
Colostomy in Fournier’s Gangrene: is it always necessary?
Colostomy in Fournier’s Gangrene
Authors
Abstract
Aim Fournier’s gangrene is a rapidly progressing necrotizing infection of the perineal, genital, and perianal regions with high morbidity and mortality. The necessity of colostomy in preventing fecal contamination and improving outcomes remains controversial. This study aimed to assess the role of colostomy in patients surgically treated for Fournier’s gangrene.
Methods This retrospective single-center study included 107 patients treated for Fournier’s gangrene between May 2017 and April 2025. Patients were grouped according to colostomy status. Demographic characteristics, comorbidities, laboratory values, hospital stay, and mortality were compared. Statistical analyses were performed using appropriate parametric and nonparametric tests, with significance defined as p < 0.05.
Results Mortality was significantly higher in the colostomy group (57.14%) than in the non-colostomy group (12.0%, p = 0.009). Colostomy was performed in cases with sphincter injury, advanced fecal contamination, impaired consciousness, or poor treatment adherence. In patients managed without colostomy, meticulous wound care, repeated debridement, and structured patient education effectively controlled fecal contamination. Colostomy was associated with longer hospital stays, additional surgical interventions, increased costs, and reduced quality of life.
Conclusion Routine colostomy is not required in most Fournier’s gangrene cases. Early debridement, broad-spectrum antibiotics, and careful wound management are generally sufficient to control infection. Colostomy should be reserved for selected patients, and high-quality postoperative care and multidisciplinary support remain essential for favorable outcomes.”
Keywords
Introduction
Fournier’s gangrene (FG) is a rare, fulminant necrotizing fasciitis affecting the subcutaneous soft tissues and fascia of the perineal, genital, and perianal regions, and is associated with high morbidity and mortality.1,2 Most cases arise from mixed bacterial infections involving Gram-positive and Gram-negative organisms, with fungal pathogens detected only occasionally.³
FG can affect individuals of all ages, yet several predisposing factors have been identified, including diabetes mellitus, advanced age, male sex, obesity, immunosuppression, chronic kidney disease, and alcoholism.4,5 The most common initiating factor is inadequately drained perianal abscesses, especially in the early stages, while genitourinary infections, colorectal carcinoma, rectal perforation, acute diverticulitis, and routine anorectal procedures such as hemorrhoid band ligation can also be sources.6
Due to its rapid progression, FG represents a life-threatening surgical emergency that requires early recognition and aggressive treatment.7 Reported mortality rates vary from 0% to 42%, most often resulting from fulminant sepsis and subsequent multi-organ failure.6
The cornerstone of treatment is aggressive surgical debridement combined with broad-spectrum antibiotic therapy. In selected cases, colostomy may be performed to control fecal contamination.8 Involvement of the penis and scrotum carries a relatively low risk of contamination, making colostomy unnecessary in many cases. However, perianal involvement may benefit from diversion to promote wound healing and prevent fecal contamination, particularly in patients with fecal incontinence or rectal perforation.9
Data on the impact of diversion on mortality in FG remain limited, and whether stomas improve survival is still debated.10 Furthermore, stoma formation itself may result in several adverse outcomes, including increased stoma output, renal failure, intestinal obstruction, stoma-related prolapse or hernia, injury to the bowel, leakage after reversal, and sepsis.11
Soft tissue defects resulting from FG can be reconstructed using techniques such as skin grafts, flap procedures, or testicular transposition.12
This study aimed to assess whether colostomy is necessary in the management of patients with Fournier’s gangrene.
Materials and Methods
Between May 2017 and April 2025, 107 patients who underwent surgery due to FG were included in this retrospective study. Ethical approval was obtained from the local ethics committee on May 25, 2025, under protocol number 2025/616. All patients provided written consent after being fully informed about the surgical procedure.
The study included patients older than 18 years with FG associated with involvement of the perianal region and with complete clinical data. Patients under 18, those with missing data, or those with underlying malignancies were excluded. Patient information was retrieved from institutional medical files, and additional details were collected through telephone communication when required.
Patients were divided into two groups: those who underwent colostomy and those who did not. Age, sex, comorbidities, mortality, preoperative white blood cell (WBC) count, and hemoglobin levels were compared. The decision to perform colostomy was based on patient compliance and sphincter injury, with the procedure performed either during the initial or second debridement.
Initially, oral intake was restricted, and wound contamination by feces was prevented. Repeat debridements were performed as needed. Patients were educated on wound care after defecation, and regular dressing changes were applied. In compliant patients, contamination was effectively minimized without the need for colostomy. When indicated, a loop sigmoid colostomy was created via a small incision in the left lower quadrant. Following sufficient granulation and local control of infection, wound cultures were obtained. In the absence of microbial growth, definitive wound closure was undertaken—either through primary closure or flap-based reconstruction, tailored to the extent of tissue loss. Patients deemed suitable underwent colostomy reversal 3–6 months after the procedure.
Ethics ApprovalEthical approval was obtained from the local ethics committee on May 25, 2025, under protocol number 2025/616.
All patients provided written consent after being fully informed about the surgical procedure.
Statistical AnalysisData were analyzed using IBM SPSS Statistics for Windows, Version 21.0. Continuous variables are presented as mean ± standard deviation, and categorical variables as frequencies and percentages. The Independent Samples t-test was applied to variables with a normal distribution, whereas the Mann–Whitney U test was employed for those not meeting normality assumptions. For categorical parameters, comparisons were performed using either the Chi-square test or Fisher’s Exact test when the expected frequencies were insufficient.
A p-value less than .05 is considered statistically significant.
Reporting GuidelinesThis study was conducted and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for observational studies.
Results
A total of 107 patients were included, comprising 85 males (79.44%) and 22 females (20.56%), with a mean age of 59.64 ± 13.58 years. Colostomy was performed in 7 patients (6.54%), while 100 patients (93.46%) were managed without diversion. Among those receiving colostomy, 3 underwent the procedure during the first operation and 4 during the second.
The mean hospital stay for the 91 discharged patients was 28.97 ± 11.66 days. Diabetes mellitus was present in 93 patients (86.92%) and hypertension in 37 (34.58%). The mean number of comorbidities was 1.95 ± 1.06 (range 0–5) (Table 1).
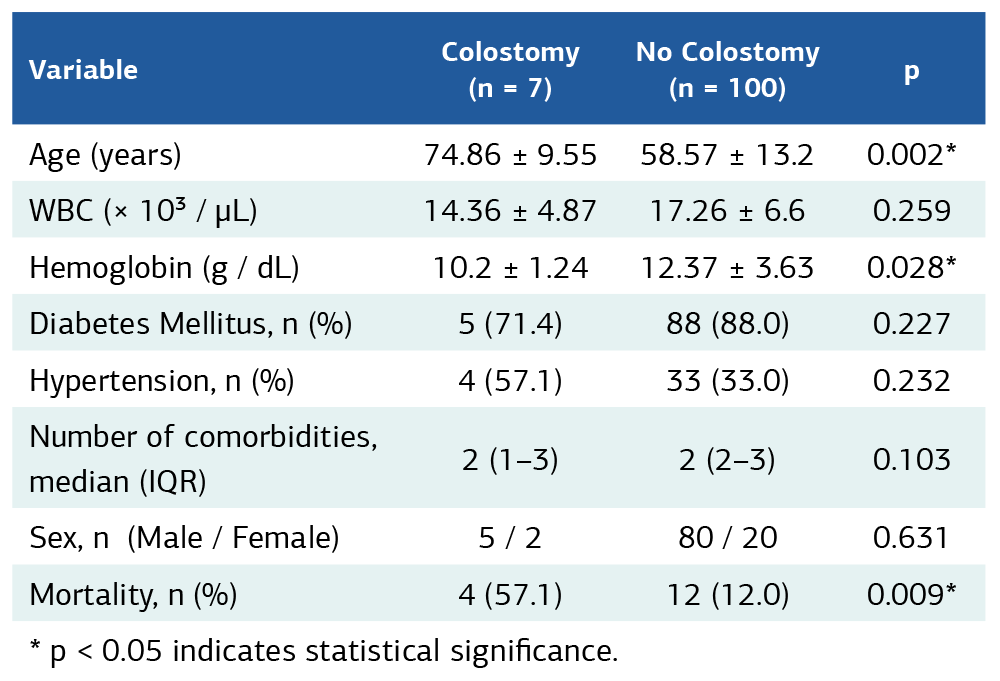
During follow-up, 91 patients were discharged, while 16 patients died during hospitalization. Mortality was 57.14% (4/7) in the colostomy group and 12.0% (12/100) in the non-colostomy group, with the difference being statistically significant (p = 0.009). When the groups were compared, statistically significant differences were observed in age and hemogram parameters at admission. No significant differences were found in other clinical parameters (Table 2).
Discussion
FG is a severe surgical emergency with high mortality rates and necessitates a multidisciplinary approach.2 In our study, mortality was significantly higher among patients who underwent colostomy. While the role of fecal diversion in the management of FG remains controversial in the literature, our findings suggest that colostomy is not required in every case and, conversely, may contribute to additional morbidity and mortality in selected patients.10
The main rationale for performing colostomy in FG is to prevent fecal contamination and facilitate wound healing. However, several studies have reported that fecal diversion does not confer a clear survival benefit and may even predispose patients to additional complications.4,5,10
A retrospective analysis emphasized that neither colostomy nor non-invasive fecal diversion techniques such as Flexi-Seal had a significant impact on mortality, and that surgical diversion should be deferred whenever possible.6 In our series, mortality was markedly higher among patients with colostomy (57.14%) compared to those managed without colostomy (12.0%), a finding that may suggest a negative influence of stoma formation on prognosis.
Nevertheless, this difference may not represent a direct causal relationship. Most patients who required colostomy presented with advanced disease, including anal sphincter injury, severe fecal contamination, impaired consciousness, or poor adherence to treatment. Therefore, the increased mortality is more likely attributable to the advanced baseline condition of this subgroup rather than the colostomy procedure itself.13,14
Potential complications of colostomy include electrolyte imbalances, stoma prolapse, parastomal hernia, anastomotic leakage, and renal dysfunction.11,13,15 Furthermore, colostomy is associated with prolonged hospital stays, the need for additional surgical interventions, increased healthcare costs, and a significant reduction in patient quality of life.10,16 These issues reinforce the need for cautious, individualized decision-making.
In our study, patients who did not undergo colostomy achieved effective prevention of fecal contamination with meticulous wound dressings, repeated debridement when necessary, and structured patient education. This approach not only minimized the need for additional surgical procedures but also supported recovery through less invasive means.17
Successful management of FG relies primarily on early diagnosis, aggressive surgical debridement, broad-spectrum antibiotic therapy, and intensive care support.5,6,10 Fecal diversion should be considered only in carefully selected patients, such as those with sphincter injury, rectal perforation, severe incontinence, impaired mental status, or poor compliance. In the absence of such indications, colostomy may expose patients to unnecessary morbidity and additional costs.9
The quality of postoperative care plays a pivotal role in patient outcomes. Regular and thorough wound dressing, maintenance of hygiene, and prevention of fecal contamination are essential. When such care is delivered by an experienced and qualified healthcare team, wound healing is accelerated, and complication rates are reduced.18,19
At the institution where this study was conducted, management of FG cases was facilitated by the availability of experienced surgical and nursing staff. This ensured consistent wound care, strict infection control, and the effective application of a multidisciplinary strategy. In our study, only 7 out of 107 patients (6.54%) required colostomy, a remarkably low rate that highlights the effectiveness of skilled wound management and infection control. The presence of an experienced team contributed to maintaining wound hygiene and meticulous postoperative care, thereby reducing the need for colostomy. Such an approach lowered morbidity and mortality while supporting faster recovery.
Limitations
The main limitations of this study are its retrospective design and the unequal number of patients between groups.
Conclusion
Colostomy does not appear to reduce mortality in FG and, on the contrary, may increase both complication rates and overall mortality. In most cases, early surgical debridement, appropriate antibiotic therapy, meticulous wound care, and patient education are sufficient to control fecal contamination. The decision to perform colostomy should be individualized according to patient characteristics, while the quality of postoperative care and multidisciplinary support are at least as important as the surgical intervention itself. The presence of experienced care teams improves infection control, enhances treatment adherence, and ultimately contributes to better survival outcomes.
Future large-scale prospective studies are needed to more clearly define the true indications for colostomy in FG.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Mersin University (Date: 2025-05-25, No: 2025/616).
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
All patients provided written informed consent after being fully informed about the surgical procedure.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: G.E.
Methodology: G.E., A.B.
Formal Analysis: G.E., R.O.Ü., B.S.
Investigation: G.E., S.S., R.O.Ü.
Data Curation: G.E., G.D.
Resources: G.E., A.B., G.D.
Writing – Original Draft Preparation: G.E.
Writing – Review & Editing: A.B., R.O.Ü., G.D., S.S., B.S.
Visualization: G.E., S.S.
Supervision: G.E.
Project Administration: G.E.
Validation: G.E., B.S.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
AHA: American Heart Association
ALS: Advanced Life Support
CPR: Cardiopulmonary Resuscitation
ECMO: Extracorporeal Membrane Oxygenator
ECPR: Extracorporeal Cardiopulmonary Resuscitation
ERC: European Resuscitation Council
EWS: Early Warning System
EWSS: Early Warning Scoring System
References
-
Ucaner B, Kesikli SA, Buldanli MZ, Ciftci MS, Hancerliogullari O. Fournier’s Gangrene: evaluation of patient outcomes using clinical data and prognostic biomarkers. J Coll Physicians Surg Pak. 2023;33(3):275-280. doi:10.29271/jcpsp.2023.03.275
-
Mahmood BA, ElSayed EH, Ali SA. Effect of colostomy on treatment outcome in Fournier Gangrene: a prospective comparative study. Plast Surg (Oakv). 2023;31(1):24-28. doi:10.1177/22925503211024757
-
Wróblewska M, Kuzaka B, Borkowski T, Kuzaka P, Kawecki D, Radziszewski P. Fournier’s gangrene--current concepts. Pol J Microbiol. 2014;63(3):267-273.
-
El-Qushayri AE, Khalaf KM, Dahy A, et al. Fournier’s Gangrene mortality: a 17-year systematic review and meta-analysis. Int J Infect Dis. 2020;92:218-225. doi:10.1016/j.ijid.2019.12.030
-
Jallali N. Necrotising fasciitis: its aetiology, diagnosis and management. J Wound Care. 2003;12(8):297-300. doi:10.12968/jowc.2003.12.8.26523
-
Ortega Ferrete A, López E, Juez Sáez LD, et al. Fournier’s Gangrene and fecal diversion. When, in which patients, and what type should I perform?. Langenbecks Arch Surg. 2023;408(1):428. doi:10.1007/s00423-023-03137-3
-
Tarchouli M, Bounaim A, Essarghini M, et al. Analysis of prognostic factors affecting mortality in Fournier’s Gangrene: a study of 72 cases. Can Urol Assoc J. 2015;9(11-12):E800-4. doi:10.5489/cuaj.3192
-
Kopechek KJ, Patel HV, Koch GE. Modern management of Fournier’s Gangrene. Curr Urol Rep. 2025;26(1):47. doi:10.1007/s11934-025-01275-3
-
Akcan A, Sözüer E, Akyildiz H, Yilmaz N, Küçük C, Ok E. Necessity of preventive colostomy for Fournier’s Gangrene of the anorectal region. Ulus Travma Acil Cerrahi Derg. 2009;15(4):342-346.
-
Sarofim M, Di Re A, Descallar J, Toh JWT. Relationship between diversional stoma and mortality rate in Fournier’s gangrene: a systematic review and meta-analysis. Langenbecks Arch Surg. 2021;406(8):2581-2590. doi:10.1007/s00423-021-02175-z
-
Sherman KL, Wexner SD. Considerations in stoma reversal. Clin Colon Rectal Surg. 2017;30(3):172-177. doi:10.1055/s-0037-1598157
-
Insua-Pereira I, Ferreira PC, Teixeira S, Barreiro D, Silva Á. Fournier’s Gangrene: a review of reconstructive options. Cent European J Urol. 2020;73(1):74-79. doi:10.5173/ceju.2020.0060
-
Desai R, Batura D. A contemporaneous narrative review of Fournier’s Gangrene. Urologia. 2023;90(2):201-208. doi:10.1177/03915603231165067
-
Huang S, Chen DC, Perera M, Lawrentschuk N. Role of diverting colostomy and reconstruction in managing Fournier’s Gangrene-a narrative review. BJU Int. 2024;134(4):534-540. doi:10.1111/bju.16365
-
Yanar H, Taviloglu K, Ertekin C, et al. Fournier’s Gangrene: risk factors and strategies for management. World J Surg. 2006;30(9):1750-1754. doi:10.1007/s00268-005-0777-3
-
Mayoral V, Coquerel-Beghin D, Cornu JN, Bridoux V, Auquit-Auckbur I, Pfister C. Impact of fecal diversion in perineal necrotizing soft tissue infection on disease survival: a large retrospective study. Surg Pract Sci. 2024;16:100231. doi:10.1016/j.sipas.2024.100231
-
Dupont M, Leal C, Tenreiro N, Marques R, Pinto-de-Sousa J. Fournier Gangrene management: is a stoma mandatory? Cureus. 2023;15(5):e39450. doi:10.7759/cureus.39450
-
Wang J, Yuan T, Shi J. Application of medical-nursing integration multidisciplinary-assisted surgical wound nursing mode in improving the quality of wound treatment. Emerg Med Int. 2022;2022:9299529. doi:10.1155/2022/9299529
-
Bisgaard EK, Bulger EM. Current diagnosis and management of necrotizing soft tissue infections: what you need to know. J Trauma Acute Care Surg. 2024;97(5):678-686. doi:10.1097/TA.0000000000004351
Tables
Table 1. General characteristics and clinical findings: 107 patients with Fournier’s Gangrene
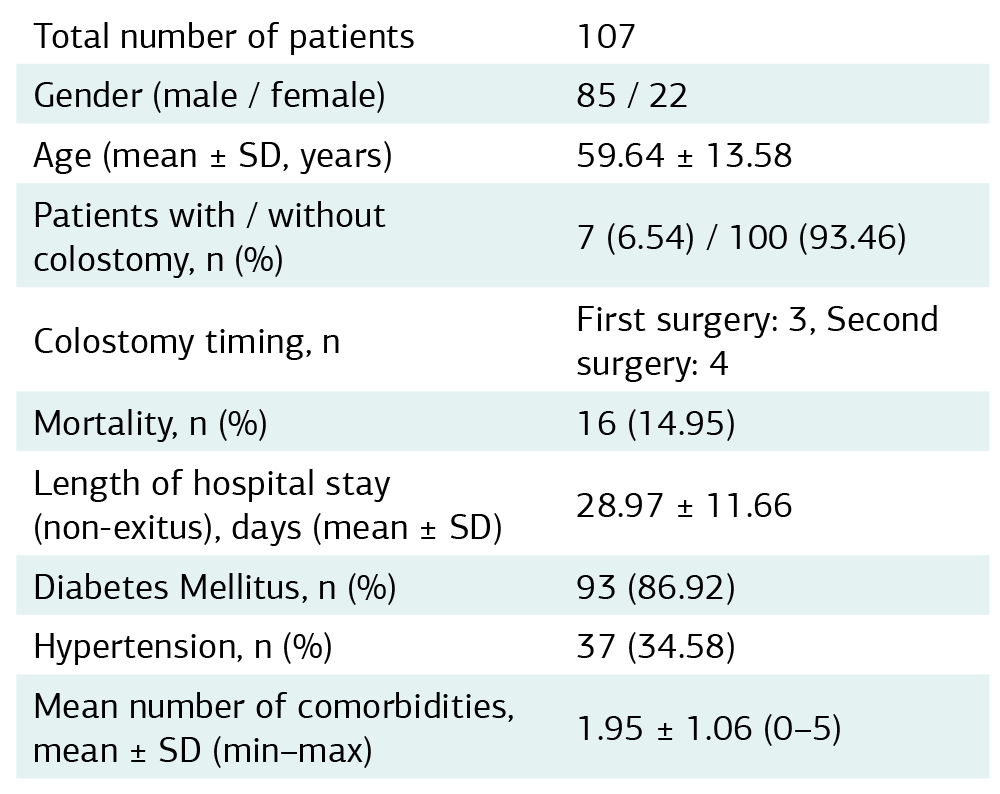
Table 2. Clinical characteristics of Fournier’s Gangrene patients with and without colostomy
* p < 0.05 indicates statistical significance.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Erdoğrul Güven, Börekoğlu Ali, Üstün Recep Okan, Diner Güvenç, Sayar Samed, Saylam Barış. Colostomy in Fournier’s gangrene: is it always necessary? Ann Clin Anal Med 2026;17(Suppl 1):65-68
- Received:
- December 18, 2025
- Accepted:
- February 10, 2026
- Published Online:
- February 19, 2026
- Printed:
- February 20, 2026