
Inflammatory and nutritional indices predict pCR in HER2+ breast cancer: retrospective cohort study
Inflammation/nutrition indices and pCR
Authors
Abstract
Aim Systemic inflammation and nutritional status may influence response to neoadjuvant therapy in HER2-positive breast cancer, yet simple low-cost predictors of pathologic complete response (pCR) are limited. We evaluated NLR, LMR, SII, and PNI as baseline predictors of pCR.
Methods This retrospective single-center study included 70 HER2-positive patients treated with anthracycline/taxane-based neoadjuvant chemotherapy plus dual anti-HER2 therapy, followed by surgery. Pretreatment blood counts and albumin were used to calculate NLR, LMR, SII, and PNI. ROC analyses estimated discrimination and optimal cut-offs; associations with pCR were tested, and multivariable logistic regression assessed independent predictors.
Results pCR occurred in 60.0% of patients. PNI showed the highest discriminatory ability with a borderline association with pCR, and LMR showed a similar non-significant trend. NLR and SII performed poorly and were not associated with pCR. None of the indices remained independently predictive in multivariable logistic regression.
Conclusion In this relatively homogeneous cohort receiving contemporary dual HER2 blockade, inflammation-ratio markers (NLR/SII) may be less informative, potentially because effective targeted therapy attenuates the influence of baseline systemic inflammation on response. By contrast, PNI—integrating lymphocyte status and nutritional reserve—showed the most consistent signal and may better capture host factors related to immune competence and treatment tolerance that contribute to pCR. However, the retrospective design and limited sample size restrict inference; validation in larger prospective cohorts is warranted.
Keywords
Introduction
Breast cancer is the most commonly diagnosed malignancy among women worldwide and remains a leading cause of cancer-related mortality. It accounts for approximately 30% of newly diagnosed cancers and 15% of cancer- related deaths in women 1. Current international guidelines recommend a multimodal treatment approach—including surgery, chemotherapy, targeted therapy, endocrine therapy, radiotherapy, and immunotherapy—tailored according to tumor biology and disease stage 1. Among these strategies, neoadjuvant chemotherapy has gained increasing importance, particularly in patients with axillary lymph node involvement. Administered prior to surgery, neoadjuvant therapy offers several advantages, such as tumor downstaging, increasing breast-conserving surgery rates, and potentially reducing distant metastasis risk. However, not all breast cancer patients achieve a pathological complete response (pCR) after receiving neoadjuvant chemotherapy 1. Pathological complete response is defined as the absence of invasive tumor in both the breast and axillary lymph nodes, although carcinoma in situ may be present 2.
Achieving a pCR is recognized as a strong surrogate marker for favorable long-term outcomes, especially in HER2-positive and triple-negative breast cancer (TNBC) subtypes 3,4. Conversely, patients who fail to achieve pCR exhibit worse prognosis and a higher likelihood of recurrence 5. In addition to intrinsic tumor characteristics, an expanding body of evidence suggests that host-related systemic inflammation and nutritional status play a pivotal role in modulating tumor progression, treatment response, and survival 6,7. The tumor microenvironment, composed of diverse inflammatory cells and mediators, has emerged as a key determinant of cancer behavior 8. Circulating immune and inflammatory cells—including neutrophils, lymphocytes, monocytes, and platelets—reflect systemic immune status and have been linked to prognosis in various malignancies. Several hematological indices derived from these parameters have been proposed as accessible and cost-effective biomarkers of cancer-related inflammation. Among them, the systemic immune-inflammation index (SII), calculated from platelet, neutrophil, and lymphocyte counts, has been identified as an adverse prognostic factor across multiple tumor types 9. Similarly, the prognostic nutritional index (PNI), calculated using serum albumin and lymphocyte count, has shown prognostic value across multiple cancer types, with lower PNI values consistently associated with poorer survival outcomes 10,11,12. Other well-studied inflammatory markers include the neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR), both of which have been reported as prognostic indicators in various malignancies 13,14. The lymphocyte-to-monocyte ratio (LMR), another index of systemic inflammation, has been associated with prognosis in diffuse large B-cell lymphoma, colorectal cancer, esophageal carcinoma, and lung cancer 15,16,17,18. Moreover, systemic inflammation and host immune status may influence the response to chemotherapy, suggesting that inflammatory and nutritional biomarkers could potentially predict pCR following neoadjuvant therapy 19,20.
Study RationaleDespite advancements in neoadjuvant systemic therapy, predicting which patients will achieve pCR remains a major unmet need in HER2-positive breast cancer. Although molecular subtype is a major determinant of treatment sensitivity, tumor- independent host factors—particularly systemic inflammation and nutritional status—may significantly influence treatment responsiveness. Inflammatory and nutritional indices such as NLR, LMR, SII, and PNI are inexpensive, non-invasive, and routinely measured in clinical practice, making them promising candidates for response prediction. However, existing evidence for their predictive value in HER2-positive breast cancer is inconsistent, partly due to heterogeneous study populations. Therefore, a focused investigation within a homogeneous HER2-positive cohort is warranted to clarify their potential clinical utility.
Study ObjectivesThe primary objective of this study was to evaluate the predictive performance of pre-treatment NLR, LMR, SII, and PNI in determining pCR following neoadjuvant systemic therapy in patients with HER2-positive breast cancer. The specific aims were to: assess the discriminatory ability of each biomarker using receiver operating characteristic (ROC) analysis; determine optimal cut-off values using the Youden Index; examine the association between dichotomized biomarker levels and pCR using univariate statistical testing; and evaluate the independent predictive contribution of each marker through multivariate logistic regression 1,2,3,4. These analyses sought to determine whether readily obtainable inflammatory and nutritional biomarkers could support clinical decision-making by identifying patients more likely to benefit from neoadjuvant therapy.
Materials and Methods
This retrospective, single-center study included 70 patients with HER2-positive breast cancer who received neoadjuvant systemic therapy followed by definitive surgery. Clinical, pathological, and laboratory data were obtained from institutional electronic medical records. Patients with complete baseline hematologic parameters required to calculate NLR, LMR, SII, and PNI were included; cases with missing laboratory values were excluded. All patients received anthracycline- and taxane-based neoadjuvant chemotherapy combined with dual anti-HER2 therapy per institutional practice. Pathologic complete response (pCR) was defined as the absence of residual invasive carcinoma in the breast and axillary lymph nodes (ypT0/Tis ypN0), as assessed by an experienced breast pathologist.
Baseline complete blood count parameters and serum albumin levels were collected prior to treatment initiation. NLR, LMR, SII, and PNI were calculated using standard formulas from pre- treatment values only. Continuous variables are presented as median (IQR) and categorical variables as n (%); normality was assessed with the Shapiro–Wilk test. ROC analyses evaluated discriminatory performance for pCR (AUC, 95% CI), and optimal cut-offs were derived using the Youden index and are shown in Table 1; biomarkers were dichotomized accordingly. Associations with pCR were tested using chi-square or Fisher’s exact test and reported as ORs (95% CI). Multivariable logistic regression, including NLR, LMR, SII, and PNI, assessed the independent predictive value. Two-sided p < 0.05 was considered significant; analyses were performed in SPSS v27.0
Ethical ApprovalThis study was approved by the Ethics Committee of Gaziantep City Hospital (Date: 2023-12-17, No: 350/2025).
Results
The cohort had a median age of 53 years (IQR 43.0–63.25) and was predominantly composed of invasive ductal carcinoma (90.0%). Most patients presented with stage II disease, and 55.7% were postmenopausal. ER and PR positivity were observed in 58.6% and 44.3%, respectively, and HER2 IHC 3+ was present in 87.1%. Tumors were mainly grade 2 (52.9%), and nearly all patients received AC-based dual anti-HER2 neoadjuvant therapy (97.1%). Overall, pCR was achieved in 60.0% of patients (Supplementary Table S1).
ROC Analysis of Inflammatory and Nutritional IndicesROC analyses were performed to assess the discriminatory abilities of NLR, LMR, SII, and PNI for predicting pCR. NLR demonstrated poor discriminative performance, with an AUC of 0.427 (SE: 0.072; p = 0.303; 95% CI: 0.286–0.568). The optimal cut-off value (1.37) yielded a high sensitivity of 81.0%, but a low specificity of 14.3%, and the negative Youden Index indicated no meaningful predictive capacity. LMR showed modest discrimination, with an AUC of 0.598 (SE: 0.069; p = 0.168; 95% CI: 0.462–0.734). The Youden-derived cut-off of 3.36 provided 76.2% sensitivity and 39.3% specificity. SII exhibited poor predictive ability, with an AUC of 0.447 (SE: 0.074; p = 0.457; 95% CI: 0.303–0.592) and an optimal cut-off of 353, corresponding to 81.0% sensitivity and 25.0% specificity. Among all indices, PNI demonstrated the highest accuracy, with an AUC of 0.635 (SE: 0.068; p = 0.057; 95% CI: .503–0.768). The optimal cut-off value for PNI (52.4) yielded 81.0% sensitivity and 39.3% specificity, representing the strongest—though still moderate—discriminatory performance (Supplementary Figure S1).
Association Between Cut-Off–Based Groups and pCR
Dichotomization of indices using ROC-derived thresholds revealed that PNI demonstrated the most notable association with pCR. Patients with PNI ≥ 52.4 achieved pCR more frequently than those below the cut-off (81.0% vs. 19.0%), and although this difference approached statistical significance, it did not meet the conventional threshold (χ² = 3.480, p = 0.062; OR = 2.75). LMR showed a positive but nonsignificant trend, with higher pCR rates observed in patients with LMR ≥ 3.36 (76.2% vs. 23.8%; χ² = 1.916, p = 0.166; OR = 2.07). SII and NLR demonstrated no significant associations with pCR. For SII, pCR occurred in 81.0% of patients with SII ≥ 353 and 19.0% of those below the threshold (χ² = 0.354, p = 0.552; OR = 1.42). NLR showed the weakest relationship, with pCR occurring at similar frequencies in both categories (χ² = 0.268, p = 0.605), and high NLR was associated with a nonsignificant 29% reduction in pCR likelihood (OR = 0.71). Overall, among all indices, PNI showed the strongest predictive trend, followed by LMR, whereas SII and NLR did not demonstrate meaningful discriminatory value (Supplementary Figure S2, Table 1).
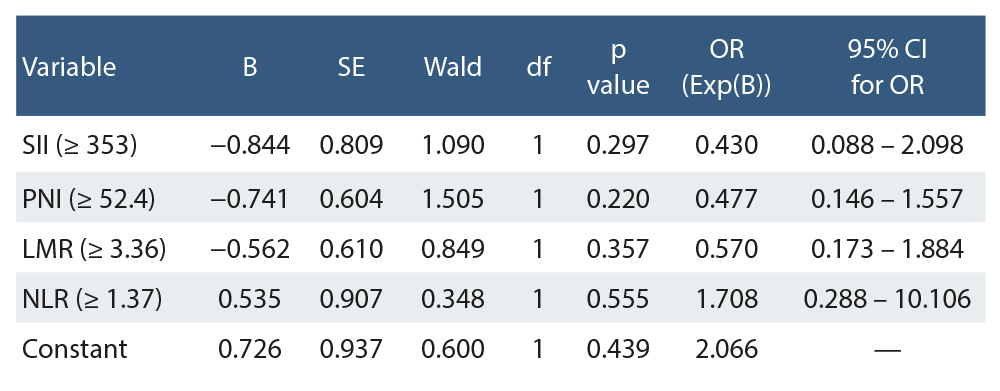
Multivariate Logistic Regression AnalysisA multivariate logistic regression model including SII, PNI, LMR, and NLR was constructed to evaluate their independent predictive value for pCR. None of the biomarkers emerged as a statistically significant independent predictor. SII showed a nonsignificant inverse association (B = −0.844, OR = 0.430, 95% CI: 0.088–2.098; p = 0.297). PNI demonstrated a nonsignificant reduction in pCR likelihood (B = −0.741, OR = 0.477, 95% CI: 0.146–1.557; p = 0.220). LMR showed a similarly nonsignificant trend (B = −0.562, OR = 0.570, 95% CI: 0.173–1.884; p = 0.357).
NLR displayed a nonsignificant positive association with pCR (B = 0.535, OR = 1.708, 95% CI: 0.288–10.106; p = 0.555).
None of the 95% confidence intervals excluded unity, indicating the absence of independent discriminatory capacity. These findings collectively suggest that none of the evaluated indices independently predicts pCR when adjusted for each other (Table 2).
Discussion
In this retrospective study of 70 patients with HER2-positive breast cancer treated with standardized dual anti-HER2 neoadjuvant systemic therapy, we assessed whether pre- treatment inflammatory and nutritional indices (NLR, LMR, SII, and PNI) could predict pathological pCR. Among these biomarkers, PNI exhibited the strongest association with treatment response, demonstrating the highest discriminatory accuracy (AUC = 0.635) and a notable trend toward predicting pCR, although statistical significance was not reached. LMR showed a similar but weaker directional trend, whereas SII and NLR displayed poor discriminative performance and no meaningful correlation with pCR. These findings suggest that, in contrast to classical systemic inflammation-based markers, baseline nutritional and immunologic status may have greater relevance in shaping response to neoadjuvant therapy in HER2-positive disease. Given that neoadjuvant chemotherapy— combined with targeted anti-HER2 therapy—has become a cornerstone of modern breast cancer management, yet does not uniformly result in complete eradication of invasive disease, the identification of reliable and accessible predictors remains clinically crucial for optimizing treatment strategies and improving patient outcomes. Moreover, previous studies have highlighted the important interplay between nutritional status and tumor progression 21,22,23. Further supporting the potential value of PNI as a biologically plausible predictor of treatment efficacy.
Malnutrition has been shown to adversely affect survival, treatment tolerance, and postoperative recovery in cancer patients, underscoring the importance of evaluating nutritional status prior to therapy. PNI, derived from serum albumin and peripheral lymphocyte counts, serves as an accessible tool for assessing long-term nutritional and immunological conditions 24,25. In our study, PNI demonstrated the strongest discriminatory ability among all investigated biomarkers and exhibited a clear positive trend toward predicting pCR, supporting previous evidence linking nutritional-immune competence with improved treatment outcomes. In contrast, systemic inflammatory processes are known to contribute to tumor initiation, progression, and therapeutic resistance 26. Classical inflammation-based indices, such as NLR and LMR, did not demonstrate significant predictive value in our HER2- positive cohort. In contrast, SII—a more recently developed systemic immune-inflammation index reflecting the combined influence of neutrophils, platelets, and lymphocytes has been reported to predict survival in several carcinomas 9,26,27,28. However, its performance in our cohort was similarly limited. These discrepancies may reflect subtype-specific differences, as prior research—such as the study by Chung et al.—showed that dynamic changes in NLR and PLR predicted neoadjuvant chemotherapy response in TNBC, and they even developed a nomogram integrating hematologic markers and imaging features to estimate pCR likelihood 29. The underlying biological rationale is supported by the functions of circulating immune cells. Neutrophils may promote tumor progression through the secretion of inflammatory mediators, platelets can facilitate tumor immune evasion by shielding malignant cells from NK cell–mediated cytotoxicity, and lymphocytes play a central role in anti-tumor immunity and cancer immunosurveillance 30,31,32,33. Monocytes and their derivatives, tumor-associated macrophages, further contribute to tumor proliferation, invasion, angiogenesis, and metastatic dissemination 34,35. Although numerous studies have demonstrated prognostic or predictive value for NLR and LMR in breast cancer across different subtypes 36,37.
Taken together, these findings indicate that the predictive value of systemic inflammatory markers may be considerably attenuated in HER2-positive breast cancer, likely due to the dominant immunologic mechanisms uniquely activated by HER2-directed therapies. Trastuzumab and pertuzumab exert potent immunomodulatory effects—most notably antibody- dependent cellular cytotoxicity—which depend more on functional effector lymphocytes and Fc-mediated immune activation than on baseline peripheral inflammatory ratios.
This may partly explain why indices such as NLR, LMR, and SII, which reflect generalized systemic inflammation, performed poorly in our analysis despite evidence of their prognostic utility in other breast cancer subtypes. Conversely, the relatively stronger performance of PNI suggests that broader host factors—such as nutritional reserve, immune competence, and systemic resilience—may have greater relevance in influencing pathologic response under HER2-targeted regimens. Given that low albumin levels and lymphopenia reflect chronic inflammation, impaired immunity, and metabolic stress, PNI may capture a multidimensional biological profile that is more directly aligned with treatment responsiveness than isolated inflammatory cell ratios. These observations underscore the importance of considering subtype-specific tumor biology when interpreting inflammation-based biomarkers and highlight the need for larger, mechanistically oriented studies to elucidate how nutritional-immune status interacts with targeted therapy– induced anti-tumor immunity in HER2-positive breast cancer.
Limitations
This retrospective, single-center study is subject to selection bias and limited generalizability. The small sample size (n = 70) likely reduced statistical power—especially in multivariable analyses—resulting in wide confidence intervals and borderline findings. Lymphovascular / peritumoral vascular invasion data were largely missing, and indices were calculated from a single baseline laboratory measurement, which may not reflect dynamic treatment-related immune changes. Inflammation- based markers can also be affected by infections, comorbidities, and medications, and subgroup heterogeneity within HER2- positive disease (including hormone receptor co-expression) could not be fully explored.
Conclusion
In this retrospective HER2-positive breast cancer cohort treated with dual anti-HER2 neoadjuvant therapy, NLR and SII showed poor ability to predict pCR, while LMR demonstrated only modest performance. PNI yielded the most favorable— though not statistically significant—signal, suggesting that baseline nutritional–immune reserve may be more informative than isolated inflammatory ratios in this setting. Therefore, inflammation-based indices should not be used alone for clinical decision-making; however, pretreatment PNI may serve as a practical adjunct for counseling and risk stratification, pending confirmation in larger prospective, multicenter cohorts. Future work should also clarify the biological link between nutritional– immune status and response to HER2-targeted therapy, evaluate dynamic changes in these indices during treatment, and explore whether integrating PNI with immune- or tumor- based biomarkers can improve predictive accuracy.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Gaziantep City Hospital (Date: 2023-12-17, No: 350/2025)
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
References
-
Ni XJ, Zhang XL, Ou-Yang QW, et al. An elevated peripheral blood lymphocyte- to-monocyte ratio predicts favorable response and prognosis in locally advanced breast cancer following neoadjuvant chemotherapy. PLoS One. 2014;9(11):e111886. doi:10.1371/journal.pone.0111886.
-
Charfare H, Limongelli S, Purushotham AD. Neoadjuvant chemotherapy in breast cancer. Br J Surg. 2005;92(1):14-23. doi:10.1002/bjs.4840.
-
von Minckwitz G, Untch M, Blohmer JU, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol. 2012;30(15):1796-804. doi:10.1200/JCO.2011.38.8595.
-
Symmans WF, Peintinger F, Hatzis C, et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. J Clin Oncol. 2007;25(28):4414-22. doi:10.1200/JCO.2007.10.6823.
-
ortazar P, Zhang L, Untch M, et al. Pathological complete response and long- term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164-72. doi:10.1016/S0140-6736(13)62422-8.
-
Kohler BA, Sherman RL, Howlader N, et al. Annual report to the nation on the status of cancer, 1975–2011, featuring incidence of breast cancer subtypes by race/ethnicity, poverty, and state. J Natl Cancer Inst. 2015;107(6):djv048. doi:10.1093/jnci/djv048.
-
Lu H, Ouyang W, Huang C. Inflammation, a key event in cancer development. Mol Cancer Res. 2006;4(4):221-33. doi:10.1158/1541-7786.MCR-05-0261.
-
Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140(6):883-99. doi:10.1016/j.cell.2010.01.025.
-
Gao Y, Zhang H, Li Y, Wang D, Ma Y, Chen Q. Preoperative increased systemic immune-inflammation index predicts poor prognosis in patients with operable non-small cell lung cancer. Clin Chim Acta. 2018;484:272-7. doi:10.1016/j.cca.2018.05.059.
-
Ikeya T, Shibutani M, Maeda K, et al. Maintenance of the nutritional prognostic index predicts survival in patients with unresectable metastatic colorectal cancer. J Cancer Res Clin Oncol. 2015;141(2):307-13. doi:10.1007/s00432-014-1799-8.
-
Wang DS, Luo HY, Qiu MZ, et al. Comparison of the prognostic values of various inflammation-based factors in patients with pancreatic cancer. Med Oncol. 2012;29(5):3092-100. doi:10.1007/s12032-012-0226-8.
-
Migita K, Takayama T, Saeki K, et al. The prognostic nutritional index predicts long-term outcomes of gastric cancer patients independent of tumor stage. Ann Surg Oncol. 2013;20(8):2647-54. doi:10.1245/s10434-013-2926-5.
-
Shibutani M, Maeda K, Nagahara H, et al. A high preoperative neutrophil- to-lymphocyte ratio is associated with poor survival in patients with colorectal cancer. Anticancer Res. 2013;33(8):3291-4.
-
Neofytou K, Smyth EC, Giakoustidis A, Khan AZ, Cunningham D, Mudan S. Elevated platelet-to-lymphocyte ratio predicts poor prognosis after hepatectomy for liver-only colorectal metastases and is superior to neutrophil-to-lymphocyte ratio. Med Oncol. 2014;31(10):239. doi:10.1007/s12032-014-0239-6.
-
Li YL, Pan YY, Jiao Y, Ning J, Fan YG, Zhai ZM. Peripheral blood lymphocyte/ monocyte ratio predicts outcome for patients with diffuse large B-cell lymphoma after standard first-line regimens. Ann Hematol. 2014;93(4):617-26. doi:10.1007/s00277-013-1916-9.
-
Stotz M, Pichler M, Absenger G, et al. The preoperative lymphocyte-to- monocyte ratio predicts clinical outcome in patients with stage III colon cancer. Br J Cancer. 2014;110(2):435-40. doi:10.1038/bjc.2013.785.
-
Huang Y, Feng JF. Low preoperative lymphocyte-to-monocyte ratio predicts poor cancer-specific survival in patients with esophageal squamous cell carcinoma. Onco Targets Ther. 2015;8:137-45. doi:10.2147/OTT.S73794.
-
Hu P, Shen H, Wang G, et al. Prognostic significance of systemic inflammation- based lymphocyte-to-monocyte ratio in patients with lung cancer. PLoS One. 2014;9(9):e108062. doi:10.1371/journal.pone.0108062.
-
Iyengar NM, Hudis CA, Dannenberg AJ. Obesity and inflammation: new insights into breast cancer development and progression. Am Soc Clin Oncol Educ Book. 2013;33:46-51. doi:10.1200/EdBook_AM.2013.33.46.
-
Ménard C, Martin F, Apetoh L, et al. Cancer chemotherapy: not only a direct cytotoxic effect, but also an adjuvant for antitumor immunity. Cancer Immunol Immunother. 2008;57(11):1579-87. doi:10.1007/s00262-008-0505-6.
-
Hong S, Zhou T, Fang W, et al. The prognostic nutritional index predicts overall survival of small-cell lung cancer patients. Tumour Biol. 2015;36(5):3389-97. doi:10.1007/s13277-014-2973-y.
-
Yang Y, Gao P, Chen X, et al. Prognostic significance of preoperative prognostic nutritional index in colorectal cancer: a retrospective cohort study and meta- analysis. Oncotarget. 2016;7(36):58543-52. doi:10.18632/oncotarget.10148.
-
Hayasaka K, Shiono S, Suzuki K, Endoh M, Okada Y. Postoperative prognostic nutritional index as a prognostic factor after non-small cell lung cancer surgery. Gen Thorac Cardiovasc Surg. 2020;68(10):1163-71. doi:10.1007/s11748-020-01366-7.
-
McMillan DC. Systemic inflammation, nutritional status and survival in patients with cancer. Curr Opin Clin Nutr Metab Care. 2009;12(3):223-6. doi:10.1097/MCO.0b013e32832a7902.
-
Gomes de Lima KV, Maio R. Nutritional status, systemic inflammation and prognosis of patients with gastrointestinal cancer. Nutr Hosp. 2012;27(3):707-14. doi:10.3305/nh/2012.27.3.5567.
-
Migita K, Matsumoto S, Wakatsuki K, et al. Effect of oral nutritional supplementation on the prognostic nutritional index in gastric cancer patients. Nutr Cancer. 2021;73(11-12):2420-7. doi:10.1080/01635581.2020.1826990.
-
Chen L, Kong X, Wang Z, Wang X, Fang Y, Wang J. Pre-treatment systemic immune-inflammation index is a useful prognostic indicator in patients with breast cancer undergoing neoadjuvant chemotherapy. J Cell Mol Med. 2020;24(5):2993-3021. doi:10.1111/jcmm.14934.
-
Wang Q, Zhu D. The prognostic value of systemic immune-inflammation index (SII) in patients after radical operation for carcinoma of stomach in gastric cancer. J Gastrointest Oncol. 2019;10(5):965-78. doi:10.21037/jgo.2019.05.03.
-
Chung WS, Chen SC, Ko TM, et al. An integrative clinical model for prediction of pathological complete response in operable stage II–III triple-negative breast cancer receiving neoadjuvant chemotherapy. Cancers (Basel). 2022;14(17):4170. doi:10.3390/cancers14174170.
-
Tan KW, Chong SZ, Wong FHS, et al. Neutrophils contribute to inflammatory lymphangiogenesis by increasing VEGF-A bioavailability and secreting VEGF-D. Blood. 2013;122(22):3666-77. doi:10.1182/blood-2012-11-466532.
-
Nieswandt B, Hafner M, Echtenacher B, Männel DN. Lysis of tumor cells by natural killer cells in mice is impeded by platelets. Cancer Res. 1999;59(6):1295-300.
-
Dunn GP, Old LJ, Schreiber RD. The immunobiology of cancer immunosurveillance and immunoediting. Immunity. 2004;21(2):137-48. doi:10.1016/j.immuni.2004.07.017.
-
Zikos TA, Donnenberg AD, Landreneau RJ, Luketich JD, Donnenberg VS. Lung T-cell subset composition at the time of surgical resection is a prognostic indicator in non-small cell lung cancer. Cancer Immunol Immunother. 2011;60(6):819-27. doi:10.1007/s00262-011-0996-4.
-
Noy R, Pollard JW. Tumor-associated macrophages: from mechanisms to therapy. Immunity. 2014;41(1):49-61. doi:10.1016/j.immuni.2014.06.010.
-
Qian BZ, Pollard JW. Macrophage diversity enhances tumor progression and metastasis. Cell. 2010;141(1):39-51. doi:10.1016/j.cell.2010.03.014.
-
Chen Y, Chen K, Xiao X, et al. Pretreatment neutrophil-to-lymphocyte ratio is correlated with response to neoadjuvant chemotherapy as an independent prognostic indicator in breast cancer patients. BMC Cancer. 2016;16:320. doi:10.1186/s12885-016-2352-8.
-
Marín Hernández C, Piñero Madrona A, Gil Vázquez PJ, et al. Usefulness of lymphocyte-to-monocyte, neutrophil-to-monocyte and neutrophil-to-lymphocyte ratios as prognostic markers in breast cancer patients treated with neoadjuvant chemotherapy. Clin Transl Oncol. 2018;20(4):476-83. doi:10.1007/s12094-017-1732-0.
Tables
Table 1. Association between inflammatory/nutritional indices and pathological complete response (pCR)
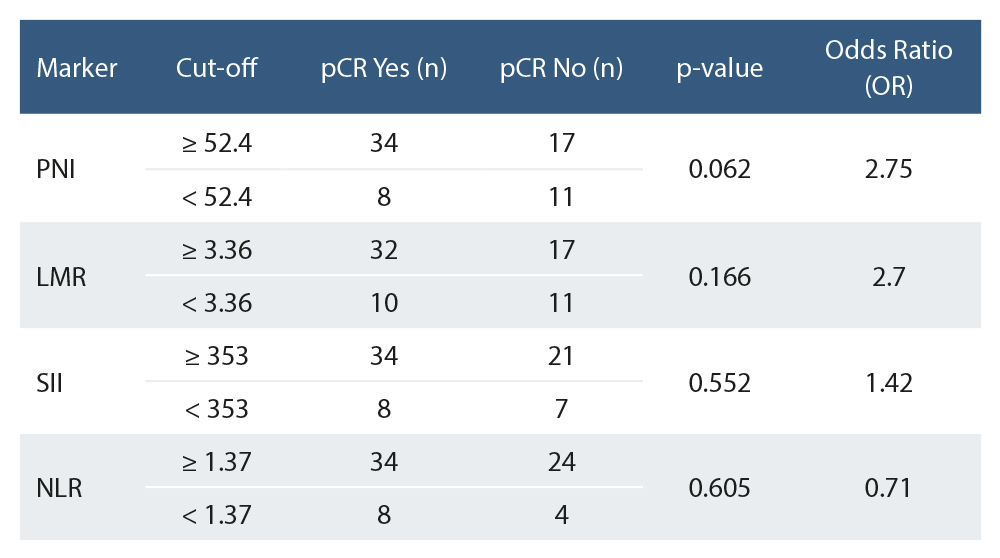
Table 2. Multivariate logistic regression analysis for predicting pathological complete response (pCR)
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ömer Faruk Kuzu, Çağlar Köseoğlu. Inflammatory and nutritional indices predict pCR in HER2+ breast cancer: retrospective cohort study. Ann Clin Anal Med 2026;17(2):163-167
- Received:
- December 23, 2025
- Accepted:
- January 23, 2026
- Published Online:
- January 24, 2026
- Printed:
- February 1, 2026