
The diagnostic utility of MMSE in legal decision-making capacity: results from a Turkish older adult sample
MMSE and legal capacity in older adults
Authors
Abstract
Aim This study aimed to examine the diagnostic utility of the Mini-Mental State Examination (MMSE) in discriminating legal decision-making capacity among older adults, using structured clinical capacity judgements as the reference standard. We evaluated the discriminatory performance of MMSE total and domain scores, identified optimal cut-off values, and assessed whether demographic variables improved classification accuracy.
Methods This retrospective study included 283 adults aged 65 years and older referred for legal capacity assessment in an outpatient psychiatry clinic in Türkiye. Logistic regression models and receiver operating characteristic analyses were conducted to assess diagnostic performance. Optimal thresholds were determined using the Youden Index, and sensitivity, specificity, likelihood ratios, and diagnostic odds ratios were calculated. Models adjusting for age, gender, and education were also examined.
Results The MMSE total score showed excellent discrimination for legal decision-making capacity (AUC = 0.97, 95% CI 0.94–0.99). A cut-off of 20.5 yielded high sensitivity (0.97) and specificity (0.86), with a very low negative likelihood ratio (0.03). Orientation demonstrated comparable performance, whereas other domains showed only fair-to-good accuracy. Demographic adjustments did not meaningfully improve model performance.
Conclusion MMSE performance, particularly total and orientation scores, closely reflected clinicians’ determinations of legal decision-making capacity. However, misclassification remained present, indicating that preserved global cognition does not uniformly guarantee intact capacity. These findings support the use of MMSE as a supportive indicator within a structured functional assessment, rather than as a stand-alone determinant, and highlight the continued importance of clinician judgement in capacity evaluations.
Keywords
Introduction
Legal decision-making capacity refers to a person’s ability to make informed, autonomous choices about medical, financial, or legal matters. This concept is generally defined through four core functional abilities: understanding relevant information, appreciating its personal implications, reasoning about alternatives, and communicating a choice.1,2 These abilities form the basis of widely accepted clinical and legal frameworks for assessing capacity.3
In everyday psychiatric and geriatric practice, clinicians frequently rely on structured clinical interviewing to evaluate these functional abilities. However, formal capacity assessment instruments are not routinely used in most outpatient settings due to time, training, and workflow constraints. As a result, brief cognitive screening measures are commonly used as adjunct tools to support clinical judgement. Among these, the mini-mental state examination (MMSE) is one of the most widely used and well-known instruments for evaluating global cognitive functioning in older adults.4
Although MMSE was originally developed as a screening test for cognitive impairment and dementia, research has consistently shown that MMSE scores are associated with decision-making ability. Lower MMSE scores are linked with a markedly increased likelihood of impaired decisional capacity, whereas higher scores are more often observed among individuals who retain capacity.5,6 For example, MMSE scores below 20 are associated with a higher likelihood of incapacity in treatment-related decisions, whereas scores above 24 are more often seen in patients judged to retain decision-making capacity.6 At the same time, the relationship is not absolute. Some individuals with normal MMSE scores may still lack capacity due to impaired judgement, insight, or reasoning, whereas a minority of patients with cognitive deficits may retain decision-making abilities. These findings highlight that MMSE should not be considered a substitute for functional assessment, but rather as a supportive diagnostic indicator.7
Despite its widespread clinical use, there remains limited empirical evidence regarding the diagnostic accuracy of MMSE scores when compared directly with clinicians’ structured capacity judgements in routine outpatient psychiatric practice. Much of the literature has focused instead on research assessments of treatment consent in hospital populations or dementia cohorts.8,9 Therefore, it is still unclear how effectively MMSE discriminates between individuals judged clinically to have or to lack legal decision-making capacity in real-world outpatient settings.
The present study seeks to clarify the diagnostic value of the MMSE in the context of legal decision-making capacity among older adults referred for psychiatric evaluation. In routine clinical practice, capacity judgements are based primarily on structured clinical assessment of decision-relevant functional abilities, with cognitive screening used only as an adjunct source of information. Within this context, we examined whether MMSE performance meaningfully reflects clinicians’ determinations of legal decision-making capacity. Specifically, we investigated the ability of MMSE total and domain scores to discriminate between individuals judged to have or to lack capacity, identified statistically optimal cut-off values and associated diagnostic indices (including sensitivity, specificity, likelihood ratios, and diagnostic odds ratios), and explored whether basic demographic variables further improved discrimination. By situating MMSE performance within a diagnostic framework, this study aims to clarify the extent to which MMSE scores can help inform legal-capacity evaluations in everyday psychiatric practice, and to provide evidence-based guidance on their appropriate interpretation.
Materials and Methods
ProcedureThis retrospective study was based on clinical records from the outpatient psychiatry clinics of Marmara University Pendik Training and Research Hospital, and included records dated between 1 March 2025 and 31 October 2025. Individuals aged 65 years and older who presented for assessment of mental state and legal decision-making capacity, and for whom the MMSE had been requested as part of the clinical evaluation, were included in the study. Patients with a known prior diagnosis of dementia, those who received a dementia diagnosis during the assessment, individuals diagnosed with mild cognitive impairment, and those with intellectual disability were excluded. As the institutional database routinely records only validly administered MMSE assessments, individuals who were illiterate or who were unable to complete the MMSE due to physical or mental health limitations were not included in the final sample.
In our clinic, final judgments regarding legal decision-making capacity are made independently by at least two psychiatrists (one resident and one board-certified consultant) following a structured mental state examination. Importantly, this determination is not primarily based on the MMSE; the MMSE is used only as a supportive cognitive screening tool within a broader, structured clinical evaluation. During the capacity assessment, clinicians systematically evaluate whether the individual is able to: i) form and express a treatment-related choice, ii) provide reasons for the chosen option and demonstrate logical consistency, iii) engage in rational deliberation, iv) understand and process relevant information.
Accordingly, the MMSE served only as an adjunct indicator of global cognitive functioning, whereas the final judgment regarding legal capacity reflected a multidimensional, clinically grounded capacity evaluation incorporating the domains above.
ParticipantsA total of 283 individuals met the inclusion criteria and were included in the final analysis.
Statistical AnalysisAll analyses were conducted in R (version 4.4.2). Descriptive statistics were computed for demographic, clinical, and cognitive variables (means, standard deviations, medians, interquartile ranges, and frequencies). The primary outcome was legal capacity (0 = lacks capacity, 1 = has capacity). Univariable logistic regression models were first fitted with MMSE total (Model 1) and each cognitive domain as predictors, and odds ratios (OR) with 95% confidence intervals (CI) were reported.
Two multivariable models were then estimated: Model 3 included MMSE total score, age, and gender; Model 4 additionally included education level (collapsed into higher vs. lower). Model performance was summarised using Akaike Information Criterion (AIC) and McFadden’s pseudo-R². Receiver operating characteristic (ROC) curves and area under the curve (AUC) estimates with 95% CI were obtained using the pROC package, and model AUCs were compared using DeLong’s test.10
For MMSE total, each subscale, and the multivariable models, optimal classification thresholds were determined using the Youden Index. At these thresholds, sensitivity, specificity, predictive values, likelihood ratios, and diagnostic odds ratios (DOR) with 95% CI were calculated. Missing data (2.3%) were handled via multiple imputation prior to modelling. All tests were two-tailed, with p < 0.05 considered statistically significant.
Ethical ApprovalEthical approval was approved by the Marmara University School of Medicine Non-Interventional Research Ethical Committee (Date: 2025-11-21, No: 09.2025.25-0913).
Reporting GuidelinesThis study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Results
Sample CharacteristicsA total of 283 older adults were included in the study. The mean age was 73.1 years (standard deviation (SD) = 9.3, range 65–94), and 58.7% of participants were female. Most participants were married (50.9%) or widowed (34.3%), and the majority had completed primary education or less (71.3%). Medical comorbidity was common (67.5%), whereas documented psychiatric comorbidity was present in 18.0%. Overall, 89.9% of participants were judged to have legal decision-making capacity. The mean MMSE total score was 26.1 (SD = 3.7), indicating generally preserved global cognitive performance. Orientation (Mean = 8.8, SD = 1.7) and language abilities (Mean = 8.1, SD = 1.1) were largely intact, whereas delayed recall showed greater variability (Mean = 2.3, SD = 1.0) (Supplementary Table 1).
Model PerformanceLogistic regression models predicting legal capacity demonstrated good overall fit for the MMSE total score and the Orientation subscale. Model fit indices were strongest for the MMSE total score (AIC = 57.66, McFadden R² = 0.64), followed by the model including MMSE with age and gender (AIC = 61.04, McFadden R² = 0.65). Adding education did not materially improve model fit (AIC = 62.62, McFadden R² = 0.65). In contrast, Registration showed poor fit (AIC = 145.88, McFadden R² = 0.05), while Recall, Language, and Attention/Calculation demonstrated intermediate explanatory power (McFadden R² = 0.16–0.33).
ROC Curve AnalysisROC analyses indicated that the MMSE total score demonstrated excellent discrimination for legal capacity (AUC = 0.97, 95% CI [0.94, 0.99]). Orientation also showed excellent performance (AUC = 0.96, 95% CI [0.93, 0.99]). The models that additionally adjusted for age and gender (AUC = 0.97, 95% CI [0.95, 0.99]) and for age, gender, and education (AUC = 0.97, 95% CI [0.95, 0.99]) showed no meaningful improvement in classification accuracy. In contrast, Registration demonstrated poor discrimination (AUC = 0.64, 95% CI [0.54, 0.74]), whereas Recall (AUC = 0.76, 95% CI [0.63, 0.88]), Language (AUC = 0.80, 95% CI [0.71, 0.90]), and Attention/Calculation (AUC = 0.86, 95% CI [0.77, 0.96]) showed only fair-to-good accuracy.
Pairwise comparisons of AUC values were conducted using the DeLong test. The MMSE total score showed significantly greater discrimination than Registration (Z = 6.45, p < 0.001), Recall (Z = 3.69, p < 0.001), Language (Z = 3.37, p < 0.001), and Attention/Calculation (Z = 2.57, p = 0.010). However, MMSE total did not differ significantly from Orientation (Z = 0.85, p > 0.05). Likewise, the AUC for the MMSE total score did not differ from models additionally adjusting for age and gender (Z = −0.57, p > 0.05) or for education (Z = −0.45, p > 0.05). The comparison between the two adjusted models was also nonsignificant (Z = −0.30, p > 0.05).
Diagnostic Performance of MMSE & Subscales and ModelsWhen optimal cut-off points were applied, the MMSE total score demonstrated excellent diagnostic accuracy for legal decision-making capacity. A cut-off of 20.5 yielded high sensitivity (0.97, 95% CI [0.95–0.99]) and high specificity (0.86, 95% CI [0.64–0.97]), with an overall accuracy of 0.96 (95% CI [0.94–0.98]). The positive likelihood ratio indicated a substantial increase in post-test probability (LR+ = 6.81, 95% CI [2.39–19.43]), while the negative likelihood ratio was very low (LR− = 0.03, 95% CI [0.01–0.07]). The corresponding diagnostic odds ratio was extremely high (DOR = 218.6, 95% CI [52.1–917.5]).
The Orientation subscale also showed very strong performance at a cut-off of 7.5, with sensitivity of 0.88 (95% CI [0.84–0.92]) and specificity of 0.95 (95% CI [0.76–1.00]). This resulted in a large LR+ (18.52, 95% CI [2.73–125.45]) and high DOR (149.0, 95% CI [19.3–1149.7]).
Model-based probability classifiers performed similarly. The MMSE-only probability model (Model 1) achieved identical accuracy to the raw score threshold (accuracy = 0.96), with LR− again approaching zero (0.03, 95% CI [0.01–0.07]). Adding age and gender (Model 3) or education (Model 4) did not meaningfully improve classification performance, despite LR+ values remaining high across models. The ROC curves for the logistic regression models are shown in Figure 1.
In contrast, Registration, Recall, Language, and Attention/Calculation demonstrated only modest discrimination with weaker likelihood ratios and lower DOR values compared with MMSE total and Orientation. ROC curves for the MMSE cognitive domains are presented in Figure 2. The detailed data are provided in Supplementary Table 1 and Table 2.
Discussion
This study examined whether MMSE performance is associated with psychiatrists’ determinations of legal decision-making capacity among older adults referred for assessment. MMSE total scores showed good discriminatory ability in distinguishing between individuals judged to have or to lack capacity, with several cognitive domains also related to capacity status. Optimal cut-off values produced clinically meaningful accuracy estimates, and demographic factors added only limited incremental value beyond the MMSE total score. Overall, the findings indicate that MMSE performance reflects key aspects of decision-relevant cognition, while reinforcing that it should support, rather than replace, structured clinical assessment.
Our results align with a substantial body of work indicating that global cognitive performance, as measured by the MMSE, is meaningfully associated with medical or legal decision-making capacity,11 but that this relationship is imperfect. Sessums and colleagues (2011) concluded that MMSE scores are informative primarily at the extremes, with very low scores increasing the likelihood of incapacity and higher scores reducing it, while emphasising that no single cut-off can safely substitute for a structured capacity assessment.6 Similarly, Whelan et al. (2009) found that MMSE scores predicted capacity to consent to research in care-home residents, identifying an optimal cut-point but also reporting substantial misclassification even at that threshold.12
Our finding that MMSE total scores showed good discrimination for clinician-judged legal capacity is consistent with prior work demonstrating that lower MMSE scores are associated with increased odds of lacking capacity in dementia and older adult populations.12,13,14 Studies conducted on psychiatric inpatients report a significant predictive relationship between lower scores on the MMSE and impaired decisional capacity.15
Although the MMSE demonstrated excellent discrimination in our sample, the derived cut-off values did not yield perfect classification. Both false positives and false negatives were observed, meaning that some individuals with high MMSE scores were judged to lack capacity, whereas others with lower scores retained it. This pattern mirrors previous reports emphasising that MMSE should not be applied as a stand-alone determinant of decision-making capacity, but rather interpreted alongside structured clinical assessment.7,16 Likewise, work comparing MMSE with the MacCAT-T has shown that some patients within the “normal” MMSE range still lack capacity by expert judgement, underscoring that specific abilities such as understanding, reasoning, and appreciation are not fully captured by a brief global screen.17 Within this context, our findings indicate that MMSE can provide useful diagnostic input when evaluating legal decision-making capacity; however, its results should always be interpreted as part of a structured, functional assessment rather than being used as an isolated determinant.
Domain-level results indicated that deficits in orientation and attention/calculation were most strongly associated with incapacity, whereas registration and recall were weaker predictors. This pattern is clinically consistent with the idea that decision-making relies heavily on situational awareness and sustained cognitive processing, rather than short-term repetition. Language performance also contributed, reflecting the importance of communicating and justifying a choice. Thus, beyond global cognitive decline, certain domains appear more directly relevant to legal decision-making capacity.
These findings suggest that MMSE scores can meaningfully assist clinicians in identifying individuals at increased likelihood of lacking legal decision-making capacity. Very low scores, in particular, may prompt closer functional assessment and more careful documentation. However, the presence of misclassification indicates that MMSE cannot be used as a stand-alone determinant. Rather, it should be interpreted as one component within a structured, clinician-led evaluation that also considers context, reasoning ability, and ethical obligations to balance autonomy with protection.
Limitations
Strengths of this study include its clinically grounded design, use of structured capacity assessment by two independent psychiatrists as the reference standard, and detailed reporting of diagnostic performance indices. However, the specialist outpatient setting may limit generalisability, and MMSE scores remain partly influenced by demographic factors. In addition, although criteria were applied systematically, capacity determination necessarily involves clinical judgement. Future research comparing MMSE with dedicated capacity assessment tools and across diverse clinical settings is warranted.
Conclusion
In this clinical sample of older adults referred for medico-legal assessment, MMSE performance showed a strong ability to discriminate between individuals judged to have or to lack legal decision-making capacity. These results indicate that cognitive impairment, particularly in specific domains, is closely linked to incapacity. However, misclassification remained present, confirming that MMSE cannot replace structured functional assessment. Instead, it should be used as a supportive tool that informs, but does not determine, clinical judgement in capacity evaluations.
Declarations
Ethics Declarations
Ethical approval was approved by the Marmara University School of Medicine Non-Interventional Research Ethical Comitee (Date: 2025-11-21; No: 09.2025.25-0913).
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
The requirement for informed consent was waived due to the retrospective design.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: E.A., Z.T., P.S., E.B.A., Ö.Y.
Methodology: E.A., Z.T., P.S., E.B.A., Ö.Y.
Software: E.A.
Validation: E.A.
Formal Analysis: E.A.
Investigation: E.B.A.
Resources: E.B.A.
Data Curation: E.A., E.B.A.
Writing – Original Draft Preparation: E.A., Z.T., P.S., E.B.A., Ö.Y.
Writing – Review & Editing: E.A., Z.T., P.S., E.B.A., Ö.Y.
Visualization: E.A.
Supervision: Ö.Y.
Project Administration: E.A.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and some of the main line, or all of the preparation and scientific review of the contents, and approval of the final version of the article.
Abbreviations
AIC: Akaike information criterion
AUC: Area under the curve
CI: Confidence interval
DOR: Diagnostic odds ratio
LR: Likelihood ratio
MMSE: Mini-Mental State Examination
OR: Odds ratio
ROC: Receiver operating characteristic
SD: Standard deviation
References
-
Bari BA, Beach SR. Evaluating capacity: Appelbaum’s framework interpreted diagrammatically. J Acad Consult Liaison Psychiatry. 2024;65(1):120-121. doi:10.1016/J.JACLP.2023.09.007
-
Palmer BW, Harmell AL. Assessment of healthcare decision-making capacity. Arch Clin Neuropsychol. 2016;31(6):530-540. doi:10.1093/ARCLIN/ACW051
-
Karlawish J. Measuring decision-making capacity in cognitively impaired individuals. Neurosignals. 2007;16(1):91-98.
-
Arevalo-Rodriguez I, Smailagic N, Roqué-Figuls M, et al. Mini-Mental State Examination (MMSE) for the early detection of dementia in people with mild cognitive impairment (MCI). Cochrane Database Syst Rev. 2021;(7):CD010783. doi:10.1002/14651858.CD010783.PUB3
-
Hegde S, Ellajosyula R. Capacity issues and decision-making in dementia. Ann Indian Acad Neurol. 2016;19(Suppl 1):S34-S39. doi:10.4103/0972-2327.192890
-
Sessums LL, Zembrzuska H, Jackson JL. Does this patient have medical decision-making capacity? JAMA. 2011;306(4):420-427. doi:10.1001/JAMA.2011.1023
-
Pachet A, Astner K, Brown L. Clinical utility of the mini-mental status examination when assessing decision-making capacity. J Geriatr Psychiatry Neurol. 2010;23(1):3-8. doi:10.1177/0891988709342727
-
John S, Rowley J, Bartlett K. Assessing patients decision-making capacity in the hospital setting: A literature review. Aust J Rural Health. 2020;28(2):141-148. doi:10.1111/AJR.12592
-
Parmigiani G, Del Casale A, Mandarelli G, et al. Decisional capacity to consent to treatment and research in patients affected by Mild Cognitive Impairment. A systematic review and meta-analysis. Int Psychogeriatr. 2022;34(6):529-542. doi:10.1017/S1041610220004056
-
Robin X, Turck N, Hainard A, et al. pROC: an open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinformatics. 2011;12:77. doi:10.1186/1471-2105-12-77
-
Lepping P, Stanly T, Turner J. Systematic review on the prevalence of lack of capacity in medical and psychiatric settings. Clin Med (Lond). 2015;15(4):337-343. doi:10.7861/CLINMEDICINE.15-4-337
-
Whelan PJP, Oleszek J, Macdonald A, Gaughran F. The utility of the Mini-mental State Examination in guiding assessment of capacity to consent to research. Int Psychogeriatr. 2009;21(2):338-344. doi:10.1017/S1041610208008314
-
Gregory R, Roked F, Jones L, Patel A. Is the degree of cognitive impairment in patients with Alzheimer’s disease related to their capacity to appoint an enduring power of attorney? Age Ageing. 2007;36(5):527-531. doi:10.1093/AGEING/AFM104
-
Kim SYH, Caine ED. Utility and limits of the mini mental state examination in evaluating consent capacity in Alzheimer’s disease. Psychiatr Serv. 2002;53(10):1322-1324. doi:10.1176/APPI.PS.53.10.1322
-
Cairns R, Maddock C, Buchanan A, et al. Prevalence and predictors of mental incapacity in psychiatric in-patients. Br J Psychiatry. 2005;187:379-385. doi:10.1192/BJP.187.4.379
-
Fassassi S, Bianchi Y, Stiefel F, Waeber G. Assessment of the capacity to consent to treatment in patients admitted to acute medical wards. BMC Med Ethics. 2009;10:15. doi:10.1186/1472-6939-10-15
-
Álvarez Marrodán I, Baón Pérez BS, Navío Acosta M, Verdura Vizcaino EJ, Cantón Álvarez MB, Ventura Faci T. Limits on the use of the MMSE for assessment of capacity to consent for treatment. Eur J Psychiatry. 2018;32(3):153-157. doi:10.1016/J.EJPSY.2018.02.003
Figures
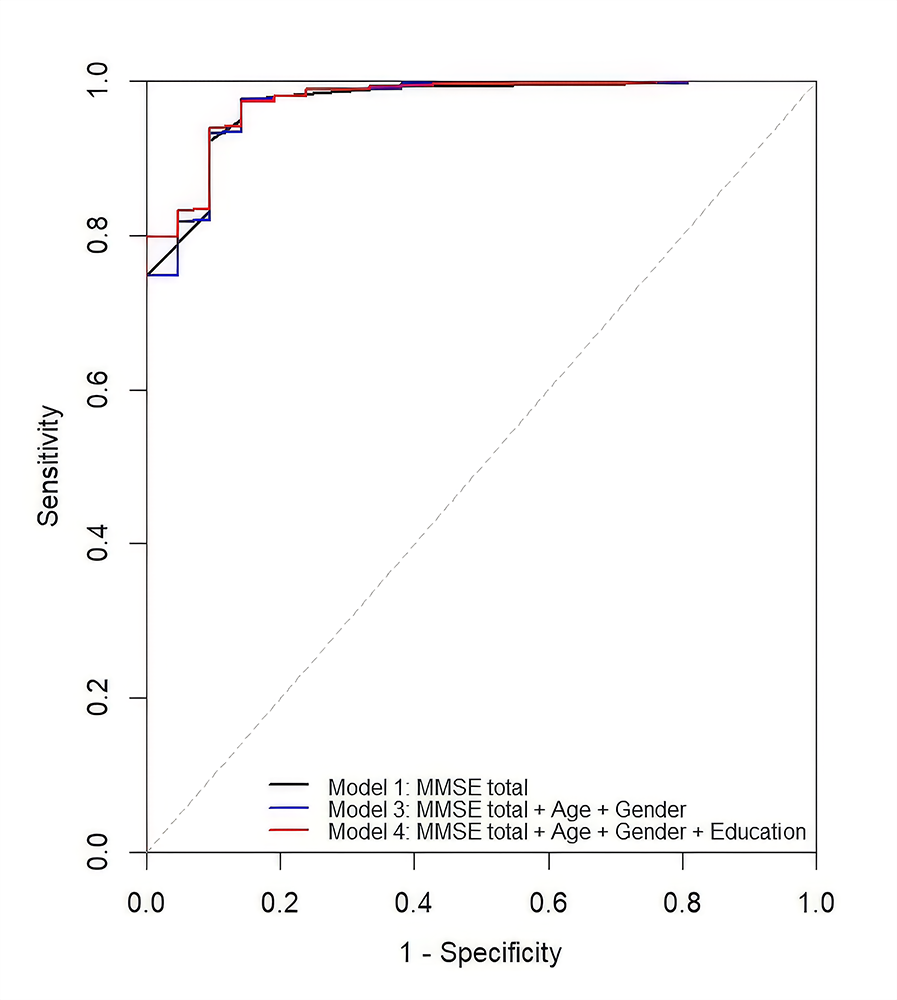
Figure 1. ROC curves comparing logistic regression models for legal decision-making capacity. All models showed high discrimination with minimal differences. The diagonal dashed line indicates chance performance
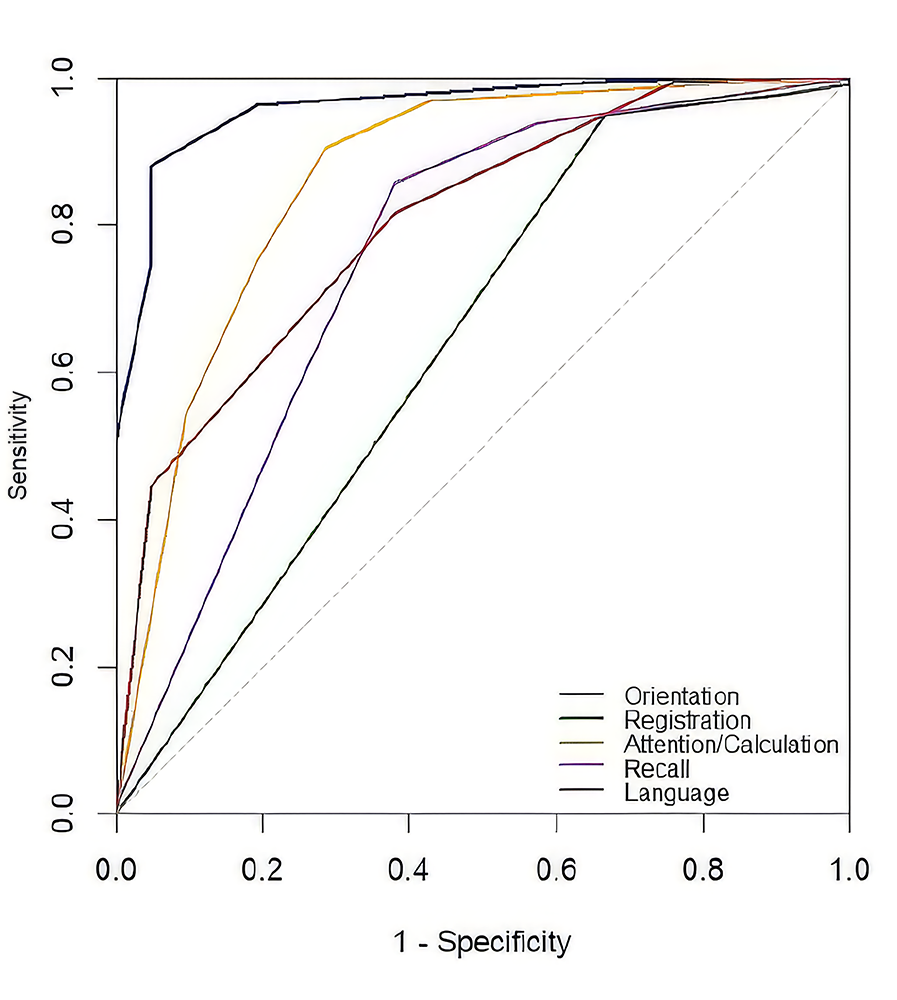
Figure 2. ROC curves for MMSE cognitive domains. Orientation and attention/calculation showed stronger discrimination than registration and recall. The diagonal dashed line indicates chance performance
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Erdoğdu Akça, Elif Başak Alço, Pelin Seçgin, Zeynep Teke, Ömer Yanartaş. The diagnostic utility of MMSE in legal decision-making capacity: results from a Turkish older adult sample. Ann Clin Anal Med 2026;17(3):244-248
- Received:
- January 11, 2026
- Accepted:
- February 23, 2026
- Published Online:
- February 28, 2026
- Printed:
- March 1, 2026