in dental implantology and maxillofacial surgery applications, as well as to the standardization of future morphometric studies.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments, or comparable ethical standards.
Informed Consent
Informed consent was waived.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization:H.K., M.İ., Z.F.
Methodology:H.K., M.İ., M.S., Z.F.
Investigation:H.K., M.İ., M.S., H.Ö.
Data Curation:H.K., H.Ö.
Formal Analysis:H.K., M.İ.
Writing–Original Draft:H.K.
Writing–Review & Editing:M.İ., M.S., Z.F., H.Ö.
Supervision:Z.F.
AI Usage Disclosure
No artificial intelligence tools were used in the preparation of this manuscript.
Abbreviations
AMF: Accessory mental foramen
CBCT: Cone-beam computed tomography
CT: Computed tomography
FOV: Field of view
MDCT: Multi-detector computed tomography
MF: Mental foramen
PACS: Picture archiving and communication system
SD: Standard deviation
SPSS: Statistical package for the social sciences
STROBE: Strengthening the reporting of observational studies in epidemiology
References
-
Apinhasmit W, Methathrathip D, Chompoopong S, Sangvichien S. Mental foramen in Thais: an anatomical variation related to gender and side. Surg Radiol Anat. 2006;28(5):529-533. doi:10.1007/s00276-006-0119-7
-
Imada TS, Fernandes LM, Centurion BS, de Oliveira-Santos C, Honório HM, Rubira-Bullen IR. Accessory mental foramina: prevalence, position, and diameter assessed by cone-beam computed tomography and digital panoramic radiographs. Clin Oral Implants Res. 2014;25(2). doi:10.1111/clr.12066
-
Greenstein G, Tarnow D. The mental foramen and nerve: clinical and anatomical factors related to dental implant placement: a literature review. J Periodontol. 2006;77(12):1933-1943. doi:10.1902/jop.2006.060197
-
Thomaidi ZM, Tsatsarelis C, Papadopoulos V. Accessory mental foramina in dry mandibles: an observational study along with systematic review and meta-analysis. Dent J (Basel). 2025;13(3):94. doi:10.3390/dj13030094
-
İnci M, Selcuk M, Kasar H, Yakar H. Digital anatomy of the mental foramen: morphometric evaluation based on multidedector CT imaging. DMT. 2025;1(2):62-67. doi:10.63594/dmte.2025.0011
-
Riesenfeld A. Multiple infraobaital, ethmoidal, and mental foramina in the races of man. Am J Phys Anthropol. 1956;14(1):85-100. doi:10.1002/ajpa.1330140122
-
Angelopoulos C, Thomas S, Hechler S, Parissis N, Hlavacek M. Comparison between digital panoramic radiography and cone-beam computed tomography for the identification of the mandibular canal as part of presurgical dental implant assessment. J Oral Maxillofac Surg. 2008;66(10):2130-2135. doi:10.1016/j.joms.2008.06.021
-
Coban D, Unal Erzurumlu Z, Sadik E, et al. Evaluation of mental foramen and accessory mental foramen using cone beam computed tomography in a Turkish population. BMC Med Imaging. 2025;25(1):140. doi:10.1186/s12880-025-01589-1
-
Aytugar E, Özeren C, Lacin N, Veli I, Çene E. Cone-beam computed tomographic evaluation of accessory mental foramen in a Turkish population. Anat Sci Int. 2019;94(3):257-265. doi:10.1007/s12565-019-00481-7
-
Goyushov S, Tözüm MD, Tözüm TF. Accessory mental/buccal foramina: case report and review of literature. Implant Dent. 2017;26(5):796-801. doi:10.1097/id.0000000000000646
-
Ahmad Y, Alajmy N, Almobiedh K, Alsemari A, Alfailakawi G, Alenezi S. Panoramic assessment of mental foramen location in adult patients in Riyadh, Saudi Arabia: a retrospective cross-sectional study. Cureus. 2024;16(10). doi:10.7759/cureus.72656
-
Kalender A, Orhan K, Aksoy U. Evaluation of the mental foramen and accessory mental foramen in Turkish patients using cone-beam computed tomography images reconstructed from a volumetric rendering program. Clin Anat. 2012;25(5):584-592. doi:10.1002/ca.21277
-
Naitoh M, Hiraiwa Y, Aimiya H, Gotoh K, Ariji E. Accessory mental foramen assessment using cone-beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107(2):289-294. doi:10.1016/j.tripleo.2008.09.010
-
Mostafavi M, Zarch SHH, Eshghpour M, Khodadadzadeh P. Prevalence of accessory mental foramen and lateral lingual foramen using cone beam computed tomography: a single-center cross-sectional study. Oral Maxillofac Surg. 2024;28(4):1623-1633. doi:10.1007/s10006-024-01289-0
-
Han SS, Hwang JJ, Jeong HG. Accessory mental foramina associated with neurovascular bundle in Korean population. Surg Radiol Anat. 2016;38(10):1169-1174. doi:10.1007/s00276-016-1680-3
-
Direk F, Uysal II, Kivrak AS, et al. Mental foramen and lingual vascular canals of mandible on MDCT images: anatomical study and review of the literature. Anat Sci Int. 2018;93(2):244-253. doi:10.1007/s12565-017-0402-1
-
Çelebi A, Gülsün B. Evaluation of accessory mental foramen and accessory infraorbital foramen with cone-beam computed tomography in Turkish population. Aust Endod J. 2023;49(1):13-19. doi:10.1111/aej.12693
Figures
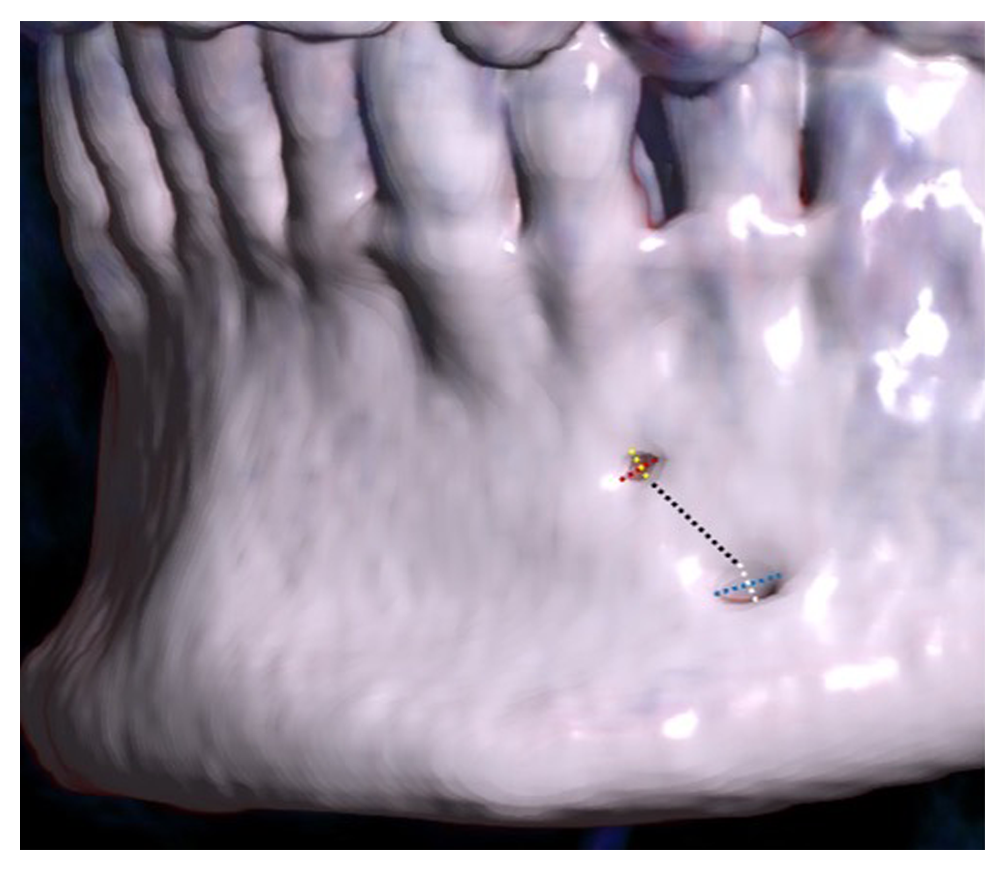
Figure 1. Left lateral view of the mandible. Height (yellow) and width (red) of the accessory mental foramen; Height (white) and width (blue) of the mental foramen; Inter-foraminal distance (black)
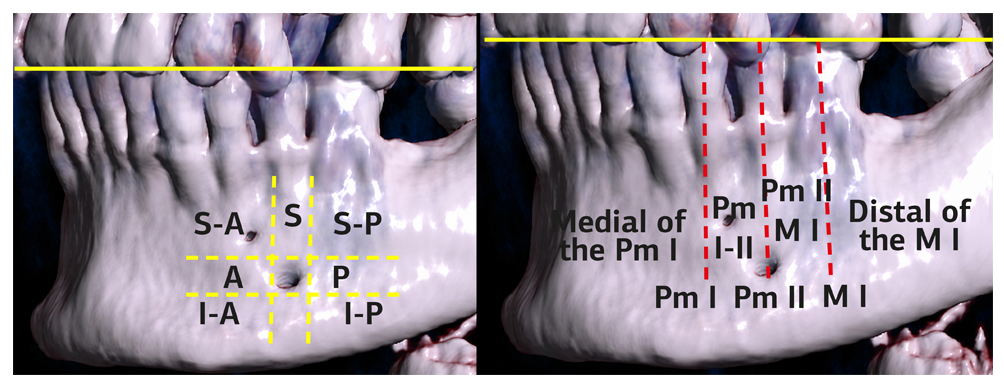
Figure 2. Location of the accessory mental foramen in relation to the mental foramen (left) and teeth (right). Yellow solid line: Occlusal plane. S-A = Supero-anterior; S = Superior; S-P = Supero-posterior; P = Posterior; I-P = Infero-posterior; I = Inferior; I-A = Infero-anterior; A = Anterior; Pm = Premolar; M = Molar
Tables
Table 1. Descriptive statistics results for age, MF, and AMF, and comparison by gender (mm)
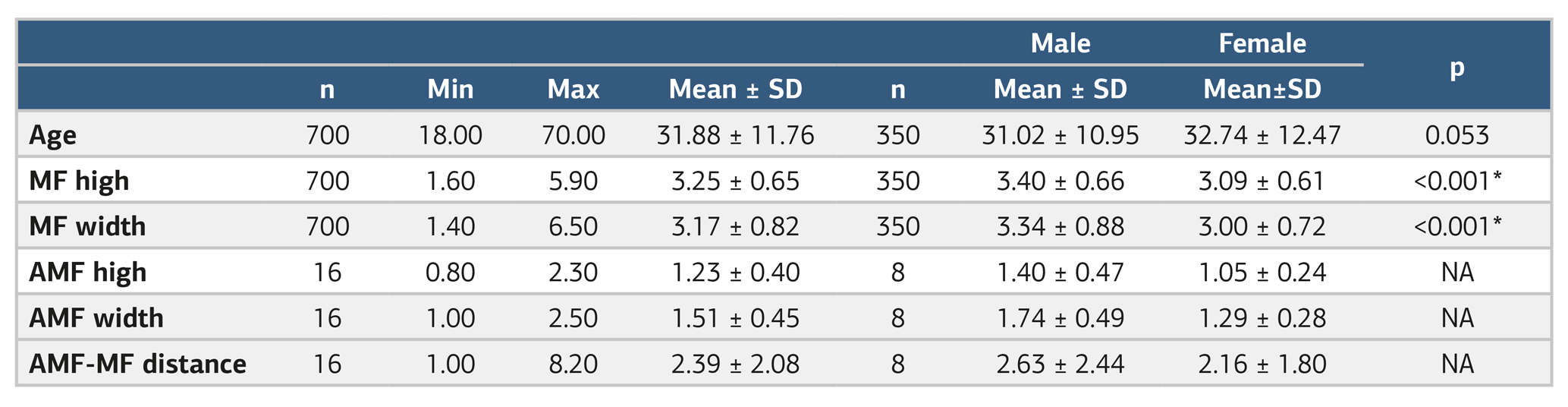
*Statistically significant (p<0.05), Independent Samples t-test; MF: Mental Foramen; AMF: Accessory Mental Foramen; SD: Standart Deviation; NA: Not Applicable
Table 2. The position of the accessory mental foramen relative to the mental foramen and teeth
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Hamza Kasar, Murat İnci, Mehmet Selçuk, Zeliha Fazlıoğulları, Halil Özer. Morphometric analysis, prevalence, and positional relationships of the accessory mental foramen using multi-detector computed tomography. Ann Clin Anal Med 2026;17(7):729-732. doi:10.4328/ACAM.22970
- Received:
- November 1, 2025
- Accepted:
- December 9, 2025
- Published Online:
- December 19, 2025
- Printed:
- July 1, 2026