
How do we close the uterus in a cesarean section? An online survey study
Cesarean closure techniques
Authors
Abstract
AimThe uterine closure technique during cesarean section (CS) significantly affects healing and niche formation; however, there is still no consensus on the optimal method. We aimed to investigate the frequency of techniques used and the factors that affect their use.
MethodsAn anonymous Turkish online survey with 12 questions was sent to available obstetricians in Türkiye. The primary response of interest was the type of uterine closure technique favored in CS. Secondary responses of interest encompassed the formation of a bladder flap, closure of the peritoneum, rectus abdominis muscles, and subcutaneous tissues. The findings were also categorized by years of practice and affiliations.
Results466 physicians filled out the survey. The primary approach utilized was the locked single layer at 75%, whilst the least preferred technique was the locked double layer at 6%. Also, 55.7% of physicians construct a bladder flap, whereas 80.8% routinely close the parietal peritoneum. 86% of surgeons typically suture the subcutaneous tissues when the thickness exceeds 2 cm. No significant difference was found in the frequency of uterine closure techniques between senior specialist physicians and less experienced obstetricians. Also, the most preferred technique was the locked layer in all affiliations.
ConclusionWe showed that the predominant strategy for uterine closure in cesarean sections is the locked single-layer method. Moreover, most doctors seal the parietal peritoneum and stitch the subcutaneous tissue if it is thick.
Keywords
Introduction
Caesarean section (CS) is the most common operation among women, and the rate has risen substantially around the world in the last two decades.1 This growing CS incidence has sparked attention to the possible short and long-term morbidity of cesarean scars. In almost 50% of women with a history of cesarean section, a uterine scar defect, referred to as a “niche”, characterized by disruption of the myometrium at the cesarean scar, can be observed.2 Uterine scar defects detected on ultrasound several weeks or months after CS are associated with numerous gynecologic complications such as prolonged menstrual bleeding, intermenstrual spotting, and subfertility.3 In addition to these gynecologic concerns, complications in subsequent pregnancies related to a niche were also reported, such as uterine rupture and placenta accreta spectrum (PAS) disorders.4 At present, these obstetric complications are among the most important causes of maternal morbidity and mortality, and they cause a severe social and economic burden. The exact mechanism for niche development remains unknown. Nonetheless, several studies have identified various prognostic risk factors for incomplete scar healing, including patient, labor, and surgery-related factors.5 The impact of uterine closure technique on uterine scar stability and the risk of niche development has become a focus of recent studies.6 Studies comparing the impact of suture techniques on scar stability yield inconsistent results. Some studies conclude that double-layer closure results in a thicker uterine scar, while others have found no significant difference between surgical techniques. Unfortunately, it is difficult to reach a definitive conclusion on this issue, and many international and national organizations fail to provide clear and explicit recommendations.
CS rates are increasing rapidly in our country, as they are worldwide. In 2017, Türkiye had a CS rate of 53.1%, nearly double the OECD average, and was the highest-ranked OECD country.7 Regrettably, our nation ranks among the top five countries globally with the highest rates of CS, which remains a significant public health issue.8 Although thousands of CS procedures are performed each day across our country, clinicians’ surgical techniques differ significantly. There is no data on maternal complications or the long-term effects of these variations in surgical technique.
In this survey study, we aimed to determine the frequency of uterine closure techniques and the most commonly used methods by obstetricians and gynecologists during CS in our country, as well as other steps in the CS procedure.
Materials and Methods
An online survey was conducted among members of the Turkish Gynecology and Obstetrics Association (TJOD). Survey questions were distributed to all participants via their social media accounts. The survey lasted two months. Four weeks after the initial contact, all participants received an updated email reminder. Consent to publish data was obtained from all respondents, and all responses were anonymous.
A 12-question survey in Turkish was created, and all questions were multiple-choice. Physicians contacted via social media were emailed a survey link. The initial six questions assessed participants' demographic and professional attributes, including age, gender, place of employment, years of medical practice, and the number of CS procedures performed annually. Question 7 was the pivotal inquiry of the study, inquiring about obstetricians’ preferred methods for closing the uterus during CS. Participants were given four options, including;’’ locked single-layer, unlocked single-layer, locked double-layer, and unlocked double-layer, “ and instructed to select one. The remaining five questions examined surgical preferences across different phases of the CS and required a ‘yes’ or ‘no’ response.
All data analyses were performed using SPSS (Statistical Packages for the Social Sciences) software, version 22.0 (SPSS Inc., Chicago, USA). Numbers and percentages were used as descriptive statistics to analyze the data. Additionally, the participants were categorized into two groups based on their professional expertise, and an analysis was conducted to determine differences in uterine closure procedures between the groups. A second analysis was also utilized based on affiliations. Categorical values were analyzed by the chi-square test. A p-value <0.05 was considered statistically significant.
Ethical ApprovalThis study was approved by the Ethics Committee of Lokman Hekim University, Faculty of Medicine (Date: 01.05.2025, Decision No: 2025/184).
Statistical AnalysisStatistical analyses were performed using IBM SPSS Statistics version 22.0 (IBM Corp., Armonk, NY, USA). Categorical variables were presented as number (n) and percentage (%). Comparisons between groups were performed using the chi-square test. A two-sided p-value <0.05 was considered statistically significant.
Reporting GuidelinesThe study was reported in accordance with STROBE guideline.
Results
A total of 795 physicians downloaded the survey, and 466 obstetricians responded to the survey questions. The response rate was calculated as 58.6%. The predominant age group among participants was 35-45 years, comprising 43.3% of the overall population, and only % 2.7% of physicians were older than 65. When categorized by career stage, 20.1% of physicians had practiced as obstetricians for less than 5 years, while 25.3% had practiced for over 20 years. Over fifty percent of the physicians held the position of specialist, 10.7% were designated as associate professors, and 12.1% were classified as professors. Additionally, 52% of the participants were female, whereas 48% were male. As categorized by their respective hospitals, 15% of physicians were employed in public hospitals, 24.2% in educational and research hospitals, 18.1% in university hospitals, 24.6% in private hospitals, and 18.1% in private clinics. Furthermore, when analyzing the number of CS performed by participants in a year, 24.6% reported fewer than 50 CS annually, while 16.2% reported more than 300 CS annually. Demographic features and characteristics of physicians were summarized in Table 1.
Analysis of the replies to the major query of our survey about incision closure procedures in CS revealed that the predominant method adopted was the locked single layer at 75%, whilst the least favored technique was the locked double layer at 6%. Besides, 8% of physicians preferred unlocked single-layer and 11% unlocked double-layer techniques. Figure 1 illustrates participants’ preferences regarding hysterotomy closure methods.
The last five questions of our poll concerned other surgical procedures involved in CS surgery. After analyzing the responses, we found that 55.7% of physicians create a bladder flap and 80.8% routinely close the parietal peritoneum in CS. Also, most surgeons routinely prefer to suture the subcutaneous tissues if the thickness is >2 cm. Closing the visceral peritoneum and approximating the rectus abdominis muscles are less commonly favored methods. Questions and answers regarding preferred alternative techniques for CS in physicians are shown in Table 2.
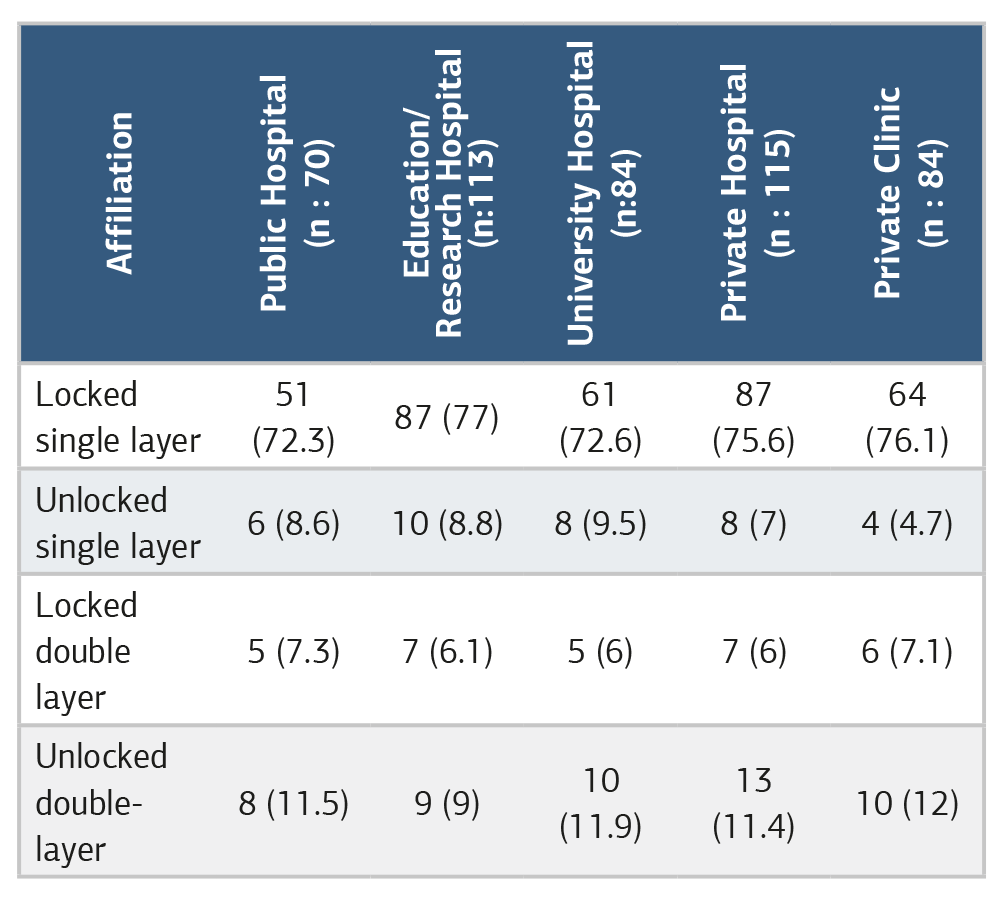
Eventually, physicians were categorized into two groups based on their professional experience: those with less than 10 years and those with more than 10 years. The <10-year group consisted of 186 (40%) physicians, while the >10-year group comprised 280 (60%) physicians. Analysis of preferences for uterine closure procedures during cesarean section revealed no significant differences between the two groups for any technique. The locked single-layer was the most favored strategy among both senior and younger physicians. The distribution of uterine closure procedures, stratified by physicians’ years of expertise, is illustrated in Table 3. Moreover, when the techniques were assessed by the institutions where the physicians worked, the locked-single-layer method was the most popular, with rates of 70% or higher at each institution. Distribution of uterine closure procedures stratified by physicians’ affiliations is shown in Table 4.
Discussion
This survey study demonstrates that the predominant uterine closure technique among Turkish obstetricians is the locked- single-layer approach, utilized by 75% of respondents. Less than 20% of physicians prefer the double-layer closure technique. Moreover, we found no significant difference between those who had been in the profession for more than 10 years and those who had been in it for the first 10 years. Also, in all institutions, more than 70% of physicians preferred the locked single-layer method.
In our survey, we also inquired about other aspects of the CS operation. We demonstrated that most physicians do not close the visceral peritoneum or approximate the rectus abdominis muscles. In contrast, the majority of physicians favor closing the parietal peritoneum and suturing the subcutaneous tissues if the subcutaneous tissue is thick.
Over the past three decades, the prevalence of CS has been steadily rising worldwide. The average CS rate across OECD countries is approximately 29%, but significant differences exist among nations, as indicated by 2022 data. While CS rates are below 20% in Israel and Scandinavian countries, they exceed 50% in Türkiye, Korea, and Chile. Sadly, Türkiye is the OECD country with the highest CS rate, approaching 60%, highlighting a serious public health concern.9 PAS rates have increased over the past two decades, especially in high-income countries, primarily due to rising CS rates.10 PAS is a significant contributor to maternal morbidity and death, resulting in severe psychological, social, and economic issues. Although the precise cause of PAS remains unclear, insufficient healing of the hysterotomy incision after a prior CS seems to be a primary contributing factor.11 This finding has prompted several experts to investigate the optimal method for closing the hysterotomy during CS to facilitate recovery and minimize the risk of PAS.
In recent years, alongside the rising incidence of CS and PAS, the optimal technique for uterine closure has emerged as a significant concern. Roberge et al. examined 20 randomized clinical trials (RCTs) and identified no statistically significant difference in cesarean scar defect and uterine dehiscence. They also determined that single-layer uterine closure was associated with a substantially reduced residual myometrial thickness.12 Sardo et al. Evaluated 9 RCTs and 3969 CS and showed that single or double-layer closure of the uterine incision is associated with a similar incidence of niche formation, as well as uterine dehiscence and uterine rupture in a subsequent pregnancy. But they also indicated that, compared with single-layer closure, double-layer closure was associated with a significantly greater residual myometrial thickness on ultrasound, which is of unclear clinical significance.13 Finally, Verberkt et al. conducted a 2-center multicenter RCT to address the optimal uterine closure technique and allocated 2292 women. They found no superiority of double-layer uterine closure after a first CS in terms of reproductive or obstetrical outcomes at the 3-year follow-up. In addition, they conclude that in both single-layer and double-layer closure groups, gynecologic symptoms, including spotting, dysmenorrhea, and mild sexual dysfunction after CS, are highly prevalent.14 Due to a lack of clear, sufficient data, there is currently no universally accepted evidence-based guideline regarding the technique for uterine closure in CS.15
Although CS is the most commonly performed operation on women worldwide, significant technical discrepancies can be seen even among physicians working in the same clinic due to the lack of sufficient evidence regarding the method used to close the hysterotomy. Demers et al. conducted an anonymous survey of all active members of the Association des Obstetriciens-Gynecologues du Quebec and found that the double-layer continuous suture was the most popular technique, reported by 89% of respondents. Furthermore, they suggested that the use of double-layer uterine closure has increased dramatically over the last two decades. Researchers attribute this increase to the growth in vaginally birth after cesarean delivery rates during the last 20 years.16 Kaps et al. performed an online survey of 648 obstetric hospitals in Germany. They found that 75% of participants preferred to close the uterus using the unlocked single-layer method, and fewer than 10% of obstetricians favored double-layer techniques.17 In our country, in contrast to Canada and Germany, the most utilized technique was the locked single-layer technique.
We believe that the primary reasons for the widespread preference for this technique in our country are that single-layer suturing reduces operative duration, and that sealing improves hemostasis. Furthermore, in many educational clinics across our nation, the locked-single-layer approach is taught throughout residency training and becomes habitual.
Limitations
There are numerous weaknesses and limitations in our publication. First of all, despite our best efforts to reach all obstetricians in our country, we were only able to distribute the survey to 795 physicians. Unfortunately, the response rate was as low as 58.6%. Secondly, we do not know whether the practices of those participants reflect the practices of all obstetricians throughout Türkiye. Nevertheless, our survey trial is the first national questionnaire on uterine closure techniques. It demonstrates the feasibility of conducting national online surveys on obstetric topics and facilitates discussion of the need to establish a standardized uterine closure technique during CS.
Conclusion
In this nationwide online survey, we demonstrated that the most common technique for uterine closure in CS is the locked single-layer method. Furthermore, the majority of clinicians close the parietal peritoneum and suture subcutaneous tissue if it is thick. Additionally, no difference was found between senior and less-experienced physicians in uterine closure methods. Given that our nation ranks among the top globally in CS rates, it is evident that more efforts are needed to identify the optimal uterine closure technique and promote it uniformly across the country.
Declarations
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Electronic informed consent was obtained from all participants before survey completion.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: G.T., H.Ç.
Methodology: G.T., M.C., H.E.
Investigation: G.T., M.C., O.K.
Data Curation: M.C., O.K.
Formal Analysis: G.T.
Writing – Original Draft: G.T.
Writing – Review & Editing: M.C., H.E., O.K., H.Ç.
Supervision: H.E., H.Ç.
AI Usage Disclosure
No artificial intelligence tools were used in the preparation of this manuscript.
Abbreviations
CS:Cesarean section
OECD: Organization for economic co-operation and development
PAS:Placenta accreta spectrum
RCT:Randomized controlled trial
SPSS:Statistical package for the social sciences
TJOD:Turkish gynaecology and obstetrics association
References
-
Betran AP, Ye J, Moller AB, Souza JP, Zhang J. Trends and projections of caesarean section rates: global and regional estimates. BMJ Glob Health. 2021;6(6). doi:10.1136/bmjgh-2021-005671
-
Lin PL, Hou JH, Chen CH. A common problem between gynecology, obstetrics, and reproductive medicine: cesarean section scar defect. Taiwan J Obstet Gynecol. 2024;63(4):459-470. doi:10.1016/j.tjog.2024.03.018
-
Tower AM, Frishman GN. Cesarean scar defects: an underrecognized cause of abnormal uterine bleeding and other gynecologic complications. J Minim Invasive Gynecol. 2013;20(5):562-572. doi:10.1016/j.jmig.2013.03.008
-
Premkumar A, Huysman B, Cheng C, Einerson BD, Moayedi G. Placenta accreta spectrum in the second trimester: a clinical conundrum in procedural abortion care. Am J Obstet Gynecol. 2025;232(1):92-101. doi:10.1016/j.ajog.2024.07.045
-
Verberkt C, Lemmers M, de Vries R, Stegwee SI, de Leeuw RA, Huirne JAF. Aetiology, risk factors, and preventive strategies for niche development: a review. Best Pract Res Clin Obstet Gynaecol. 2023;90:102363. doi:10.1016/j.bpobgyn.2023.102363
-
Mohr-Sasson A, Castel E, Cohen A, et al. The association of endometrial closure during cesarean section to the risk of developing uterine scar defect: a randomized control trial. Arch Gynecol Obstet. 2024;309(5):2063-2070. doi:10.1007/s00404-024-07417-1
-
Amyx M, Philibert M, Farr A, et al. Trends in caesarean section rates in Europe from 2015 to 2019 using Robson’s ten-group classification system: a Euro-Peristat study. BJOG. 2024;131(4):444-454. doi:10.1111/1471-0528.17670
-
Boerma T, Ronsmans C, Melesse DY, et al. Global epidemiology of use of and disparities in caesarean sections. Lancet. 2018;392(10155):1341-1348. doi:10.1016/s0140-6736(18)31928-7
-
Liu B, Abdi MA, Ma Y. Trend of cesarean section rates and related factors among first-time mothers with single pregnancies in Zhejiang Province, China: evidences from a multicentre study. Int J Womens Health. 2025;17:1681-1692. doi:10.2147/ijwh.s497765
-
Jauniaux E, Jurkovic D, Hussein AM, Burton GJ. New insights into the etiopathology of placenta accreta spectrum. Am J Obstet Gynecol. 2022;227(3):384-391. doi:10.1016/j.ajog.2022.02.038
-
Jauniaux E, Collins S, Burton GJ. Placenta accreta spectrum: pathophysiology and evidence-based anatomy for prenatal ultrasound imaging. Am J Obstet Gynecol. 2018;218(1):75-87. doi:10.1016/j.ajog.2017.05.067
-
Roberge S, Demers S, Berghella V, Chaillet N, Moore L, Bujold E. Impact of single- vs double-layer closure on adverse outcomes and uterine scar defect: a systematic review and metaanalysis. Am J Obstet Gynecol. 2014;211(5):453-460. doi:10.1016/j.ajog.2014.06.014
-
Di Spiezio Sardo A, Saccone G, McCurdy R, Bujold E, Bifulco G, Berghella V. Risk of cesarean scar defect following single- vs double-layer uterine closure: systematic review and meta-analysis of randomized controlled trials. Ultrasound Obstet Gynecol. 2017;50(5):578-583. doi:10.1002/uog.17401
-
Verberkt C, Geomini PMAJ, Van Eekelen R, et al. Single-layer vs double-layer uterine closure during cesarean delivery: 3-year follow-up of a randomized controlled trial (2Close study). Am J Obstet Gynecol. 2024;231(3):346.e1-346.e11. doi:10.1016/j.ajog.2023.12.032
-
Caughey AB, Nelson G, Wilson RD, et al. Guidelines for intraoperative care in cesarean delivery: enhanced recovery after surgery society recommendations, part 2. Am J Obstet Gynecol. 2018;219(6):533-544. doi:10.1016/j.ajog.2018.08.006
-
Demers S, Roberge S, Afiuni YA, Chaillet N, Girard I, Bujold E. Survey on uterine closure and other techniques for caesarean section among Quebec’s obstetrician-gynaecologists. J Obstet Gynaecol Can. 2013;35(4):329-333. doi:10.1016/s1701-2163(15)30960-9
-
Kaps C, Schwickert A, Dimitrova D, et al. Online survey on uterotomy closure techniques in caesarean section. J Perinat Med. 2021;49(7):809-817. doi:10.1515/jpm-2021-0118
Figures
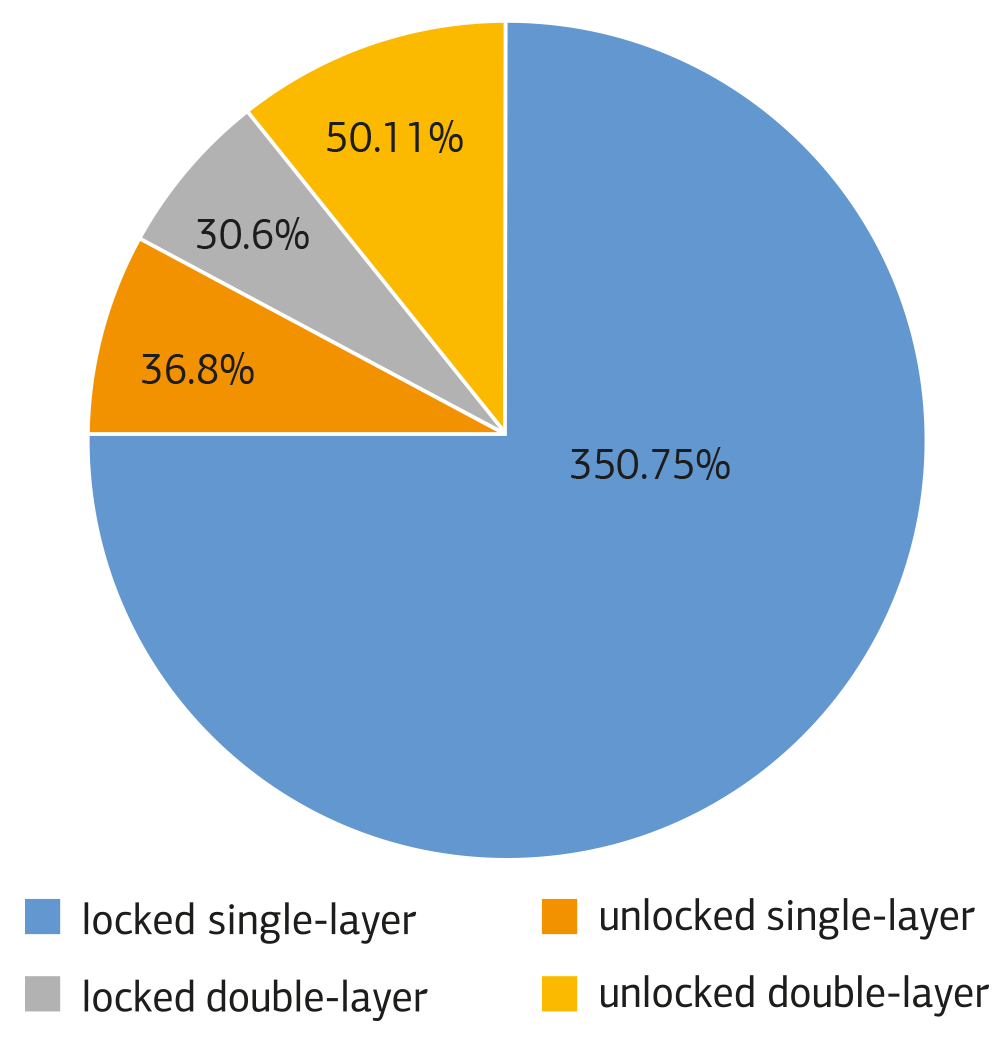
Figure 1. Distribution of the procedure used for closing the uterus during a cesarean operation (n: 466)
Tables
Table 1. Demographic features and characteristics of physicians (n: 466, (%))
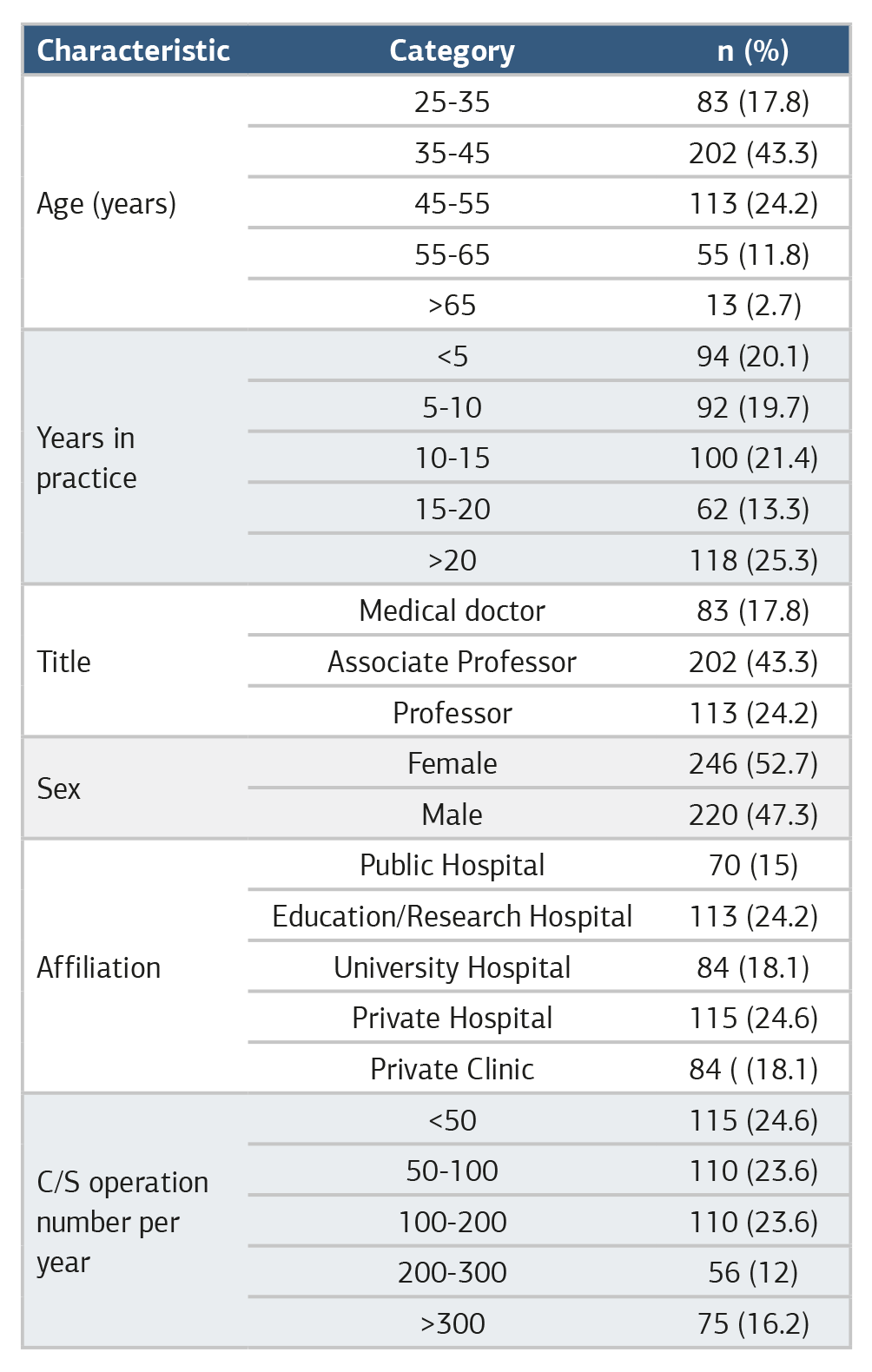
Table 2. Questions and answers regarding preferred techniques for caesarean section in physicians (n:466 (%))

Table 3. Distribution of uterine closure procedures stratified by physicians’ years of expertise

Table 4. Distribution of uterine closure procedures stratified by physicians’ affiliations (%)
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Gürcan Türkyılmaz, Meryem Ceyhan, Hakan Erenel, Onur Karaaslan, Hatice Çelik. How do we close the uterus in a cesarean section? An online survey study. Ann Clin Anal Med 2026;17(7):709-713. doi:10.4328/ACAM.22978
- Received:
- November 7, 2025
- Accepted:
- December 22, 2025
- Published Online:
- January 9, 2026
- Printed:
- June 1, 2026