
Evaluation of the association between systemic inflammatory indices and histopathological findings in high-risk HPV-positive women
Inflammatory indices in high-risk HPV
Authors
Abstract
Aim Human papillomavirus (HPV) infection is a necessary cause of cervical cancer; however, most women with high-risk HPV do not develop clinically significant cervical lesions. This study aimed to evaluate whether systemic inflammatory indices derived from routine complete blood counts are associated with early histopathological cervical lesions in high-risk HPV–positive women.
Methods This retrospective observational study included 277 women with high-risk HPV infection who underwent colposcopic examination and cervical biopsy. Histopathological findings were classified as negative (CIN0) or positive (CIN1+). Pre-colposcopy complete blood count parameters were used to calculate the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), systemic immune-inflammation index (SII), systemic inflammation response index (SIRI), and pan-immune-inflammation value (PIV). HPV genotypes and smoking status were recorded. Univariate and multivariable logistic regression analyses were performed to evaluate factors associated with histopathological positivity.
Results Of the participants, 221 (79.8%) had CIN0 and 56 (20.2%) had CIN1+ lesions. There were no significant differences between the groups in terms of age, smoking status, HPV genotypes, or systemic inflammatory indices. None of the inflammatory indices were associated with histopathological positivity in univariate analyses (all p > 0.05). In the multivariable model including age, smoking status, HPV16 positivity, and SII, no independent predictors of CIN1+ lesions were identified (all p > 0.05).
Conclusion The findings of this study indicate that systemic inflammatory indices are not independently associated with early histopathological cervical lesions in women with high-risk HPV infection, suggesting limited value of these markers for early lesion discrimination in this population.
Keywords
Introduction
Human papillomavirus (HPV) infection represents one of the leading causes of infection-related malignancies worldwide and is responsible for virtually all cases of cervical cancer, as well as a substantial proportion of other anogenital and head and neck cancers.1 Despite the implementation of preventive strategies such as organized cervical screening programs and HPV vaccination, HPV-associated diseases continue to pose a significant global health burden, particularly in low- and middle-income countries.1,2 Limitations related to vaccine coverage, genotype diversity, and disparities in healthcare access indicate that HPV-related cervical pathology remains a relevant clinical problem, underscoring the need for improved risk stratification strategies among HPV-positive women.2
Recent advances in histopathological classification have further highlighted the biological heterogeneity of HPV-associated cervical disease. The 2020 World Health Organization (WHO) classification introduced a paradigm shift by distinguishing HPV-associated and HPV-independent tumors of the female lower genital tract, emphasizing that HPV status reflects fundamental differences in tumor pathogenesis and prognosis.3 This histopathological distinction is supported by molecular evidence demonstrating that HPV-related cervical carcinogenesis is driven by complex interactions between persistent high-risk HPV infection, viral integration, and recurrent genomic alterations involving oncogenic signaling pathways and immune-related genes.4 Collectively, these findings suggest that cervical cancer and its precursor lesions represent biologically heterogeneous entities rather than a uniform disease process.
Accumulating evidence indicates that host immune response plays a pivotal role in determining the persistence, progression, or regression of HPV-associated cervical lesions. The clinical course of HPV infection varies according to HPV genotype and is strongly influenced by immune-mediated mechanisms.5 High-risk HPV types exhibit distinct carcinogenic behaviors, while dysregulation of both innate and adaptive immune responses facilitates viral persistence and disease progression.6 Furthermore, large-scale population-based studies have demonstrated that HPV infection is associated with a broad spectrum of cervical abnormalities, ranging from inflammatory changes to high-grade intraepithelial lesions and invasive carcinoma, reinforcing the close interplay between HPV infection, inflammation, and histopathological severity.7
In this context, increasing attention has been directed toward systemic inflammatory and hematologic indices derived from routine complete blood counts as potential biomarkers in HPV-associated cervical disease. Among these, the platelet-to-lymphocyte ratio (PLR) has been shown to independently predict recurrence or residual disease in patients with histopathologically confirmed high-grade squamous intraepithelial lesions following excisional treatment, suggesting a link between systemic inflammatory status and cervical lesion biology.8 In addition, other hematologic parameters reflecting platelet activation, such as mean platelet volume (MPV), have been associated with cervical cancer presence and disease stage, further supporting the relevance of systemic hematologic alterations in cervical carcinogenesis.9 However, despite growing evidence supporting the prognostic value of inflammatory indices, their association with baseline histopathological findings in high-risk HPV-positive women remains insufficiently explored. Therefore, the present study aimed to evaluate the association between systemic inflammatory indices and histopathological findings in women with high-risk HPV infection.
Materials and Methods
Study Design, Population, and Data CollectionThis retrospective observational study was conducted at a tertiary referral hospital in accordance with the principles of the Declaration of Helsinki. Ethical approval for the study was obtained from the institutional ethics committee, and all procedures were performed as part of routine clinical practice. Women who were found to be positive for high-risk HPV and subsequently underwent colposcopic examination with cervical biopsy during the study period were evaluated. Patients with available histopathological biopsy results and complete laboratory data obtained at the time of colposcopic evaluation were included in the study. Patients with a history of cervical cancer, those diagnosed with invasive cervical malignancy, and individuals with known systemic inflammatory or malignant diseases were excluded. Cases with incomplete clinical or laboratory data were also excluded from the analysis. Histopathological findings were classified according to cervical intraepithelial neoplasia (CIN) grading. For analytical purposes, benign histology (CIN0) was defined as histopathologically negative, whereas CIN grade 1 and above (CIN1+) was defined as histopathologically positive.
Laboratory Parameters, Inflammatory Indices, and Clinical VariablesComplete blood count parameters, including neutrophil, lymphocyte, monocyte, and platelet counts, were obtained from peripheral venous blood samples collected during routine clinical evaluation prior to colposcopic examination. All hematologic measurements were performed using the Beckman Coulter DxH 800 automated hematology analyzer in the hospital laboratory. Systemic inflammatory indices were calculated using parameters derived from the pre-colposcopy complete blood count, as follows: the neutrophil-to-lymphocyte ratio (NLR), PLR, monocyte-to-lymphocyte ratio (MLR), systemic immune-inflammation index (SII), systemic inflammation response index (SIRI), and pan-immune-inflammation value (PIV).
HPV genotypes were categorized as HPV16, HPV18, and other high-risk HPV types. In cases of multiple HPV infections, each genotype was recorded as a separate binary variable indicating its presence or absence. Smoking status was retrieved from medical records and categorized as active smoker or non-smoker (including never-smokers and former smokers) for statistical analysis.
Ethical ApprovalThis study was approved by the Ethics Committee of Gaziantep City Hospital (Date: 2025-12-17, No: 371/2025).
Statistical AnalysisStatistical analyses were performed using appropriate statistical software. Continuous variables were expressed as median and interquartile range (IQR), while categorical variables were presented as number and percentage. Comparisons between histopathologically negative and positive groups were performed using the Mann–Whitney U test for continuous variables and the chi-square test for categorical variables.
Univariate logistic regression analyses were conducted to evaluate the association between individual clinical, virological, and inflammatory variables and histopathological positivity. Variables with clinical relevance were subsequently included in a multivariable logistic regression model to identify factors independently associated with histopathological positivity. Among the inflammatory indices, the SII was selected for inclusion in the multivariable model because it reflects the combined effects of neutrophils, platelets, and lymphocytes and has been proposed as a comprehensive marker of systemic inflammatory status.
Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated, and a p-value < 0.05 was considered statistically significant.
Reporting GuidelinesThis study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Results
A total of 277 women with high-risk HPV infection who underwent colposcopic evaluation and cervical biopsy were included in the study. Based on histopathological examination, 221 patients were classified as histopathologically negative (CIN0), whereas 56 patients were classified as histopathologically positive (CIN1+).
The comparison of demographic characteristics, HPV genotypes, and systemic inflammatory indices between histopathologically negative (CIN0) and positive (CIN1+) groups is summarized in Table 1. There were no statistically significant differences between the two groups in terms of age, smoking status, HPV16 positivity, HPV18 positivity, or the presence of other high-risk HPV genotypes (all p > 0.05). Similarly, none of the evaluated inflammatory indices—NLR, PLR, MLR, SII, SIRI, and PIV—differed significantly between the groups (all p > 0.05).
Univariate logistic regression analyses were performed to evaluate the associations between clinical characteristics, HPV genotypes, inflammatory indices, and histopathological positivity (CIN1+). As presented in Table 2, age, smoking status, HPV genotypes, and all assessed inflammatory indices (NLR, PLR, MLR, SII, SIRI, and PIV) were not significantly associated with histopathological positivity in univariate analyses (all p > 0.05). Subsequently, a multivariable logistic regression model including age, smoking status, HPV16 positivity, and SII was constructed to identify factors independently associated with histopathological positivity. As shown in Table 2, none of these variables demonstrated an independent association with histopathological positivity (all p > 0.05).
Discussion
In the present study, we evaluated the relationship between systemic inflammatory indices and histopathological findings in women with high-risk HPV infection. Our analyses demonstrated that commonly used systemic inflammatory markers, including NLR, PLR, MLR, SII, SIRI, and PIV, were not independently associated with histopathological positivity defined as CIN1+. Although some indices showed numerically higher values among histopathologically positive cases, these differences did not reach statistical significance in either univariate or multivariable analyses. These findings suggest that systemic inflammatory responses may not yet be sufficiently pronounced in early cervical pathology to reliably discriminate between histopathologically negative lesions and CIN1+ findings.
Previous studies have suggested a potential role for systemic inflammatory and hematologic indices in the clinical course of HPV-related cervical disease, particularly in the context of high-grade lesions, invasive cancer, or disease persistence. For instance, Huang et al. reported that elevated PLR values were associated with recurrence or residual disease following excisional treatment in patients with High-Grade Squamous Intraepithelial Lesion (HSIL), indicating a prognostic relevance of systemic inflammation in advanced precancerous disease.8 Similarly, Shen et al. demonstrated that mean platelet volume was associated with the presence and stage of cervical cancer, supporting the notion that systemic hematologic alterations are more evident in invasive disease rather than in early lesions.9 Collectively, these observations imply that the clinical utility of systemic inflammatory indices may vary according to disease stage and underlying biological behavior.
Consistent with our findings, several recent studies examining lesion severity and diagnostic performance have reported the limited utility of systemic inflammatory indices in distinguishing cervical lesions. In a large retrospective cohort, Alci et al. showed that inflammatory indices such as NLR, PLR, MLR, SII, and SIRI were not independently associated with CIN2+ lesions, whereas age and HPV16 positivity emerged as more relevant factors.10 Likewise, Qin and Zhang found that although certain inflammatory markers were numerically higher in patients with cervical lesions, their overall diagnostic performance was limited, with low discriminatory capacity based on receiver operating characteristic (ROC) analyses.11 In line with these reports, none of the evaluated systemic inflammatory indices in our study were significantly associated with histopathological positivity, even when modest numerical differences were observed. Supporting this perspective, Lei et al. demonstrated that the risk of occult invasive cancer in patients with biopsy-proven HSIL was primarily related to local clinicopathological features—such as HPV16/18 positivity, lesion extent, glandular involvement, and cytological severity—rather than systemic inflammatory markers.12 Together, these findings suggest that systemic inflammatory indices alone may not provide sufficient diagnostic discrimination, particularly in populations encompassing early-stage or biologically heterogeneous cervical lesions.
Other investigations have proposed that systemic inflammatory indices may be more informative in selected high-risk populations or in the presence of invasive disease. Cim et al. reported heterogeneous alterations in inflammatory parameters across different cervical pathology subgroups, with more pronounced changes observed in HSIL, although without consistent predictive performance across the entire disease spectrum.13 Similarly, Keszthelyi et al. demonstrated that SII and SIRI exhibited high negative predictive values for excluding invasive cervical carcinoma, highlighting their potential role as adjunctive markers in advanced disease rather than as tools for identifying early histopathological changes.14 Studies conducted in conization cohorts have also reported moderate diagnostic performance of NLR or PLR for detecting invasive carcinoma, particularly in clinically selected or high-risk populations.15,16
Beyond diagnostic applications, accumulating evidence indicates that systemic inflammatory indices may have greater relevance in prognostic and therapeutic contexts. Elevated NLR, PLR, or MLR values have been associated with recurrence risk, survival outcomes, and treatment response in patients with high-grade lesions or invasive cervical cancer undergoing excisional procedures or chemoradiotherapy.17,18,19 In this regard, Li et al. demonstrated that increased NLR and MLR were independently associated with poorer survival outcomes and higher recurrence risk in patients with stage IIB cervical cancer, further supporting the relevance of systemic inflammatory indices in advanced-stage disease rather than in early histopathological differentiation.20 These findings suggest that systemic inflammation may primarily reflect disease burden and tumor–host interactions, rather than serving as a sensitive marker for early lesion detection.
Limitations
The present study has several limitations. First, the definition of histopathological positivity as CIN1 and above encompasses a biologically heterogeneous spectrum, including lesions with high rates of spontaneous regression, which may attenuate potential associations with systemic inflammatory markers. Second, the retrospective and single-center design may limit the generalizability of the findings. Additionally, the cross-sectional nature of the analysis and the assessment of inflammatory indices at a single pre-colposcopy time point preclude evaluation of temporal changes, lesion persistence, or progression. Third, differences in disease stage, clinical setting, and patient selection compared with prior studies focusing on high-grade lesions or invasive cancer may partly account for variability across the literature. Finally, local cervical immune responses and microenvironmental factors—which are not captured by peripheral blood indices—may play a more prominent role in the early development of HPV-related cervical lesions.
Taken together, these findings suggest that systemic inflammatory indices may be more reflective of overall immune–inflammatory status and disease burden rather than sensitive markers for early histopathological differentiation in high-risk HPV–positive women. In early and biologically heterogeneous cervical lesions, local immune responses and microenvironmental factors—rather than peripheral blood–based markers—may play a more prominent role in determining histopathological outcomes. This perspective highlights the importance of interpreting systemic inflammatory indices within the broader clinical and biological context of HPV-related cervical disease.
Conclusion
In conclusion, this study found no independent association between commonly used systemic inflammatory indices and histopathological positivity in women with high-risk HPV infection. These findings suggest that peripheral blood–based inflammatory markers alone may have limited utility for distinguishing early cervical lesions. Further prospective, multicenter studies incorporating longitudinal follow-up and integrated clinical, virological, and molecular parameters are warranted to better define the role of systemic inflammation in cervical disease risk stratification.
Declarations
Ethics Declarations
This study was approved by the Ethics Committee of Gaziantep City Hospital (Date: 2025-12-17, No: 371/2025).
Animal and Human Rights Statement
All procedures performed in this retrospective study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Due to the retrospective design of the study, the requirement for informed consent was waived by the ethics committee.
Informed Consent
The requirement for informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: İ.T.
Study Design: İ.T.
Data Collection: İ.T., E.Ş.
Data Analysis and Interpretation: İ.T., E.Ş.
Statistical Analysis: İ.T.
Writing – Original Draft Preparation: İ.T.
Writing – Review & Editing: İ.T., E.Ş.
Supervision: İ.T.
Final Approval of the Manuscript: All authors.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content, including study design, data collection, analysis and interpretation, writing, and approval of the final version of the article.
Abbreviations
HPV: Human papillomavirus
WHO: World Health Organization
CIN: Cervical intraepithelial neoplasia
NLR: Neutrophil-to-lymphocyte ratio
PLR: Platelet-to-lymphocyte ratio
MLR: Monocyte-to-lymphocyte ratio
SII: Systemic immune-inflammation index
SIRI: Systemic inflammation response index
PIV: Pan-immune-inflammation value
MPV: Mean platelet volume
IQR: Interquartile range
OR: Odds ratio
CI: Confidence interval
ROC: Receiver operating characteristic
References
-
Serrano B, Brotons M, Bosch FX, Bruni L. Epidemiology and burden of HPV-related disease. Best Pract Res Clin Obstet Gynaecol. 2018;47:14-26. doi:10.1016/j.bpobgyn.2017.08.006
-
Kombe Kombe AJ, Li B, Zahid A, et al. Epidemiology and burden of human papillomavirus and related diseases, molecular pathogenesis, and vaccine evaluation. Front Public Health. 2021;8:552028. doi:10.3389/fpubh.2020.552028
-
Höhn AK, Brambs CE, Hiller GGR, May D, Schmoeckel E, Horn LC. 2020 WHO classification of female genital tumors. Geburtshilfe Frauenheilkd. 2021;81(10):1145-1153. doi:10.1055/a-1545-4279
-
Ojesina AI, Lichtenstein L, Freeman SS, et al. Landscape of genomic alterations in cervical carcinomas. Nature. 2014;506(7488):371-375. doi:10.1038/nature12881
-
Kusakabe M, Taguchi A, Sone K, Mori M, Osuga Y. Carcinogenesis and management of human papillomavirus-associated cervical cancer. Int J Clin Oncol. 2023;28(8):965-974. doi:10.1007/s10147-023-02337-7
-
Gu Y, Li T, Zhang M, et al. The display between HPV infection and host immunity in cervical cancer. Front Biosci (Landmark Ed). 2024;29(12):426. doi:10.31083/j.fbl2912426
-
Lin K, Hong Q, Fu Y, et al. Cervical HPV infection and related diseases among 149,559 women in Fujian: an epidemiological study from 2018 to 2023. Front Microbiol. 2024;15:1418218. doi:10.3389/fmicb.2024.1418218
-
Huang G, Gao H, Chen Y, et al. Platelet-to-lymphocyte ratio as the prognostic factor for recurrence/residual disease in HSIL patients after LEEP. J Inflamm Res. 2023;16:1923-1936. doi:10.2147/JIR.S406082
-
Shen WJ, Fu S, Li N, et al. Decreased mean platelet volume is associated with cervical cancer development. Asian Pac J Cancer Prev. 2017;18(7):1769-1772.
-
Alci A, Yalcin N, Gokkaya M, et al. The relationship between peripheral inflammatory markers and high-grade cervical lesions: a retrospective cohort study. Diagnostics (Basel). 2025;15(16):2107. doi:10.3390/diagnostics15162107
-
Qin L, Zhang L. The predictive value of serum inflammatory markers for the severity of cervical lesions. BMC Cancer. 2024;24(1):780. doi:10.1186/s12885-024-12561-7
-
Lei L, Zhang L, Zheng Y, et al. Clinical analysis of 314 patients with high-grade squamous intraepithelial lesion who underwent total hysterectomy directly: a multicenter, retrospective cohort study. BMC Cancer. 2024;24(1):575. doi:10.1186/s12885-024-12342-2
-
Cim N, Ayguler E, Gunal N, Cim B, Atalmis HA, Cetin A. Systemic inflammatory response index in cervical pathologies (human papillomavirus and cervical neoplasia) and its prognostic value in disease prediction. Niger J Clin Pract. 2025;28(5):615-623. doi:10.4103/njcp.njcp_581_24
-
Keszthelyi M, Sziva RE, Havrán Z, et al. Systemic inflammatory indices—systemic immune-inflammation index (SII) and the systemic inflammation response index (SIRI)—as potential rule-out biomarkers for invasive cervical carcinoma. Int J Mol Sci. 2025;27(1):435. doi:10.3390/ijms27010435
-
Vida B, Keszthelyi E, Tóth Z, et al. The neutrophil-to-lymphocyte ratio as a potential predictor in conization outcomes for cervical cancer. Cancers (Basel). 2025;17(11):1856. doi:10.3390/cancers17111856
-
Kalas N, Szabó V, Vida B, et al. The platelet-to-lymphocyte ratio as a non-invasive biomarker for cervical malignancy in conization patients. Life (Basel). 2025;15(6):971. doi:10.3390/life15060971
-
Zhai F, Mu S, Song Y, Zhang M, Zhang C, Lv Z. Associations between preoperative inflammatory indices and residual or recurrent cervical intraepithelial neoplasia post loop electrosurgical excision procedure. J Inflamm Res. 2024;17:8741-8751. doi:10.2147/JIR.S485698
-
Yu J, Huang L, Dong T, Cao L. Prediction of outcomes after chemoradiotherapy for cervical cancer by neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio. J Obstet Gynaecol. 2024;44(1):2361858. doi:10.1080/01443615.2024.2361858
-
Wang L, Dong Y. Peripheral blood immune cell parameters in patients with high-grade squamous intraepithelial lesion (HSIL) and cervical cancer and their clinical value: a retrospective study. PeerJ. 2024;12:e17499. doi:10.7717/peerj.17499
-
Li YX, Chang JY, He MY, et al. Neutrophil-to-lymphocyte ratio and monocyte-to-lymphocyte ratio predict clinical outcome in patients with stage IIB cervical cancer. J Oncol. 2021;2021:2939162. doi:10.1155/2021/2939162
Tables
Table 1. Comparison of clinical characteristics and inflammatory indices between histopathologically negative (CIN0) and positive (CIN1 and Above) cases
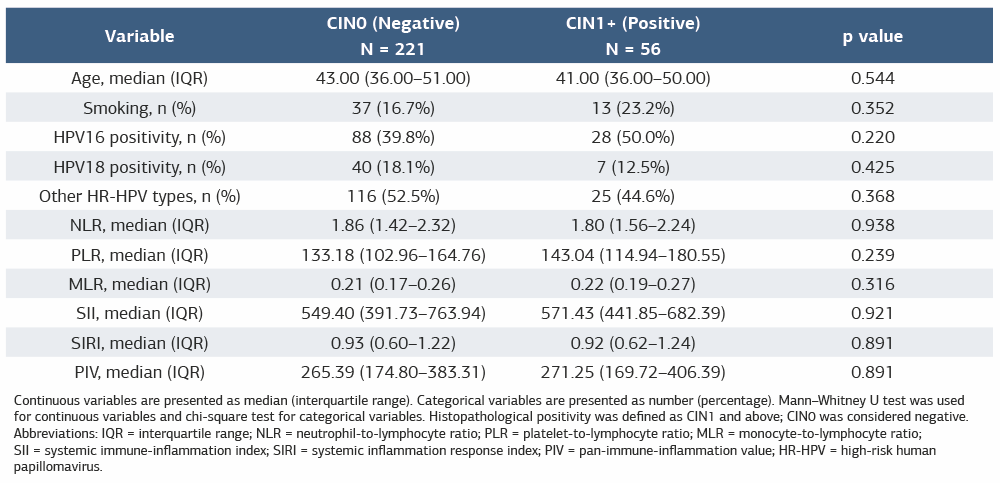
Continuous variables are presented as median (interquartile range). Categorical variables are presented as number (percentage). Mann–Whitney U test was used for continuous variables and chi-square test for categorical variables. Histopathological positivity was defined as CIN1 and above; CIN0 was considered negative. Abbreviations: IQR = interquartile range; NLR = neutrophil-to-lymphocyte ratio; PLR = platelet-to-lymphocyte ratio; MLR = monocyte-to-lymphocyte ratio; SII = systemic immune-inflammation index; SIRI = systemic inflammation response index; PIV = pan-immune-inflammation value; HR-HPV = high-risk human papillomavirus.
Table 2. Univariate and multivariable logistic regression analyses for histopathological positivity (CIN1+)
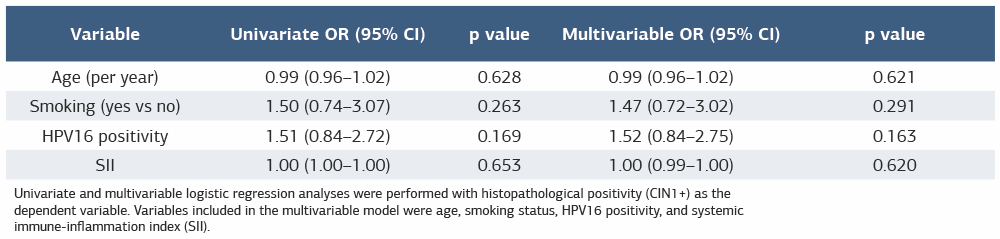
Univariate and multivariable logistic regression analyses were performed with histopathological positivity (CIN1+) as the dependent variable. Variables included in the multivariable model were age, smoking status, HPV16 positivity, and systemic immune-inflammation index (SII).
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
İbrahim Taşkum, Erkan Şimşek. Evaluation of the association between systemic inflammatory indices and histopathological findings in high-risk HPV-positive women. Ann Clin Anal Med 2026;17(3):249-253
- Received:
- January 16, 2026
- Accepted:
- February 23, 2026
- Published Online:
- February 28, 2026
- Printed:
- March 1, 2026