
Comparison of early and mid-term recanalization in deep venous thrombosis treated with rivaroxaban versus heparin–warfarin: a five-year retrospective study
Rivaroxaban vs warfarin in acute DVT
Authors
Abstract
Aim Early venous recanalization after acute deep vein thrombosis (DVT) is clinically important, as delayed thrombus resolution is associated with residual venous obstruction and post-thrombotic syndrome. This study aimed to compare early and mid-term venous recanalization outcomes in patients with acute lower-extremity DVT treated with rivaroxaban or conventional heparin followed by warfarin therapy.
Methods This retrospective multicenter cohort study included 150 consecutive patients diagnosed with acute lower-extremity DVT between September 2018 and September 2023. After exclusion of 20 patients due to insufficient imaging follow-up, 130 patients were analyzed (heparin–warfarin, n = 60; rivaroxaban, n = 70). Treatment selection was based on clinician judgment and patient characteristics. Venous recanalization was assessed using serial color Doppler ultrasonography at baseline and approximately 30, 90, and 180 days. Primary outcomes were the degree of venous recanalization and time to first recanalization; secondary outcomes included recurrent DVT and major bleeding. Kaplan–Meier analysis was used for time-to-event outcomes.
Results Rivaroxaban was associated with significantly higher recanalization rates at 30 days (57.1% vs 18.3%, p < 0.001), 90 days (82.8% vs 53.3%, p < 0.001), and 180 days (94.2% vs 81.6%, p = 0.02). Complete recanalization at 180 days was more frequent with rivaroxaban (78.5% vs 63.3%, p = 0.04). Median time to first recanalization was shorter with rivaroxaban (41 vs 76 days, p < 0.001).
Conclusion In this real-world cohort, rivaroxaban achieved faster and more complete venous recanalization than heparin–warfarin therapy without increased adverse events, supporting its use as a first-line treatment for acute DVT.
Keywords
Introduction
Deep vein thrombosis (DVT) is a key component of venous thromboembolism and remains a substantial cause of both short- and long-term morbidity worldwide.1 Despite significant advances in treatment strategies, many patients continue to experience complications related to residual venous obstruction or recurrent thrombosis, ultimately leading to post-thrombotic syndrome (PTS), which negatively affects quality of life and functional capacity.2 Accumulating evidence indicates that both the timing and extent of venous recanalization following the initial thrombotic event play a critical role in determining long-term venous outcomes.3 For many years, conventional anticoagulation with parenteral heparin followed by vitamin K antagonists (VKAs) has been the cornerstone of acute DVT management.4 However, warfarin therapy is limited by its narrow therapeutic window, requirement for frequent laboratory monitoring, food–drug interactions, and interindividual variability in anticoagulant response.4 These limitations frequently result in subtherapeutic anticoagulation, which has been associated with delayed thrombus resolution and increased rates of residual venous obstruction on follow-up imaging studies.3 Direct oral anticoagulants (DOACs) have emerged as effective alternatives to conventional therapy in the management of acute DVT.4,5 Among DOACs, rivaroxaban offers predictable pharmacokinetics, rapid onset of action, and fixed dosing without the need for routine coagulation monitoring.14 Consequently, current international guidelines recommend DOACs as first-line therapy for most patients with acute DVT in the absence of contraindications.2,4,5 Beyond their established efficacy in preventing recurrent venous thromboembolism, increasing attention has focused on the potential of DOACs to promote improved venous recanalization.6,7 Recent observational studies and comparative analyses suggest that DOAC-based regimens may be associated with more rapid thrombus regression and lower rates of residual thrombosis compared with warfarin therapy.6,8 Improved venous recanalization has also been correlated with a reduced incidence of PTS, underscoring its clinical relevance in contemporary DVT management.3,7,9 Nevertheless, available evidence remains heterogeneous, particularly with respect to time-dependent analyses of recanalization outcomes. Color Doppler ultrasonography is a widely accepted noninvasive modality for evaluating thrombus burden, venous patency, and recanalization during follow-up in patients with acute DVT.3,10 In addition, time-to-event analyses, such as Kaplan–Meier estimation of time to first successful recanalization, provide complementary insight into thrombus resolution kinetics that cannot be fully captured by fixed follow-up assessments alone.11 Within this context, the present study aims to compare early and mid-term venous recanalization outcomes in patients with acute lower-extremity DVT treated with rivaroxaban versus conventional heparin–warfarin therapy using serial color Doppler ultrasonography.
Materials and Methods
Study Design and PopulationThis retrospective, multicenter cohort study included 150 consecutive consenting adult patients with objectively confirmed acute lower-extremity deep vein thrombosis (DVT) who were treated at tertiary cardiovascular centers between September 2018 and September 2023. The study was conducted in accordance with the principles of the Declaration of Helsinki, and the study protocol was approved by the institutional ethics committee. Among the initial cohort of 150 patients with ultrasound-confirmed acute lower-extremity DVT, 20 patients were excluded due to the absence of follow-up imaging or incomplete ultrasonographic evaluations. Consequently, the final study population consisted of 130 patients.
Inclusion and Exclusion CriteriaEligible patients were adults (≥ 18 years) with symptomatic, objectively documented acute lower-extremity DVT, with symptom onset occurring within 14 days prior to diagnosis. Inclusion further required the availability of at least three follow-up color Doppler ultrasonographic examinations after initiation of anticoagulation therapy. Exclusion criteria included pregnancy; severe renal impairment (estimated glomerular filtration rate < 30 mL / min / 1.73 m²); intra-abdominal thrombophlebitis; advanced hepatic disease; active malignancy requiring alternative anticoagulation strategies; known thrombophilia necessitating non-standard anticoagulation approaches; and a history of major bleeding.
Treatment StrategyPatients received either rivaroxaban monotherapy or conventional anticoagulation consisting of initial parenteral heparin followed by warfarin therapy. Treatment allocation was not randomized and was based on physician judgment and patient-specific factors, including renal and hepatic function, bleeding risk, potential drug–drug interactions, anticipated compliance, feasibility of laboratory monitoring, and patient preference. In patients treated with warfarin, dose adjustments were guided by international normalized ratio (INR) measurements in accordance with institutional protocols. Due to the retrospective design and limitations of available INR data, calculation of time in therapeutic range (TTR) was not feasible.
Ultrasonography Protocol and DefinitionsBaseline and follow-up color Doppler ultrasonography (CDU) assessments were performed by experienced vascular sonographers in accordance with standardized imaging protocols. The evaluated venous segments included the common and external iliac, common femoral, femoral, deep femoral, popliteal, anterior tibial, posterior tibial, and peroneal veins. Venous recanalization was categorized as complete, partial, or absent, based on ultrasonographic findings of full venous compressibility with normal flow, the presence of residual non-occlusive thrombus, or persistent venous occlusion, respectively. The number of involved venous segments was recorded at baseline and during follow-up.
Follow-up and Outcome MeasuresFollow-up CDU examinations were scheduled approximately 30, 90, and 180 days after initiation of anticoagulant therapy. The primary outcomes were the extent of venous recanalization at each follow-up time point and the time to first documented venous recanalization. Secondary outcomes included recurrent DVT and major bleeding events, defined according to the criteria of the International Society on Thrombosis and Hemostasis.
Ethical ApprovalThe study was approved by the Ethics Committee of Ordu University Research and Education Hospital (Date: 2021-04-29, No: 113).
Statistical AnalysisContinuous variables are presented as mean ± standard deviation or median with interquartile range, as appropriate, while categorical variables are expressed as frequencies and percentages. Between-group comparisons were performed using Student’s t-test or the Mann–Whitney U test for continuous variables, and the chi-square test or Fisher’s exact test for categorical variables. Time-to-event analyses for first venous recanalization were conducted using Kaplan–Meier survival estimates, with intergroup comparisons assessed using the log-rank test. Owing to the retrospective design and limited sample size, multivariable adjustment for potential confounders such as age, provocation status, or DVT localization was not performed. All statistical analyses were conducted using standard statistical software, and a two-tailed p-value < 0.05 was considered statistically significant.
Reporting GuidelinesThis retrospective, multicenter cohort study is reported in accordance with the STROBE statement.
Results
Baseline CharacteristicsA total of 130 patients with acute lower-extremity DVT were included in the final analysis. Sixty patients received heparin followed by warfarin, whereas 70 patients were treated with rivaroxaban. There were no significant differences between the two groups with respect to age, sex distribution, body mass index, cardiovascular risk factors, or smoking status. In addition, the proportions of patients with provoked DVT, proximal versus distal thrombus involvement, and baseline thrombus extent expressed as the number of affected venous segments were comparable between groups. No statistically significant differences were observed in these baseline characteristics (Table 1).
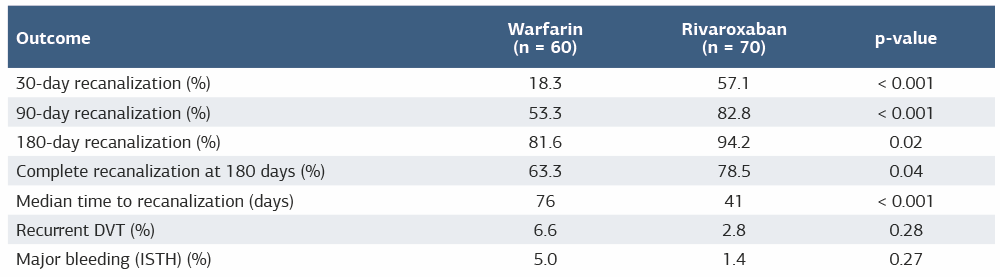
Venous Recanalization OutcomesPatients treated with rivaroxaban demonstrated significantly higher venous recanalization rates during early follow-up. At 30 days, venous recanalization occurred in 57.1% of patients in the rivaroxaban group compared with 18.3% in the heparin–warfarin group (p < 0.001). This difference remained significant at 90 days, with recanalization rates of 82.8% and 53.3% in the rivaroxaban and heparin–warfarin groups, respectively (p < 0.001). At 180 days, the overall venous recanalization rate continued to be significantly higher in the rivaroxaban group (94.2% vs 81.6%, p = 0.02) (Table 2). Complete venous recanalization at the end of follow-up was achieved more frequently in patients receiving rivaroxaban than in those receiving heparin–warfarin therapy (78.5% vs 63.3%, p = 0.04), whereas the rate of partial recanalization was similar between the two treatment groups. Residual venous obstruction at 180 days was less frequent in the rivaroxaban group.
Time to First RecanalizationKaplan–Meier analysis demonstrated a significantly shorter time to first documented venous recanalization in patients treated with rivaroxaban compared with those receiving heparin–warfarin therapy. The median time to first recanalization was 41 days in the rivaroxaban group and 76 days in the heparin–warfarin group (log-rank p < 0.001). Separation between the recanalization curves was evident early during follow-up and persisted throughout the observation period (Figure 1).
Secondary OutcomesRecurrent DVT occurred in 2 patients (2.8%) in the rivaroxaban group and 4 patients (6.6%) in the heparin–warfarin group; this difference was not statistically significant (p = 0.28). Major bleeding events were infrequent and did not differ significantly between treatment groups, occurring in 1 patient (1.4%) receiving rivaroxaban and 3 patients (5.0%) receiving heparin–warfarin therapy (p = 0.27). No fatal bleeding events were observed.
Discussion
In this retrospective cohort analysis of patients with acute lower-extremity deep vein thrombosis, treatment with rivaroxaban was associated with more rapid and more extensive venous recanalization compared with the conventional heparin–warfarin regimen. Differences between treatment strategies became evident as early as day 30 and persisted throughout the mid-term follow-up at days 90 and 180. Consistent with these findings, time-to-event analysis demonstrated a significantly shorter median time to first documented venous recanalization in patients treated with rivaroxaban. Early and successful venous recanalization is increasingly recognized as an important prognostic factor for long-term venous outcomes following acute DVT.3,12 Residual venous obstruction has been associated with an increased risk of post-thrombotic syndrome and impaired quality of life.3,9 Although post-thrombotic syndrome was not systematically evaluated in the present study, the higher rates of early and complete recanalization observed in the rivaroxaban group may have clinically relevant implications for long-term venous function and symptom burden. A potential explanation for the observed intergroup differences may lie in the pharmacological and practical characteristics of the anticoagulant regimens used. Warfarin therapy is limited by a narrow therapeutic index and substantial interindividual variability, frequently resulting in subtherapeutic anticoagulation levels.4 In contrast, rivaroxaban is characterized by predictable anticoagulant effects, rapid onset of action, and fixed dosing, which may allow more stable inhibition of thrombin generation during the early phase of thrombus organization and remodeling.13 The present findings are consistent with previous observational studies demonstrating more favorable venous recanalization outcomes with DOACs compared with vitamin K antagonists.6,7,12 Several limitations should be acknowledged, including the retrospective design, absence of adjustment for confounders, and lack of long-term PTS assessment. Despite these limitations, the present study provides real-world evidence supporting faster venous recanalization with rivaroxaban, consistent with contemporary guideline recommendations.5,2,6 From a clinical perspective, the present findings may have practical implications for the contemporary management of acute lower-extremity DVT. Current international guidelines recommend direct oral anticoagulants as first-line therapy for most patients, primarily based on their efficacy in preventing recurrent venous thromboembolism and their favorable safety profile compared with vitamin K antagonists.2,3,4 The observed earlier and more frequent venous recanalization associated with rivaroxaban in this study suggests a potential additional benefit beyond thromboembolic prevention, particularly during the early phase of thrombus resolution. Although causality cannot be inferred from this retrospective analysis, faster recanalization may contribute to improved venous patency and reduced residual venous obstruction, which have been linked to adverse long-term outcomes, including post-thrombotic syndrome.3,9,12 These findings support the preferential use of rivaroxaban in appropriately selected patients, especially in clinical scenarios where early thrombus resolution and preservation of venous function are considered important therapeutic goals.
Limitations
This study is limited by its retrospective, non-randomized design, which may have introduced selection bias and residual confounding. Time in therapeutic range could not be reliably assessed in patients treated with warfarin because of incomplete longitudinal INR data. In addition, multivariable-adjusted analyses were not performed, and long-term clinical outcomes were not systematically evaluated.
Conclusion
In patients with acute lower-extremity deep vein thrombosis, rivaroxaban was associated with earlier and more complete venous recanalization compared with heparin–warfarin therapy, while rates of recurrent thrombosis and major bleeding were comparable between treatment groups. These findings indicate that rivaroxaban is an effective and safe therapeutic option and may offer advantages in thrombus resolution. Nevertheless, prospective studies with larger cohorts and longer follow-up are warranted to clarify the clinical implications of accelerated venous recanalization.
Declarations
Ethics Declarations
Ethics approval for this study was obtained from the Ordu University Research and Education Hospital Ethics Committee (Date: 29 April 2021; No: 113).
Animal and Human Rights Statement
All procedures performed in this study were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent for participation in this study was obtained from all participants.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy considerations but are available from the corresponding author upon reasonable request.
Conflict of Interest
The author declares no conflicts of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: E.K.
Methodology: E.K.
Investigation: E.K.
Data curation: E.K.
Formal analysis: E.K.
Writing – original draft: E.K.
Writing – review & editing: E.K.
Supervision: E.K.
Scientific Responsibility Statement
The author declares responsibility for the scientific content of the manuscript, including study design, data collection, analysis and interpretation, manuscript preparation, critical revision, and approval of the final version.
Abbreviations
CDU: Color Doppler Ultrasonography
DOAC: Direct Oral Anticoagulant
DVT: Deep Vein Thrombosis
eGFR: Estimated Glomerular Filtration Rate
INR: International Normalized Ratio
ISTH: International Society on Thrombosis and Hemostasis
PTS: Post-Thrombotic Syndrome
TTR: Time in Therapeutic Range
VKA: Vitamin K Antagonist
VTE: Venous Thromboembolis
References
-
Ortel TL, Neumann I, Ageno W, et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism. Blood Adv. 2020;4(19):4693-4738. doi:10.1182/bloodadvances.2020001830
-
Twine CP, Kakkos SK, Aboyans V, et al. ESVS 2023 clinical practice guidelines on antithrombotic therapy for vascular diseases. Eur J Vasc Endovasc Surg. 2023;65(5):627-689. doi:10.1016/j.ejvs.2023.03.042
-
Prandoni P, Lensing AWA, Prins MH, et al. Residual vein thrombosis as a predictive factor of recurrent venous thromboembolism. Ann Intern Med. 2002;137(12):955-960. doi:10.7326/0003-4819-137-12-200212170-00008
-
Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149(2):315-352. doi:10.1016/j.chest.2015.11.026
-
5. Stevens SM, Woller SC, Baumann Kreuziger L, et al. Antithrombotic therapy for VTE disease: CHEST guideline update. Chest. 2021;160(6):e545-e608. doi:10.1016/j.chest.2021.07.055
-
6. Khairani CD, Bejjani A, Assi A, et al. Direct oral anticoagulants for treatment of venous thrombosis. Res Pract Thromb Haemost. 2024;8(4):102424.
-
7. Ferreira T, Huber SC, de Moraes Martinelli B, et al. Low prevalence of post-thrombotic syndrome in patients treated with rivaroxaban. Vascul Pharmacol. 2020;124:106608. doi:10.1016/j.vph.2019.106608
-
8. van Es N, Coppens M, Schulman S, Middeldorp S, Büller HR. Direct oral anticoagulants compared with vitamin K antagonists for acute venous thromboembolism. Blood. 2014;124(12):1968-1975. doi:10.1182/blood-2014-04-571232
-
9. Kahn SR, Galanaud JP, Vedantham S, Ginsberg JS. Guidance for the prevention and treatment of the post-thrombotic syndrome. J Thromb Thrombolysis. 2016;41(1):144-153. doi:10.1007/s11239-015-1312-5
-
10. Erol ME, Özyalçın S, Tekin KA, Diken Aİ, Yalçınkaya A, Ünal EU. Factors affecting recanalization in femoropopliteal deep vein thrombosis. Clin Appl Thromb Hemost. 2023;29:10760296231173409. doi:10.1177/10760296231173409
-
11. Enden T, Haig Y, Kløw NE, et al. Long-term outcome after additional catheter-directed thrombolysis versus standard anticoagulation for acute iliofemoral deep vein thrombosis. Lancet. 2012;379(9810):31-38. doi:10.1016/S0140-6736(11)61753-4
-
12. Bardetta M, Vedantham S, Kahn SR, et al. Residual vein thrombosis and its clinical implications. J Clin Med. 2025;14(17):5991.
-
13. The EINSTEIN Investigators. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363(26):2499-2510. doi:10.1056/NEJMoa1007903
Figures
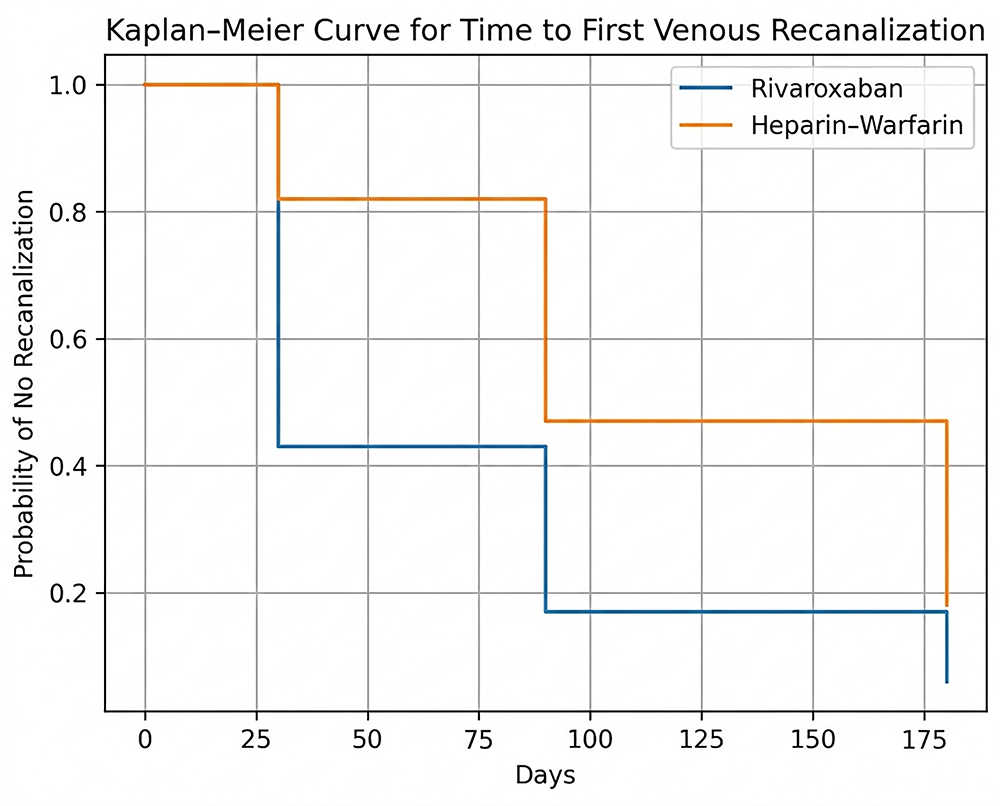
Figure 1. Kaplan–Meier curves showing time to first venous recanalization in patients treated with rivaroxaban versus heparin–warfarin. Rivaroxaban therapy was associated with significantly earlier recanalization (log-rank p < 0.001)
Tables
Table 1. Baseline demographic and clinical characteristics
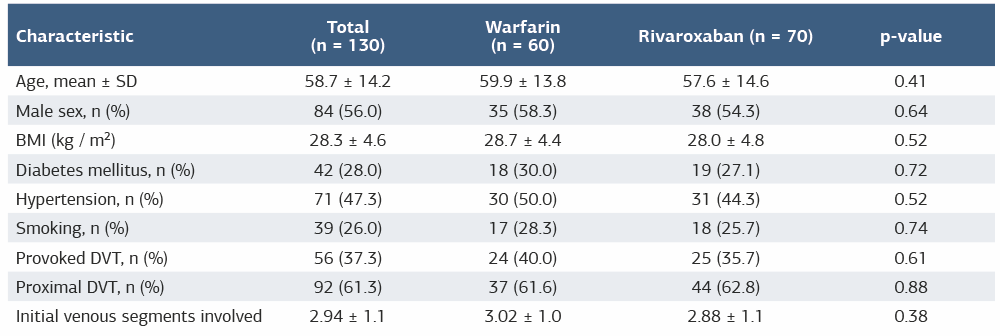
Table 2. Venous recanalization and clinical outcomes according to anticoagulant strategy
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Emced Khalil. Comparison of early and mid-term recanalization in deep venous thrombosis treated with rivaroxaban versus heparin–warfarin: a five-year retrospective study. Ann Clin Anal Med 2026;17(3):227-231
- Received:
- December 16, 2025
- Accepted:
- January 19, 2026
- Published Online:
- January 26, 2026
- Printed:
- March 1, 2026