
Analysis of short-term outcomes of laparoscopic versus open right hemicolectomy for right colon cancer in patients aged 65 years and older
Lap vs open RH in elderly patients
Authors
Abstract
Aim This study compared early postoperative outcomes between laparoscopic right hemicolectomy (including extended resections) and open right hemicolectomy in patients aged 65 years and older with right-sided colon adenocarcinoma.
Methods This retrospective cohort study included patients aged 65 years and older who underwent elective surgery for right-sided colon adenocarcinoma between 2018 and 2024. Patients were analyzed by the completed approach: laparoscopic versus open. The primary endpoint was 30-day overall postoperative complications categorized by type and severity using the Clavien–Dindo classification.
Results A total of 139 patients were included: 48 (34.5%) laparoscopic and 91 (65.5%) open cases. Operative time was longer in the laparoscopic group (median 274 vs 205 minutes, p < 0.001), while length of stay was similar (median 8 days, p = 0.953). Overall, 30-day postoperative complications were significantly less frequent in the laparoscopic group (10.4% vs 30.8%, p = 0.007), primarily due to fewer wound infections (2 vs 14). Major complications (Clavien–Dindo ≥ IIIA) were numerically lower after laparoscopy (6% vs 14%, p = 0.158). In-hospital mortality occurred only in the open group (2% vs 0%, p = 0.545).
Conclusion Laparoscopic right hemicolectomy is safe and effective for selected patients aged 65 years and older. It offers lower 30-day morbidity despite longer operative time, while maintaining staging adequacy and similar recovery duration.
Keywords
Introduction
Colorectal cancer persists as a significant global health concern, representing one of the most prevalent types of cancer on a worldwide scale. The global burden of disease is predominantly observed in older adults, in whom the presence of comorbidity and reduced physiological reserve has been demonstrated to increase perioperative risk and complicate recovery following major abdominal surgery.1
The treatment of choice for localised right-sided colon cancer is curative resection, accompanied by adequate lymphadenectomy. The prevailing contemporary guidelines advocate for minimally invasive colectomy in select patients, provided that specific criteria are met. These criteria include the maintenance of oncological principles and the execution of the procedure by experienced teams.2,3
In elderly patients, the possible advantages of laparoscopy (decreased surgical trauma and accelerated recovery) should be weighed against the patient's physical weakness and the complexity of the procedure. Evidence focusing specifically on elderly patients undergoing right hemicolectomy demonstrates that laparoscopic right hemicolectomy can be performed safely with favourable short-term outcomes when compared with open surgery, although selection bias and conversion to open surgery remain important considerations.4,5
To reduce heterogeneity introduced by left-sided and rectal procedures with different technical demands and complication profiles, the present analysis was focused on right-sided resections.
The objective of this study was to make a comparison between the early postoperative outcomes of patients who underwent laparoscopic right hemicolectomy (including extended right hemicolectomy) for right-sided colon adenocarcinoma, and those who underwent open right hemicolectomy, in patients aged 65 years and older, treated between January 2018 and December 2024.
Materials and Methods
This retrospective cohort study was conducted at the Department of General Surgery, Izmir Tepecik Training and Research Hospital (Izmir, Türkiye). Patients aged 65 years and older who underwent elective surgery for right-sided colon adenocarcinoma between January 2018 and December 2024 were retrospectively reviewed.
Eligible patients were 65 years and older at the time of surgery and underwent elective right hemicolectomy (including extended right hemicolectomy) for histologically confirmed adenocarcinoma located in the cecum, ascending colon, hepatic flexure, or proximal transverse colon. An extended right hemicolectomy was defined as a right colectomy with resection extending into the transverse colon for hepatic flexure or proximal transverse tumors. Patients were excluded if surgery was performed for benign pathology, if surgery was emergent, if key perioperative or 30-day outcome data were missing, or if conversion from laparoscopic to open surgery occurred. Patients were analyzed according to the completed operative approach: laparoscopic versus open.
Data were extracted from electronic medical records, anesthesia charts, operative reports, inpatient notes, and pathology reports. Preoperative variables included age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status, Charlson Comorbidity Index (CCI),6 and tumor markers (carcinoembryonic antigen (CEA) and carbohydrate antigen (CA) 19-9). Perioperative variables included operative time, perioperative blood transfusion, synchronous metastasectomy, anastomotic leak, length of hospital stay, and in-hospital mortality. Pathological variables included T/N/M stage according to the American Joint Committee on Cancer (AJCC) 8th edition7 and harvested lymph node count.
The primary endpoint was a 30-day overall postoperative complication, defined as the occurrence of any complication within 30 days after surgery. Postoperative complications were recorded and categorized by type (wound infection, bleeding, cardiac failure, pulmonary embolism, fever, anastomotic leak, ileus). Complication severity was graded using the Clavien–Dindo classification; major complications were defined as grade ≥ IIIA.8
Ethical ApprovalThis study was approved by the Ethics Committee of Izmir Tepecik Training and Research Hospital (Date: 2026-01-05, No: 2025/12-29).
Statistical AnalysisStatistical analyses were performed using SPSS version 28.0 (IBM Corp., Chicago, IL, USA). Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range [IQR]), as appropriate, and compared using Student’s t-test or Mann–Whitney U test. Categorical variables are presented as counts and percentages and compared using the χ² test or Fisher’s exact test. Univariable logistic regression was performed to identify factors associated with major postoperative complications (Clavien–Dindo ≥IIIA). A two-sided p-value < 0.05 was considered statistically significant.
Reporting GuidelinesThis study is reported in accordance with the STROBE guidelines.
Results
A total of 139 patients were included: 48 (34.5%) underwent laparoscopic surgery, and 91 (65.5%) underwent open surgery. Sex distribution was comparable between groups (male: 60% vs 64%, p = 0.975). Median age was lower in the laparoscopic group (70.5 [IQR 10.8] vs 76 [IQR 10] years, p = 0.018). BMI, ASA class, CCI, and preoperative tumor markers (CEA and CA 19-9) were similar between groups (Table 1). The detailed data are provided in Supplementary Table 1.
Anastomotic leak rates were low and similar in both groups (4% vs 4%, p = 0.950). The open group had a higher transfusion rate (31% vs 19%), although this difference did not reach statistical significance (p = 0.127). Operative time was longer in the laparoscopic group (median 274 [IQR 115] vs 205 [IQR 55] minutes, p < 0.001), while length of stay (LOS) was similar (median 8 days in both groups, p = 0.953). In-hospital mortality occurred only in the open group (2% vs 0%, p=0.545). Pathological T-stage distribution differed significantly between groups (p = 0.001), with a higher proportion of T4 tumors in the open group. N-stage and M-stage distributions were similar. Harvested lymph node count was lower in the laparoscopic group (median 17 [IQR 13] vs 24 [IQR 12], p = 0.009) (Table 1). The detailed data are provided in Supplementary Table 2.
Overall, 30-day postoperative complications were significantly less frequent in the laparoscopic group compared with the open group (5/48 vs 28/91, p = 0.007), mainly driven by fewer wound infections (2 vs 14). Other complications (bleeding, cardiac failure, pulmonary embolism, fever, anastomotic leak, and ileus) were numerically more frequent in the open group.
Major complications (Clavien–Dindo ≥IIIA) occurred in 3 laparoscopic and 13 open cases. Although major complications were numerically less frequent after laparoscopy (6% vs 14%), the difference did not reach statistical significance (p = 0.158).
In univariable logistic regression analysis, perioperative blood transfusion was associated with major complications (odds ratio (OR) 3.241; 95% confidence interval (CI) 1.118–9.400; p = 0.030). No other evaluated variable, including operative approach, was significantly associated with major complications (all p > 0.05) (Table 1). The detailed data are provided in Supplementary Table 3.
Discussion
In this single-centre retrospective cohort study of patients aged 65 years and older who underwent elective right or extended right hemicolectomy for colon adenocarcinoma, a completed-approach analysis (excluding conversions) revealed a reduced 30-day overall complication rate following laparoscopic surgery in comparison with open surgery. This finding is consistent with recent real-world registry data, which indicate favourable short-term outcomes following laparoscopic colon cancer resection in routine clinical practice.3,4 In the present cohort, major morbidity and early mortality were comparable between the two approaches, suggesting that the observed advantage of laparoscopy was primarily driven by a reduced incidence of minor to moderate postoperative morbidity, as opposed to severe complications.
The decision to focus specifically on geriatric patients undergoing right-sided resections was intentional. Colorectal cancer risk increases markedly with age,9 and right-sided colon cancers become proportionally more frequent in older age groups. This makes right hemicolectomy a key procedure in geriatric surgical practice.10,11 Right-sided colectomy differs substantially from left-sided colectomy and anterior resection in terms of vascular control, mesocolic dissection planes, anastomotic configuration, and procedure-specific complication profiles. Including left-sided and rectal procedures would introduce marked heterogeneity (e.g., pelvic dissection, low anastomosis, diverting stomas), which could confound early outcome comparisons. Restricting the analysis to right-sided colectomies is the only way to improve internal validity and interpretability.
Baseline risk assessment is vital in surgical care of the elderly. Our dataset clearly shows that the ASA class and CCI distributions were similar between groups, and BMI was also comparable. This definitely demonstrates comparability with respect to recorded comorbidity burden and body habitus. However, it is important to note that ASA and CCI may not fully capture geriatric vulnerability. Contemporary perioperative guidance highlights that frailty and functional reserve, which are often not documented in retrospective datasets, are major determinants of complications, delirium, prolonged recovery, and loss of independence8,9 Therefore, despite similar ASA/CCI/BMI, unmeasured factors such as frailty, sarcopenia, or functional dependence can influence both approach selection and postoperative outcomes.
The reduction in overall morbidity observed in older adults following laparoscopy is of significant clinical importance, given the propensity of even minor complications to result in further adverse outcomes and protracted return to baseline. The diminished wound-related morbidity observed is undoubtedly a primary contributing factor, given the reduced incision size and diminished tissue trauma associated with minimally invasive surgical interventions. It is noticeable that the length of stay between the two groups was comparable. This is indicative of the increasing standardisation of perioperative care, including Enhanced Recovery After Surgery (ERAS) pathways. These pathways have been shown to optimise analgesia, mobilisation, and early feeding, irrespective of incision type, thereby reducing LOS differences between operative approaches.2 In geriatric patients, discharge timing is also strongly influenced by social support, rehabilitation needs, and stabilisation of comorbid conditions. These factors are considered to be of greater significance than any minor discrepancies in surgical stress.
Operative time was longer in the laparoscopic group. This was probably due to the technical demands of central vascular ligation and intracorporeal dissection.3,4 Importantly, there was no increased major morbidity or early mortality, suggesting that laparoscopy can be used safely in older, appropriately selected patients and in experienced surgeons. However, prolonged anesthesia time may be of particular significance in geriatric practice, given the potential consequences of hypothermia, fluid shifts, and cardiopulmonary stress. This underscores the importance of meticulous perioperative optimization, encompassing geriatric-focused perioperative care and adherence to the ERAS protocol.2,8
An important observation was that the laparoscopic group had a lower number of lymph nodes. Guidelines for diagnosing colon cancer recommend examining at least 12 lymph nodes.3 Poorly evaluated lymph nodes are linked to a poor prognosis. In our series, lymph node counts remained higher than the commonly used threshold, reassuring for staging quality. But lymph node yield is multifaceted and can vary due to tumor characteristics, specimen complexity, and surgical technique. The open cohort had more pT4 tumors, possibly leading to more extensive surgery and retrieval of more tissue, increasing yield. This suggests the difference is due to the case mix and is not due to laparoscopy itself, as emerging data shows that optimal thresholds may vary by tumor type and stage.7
The higher pT4 rate in the open group suggests that tumors may be assigned to open surgery because of anticipated complexity or the need for multivisceral resection. Laparoscopy can be feasible for selected T4 disease, but caution is advised for suspected right-sided T4b tumors.12 This imbalance should be considered when interpreting the morbidity advantage of laparoscopy in our completed approach comparison.
In this study, conversions were excluded in order to preserve a completed‑approach comparison; however, it should be noted that conversion is a clinically meaningful real‑world event. Recent multinational data demonstrate that conversion during minimally invasive right colectomy for cancer is associated with worse postoperative outcomes in comparison with successfully completed minimally invasive surgery.5 Therefore, excluding converted cases may result in an overestimation of the benefit of laparoscopy. Conversion should not be interpreted as a failure; timely conversion is often a safety strategy when intraoperative findings exceed minimally invasive feasibility.
Limitations
The study's retrospective design is a limitation, as it is susceptible to selection bias and residual confounding. Despite the comparable findings between the ASA, CCI, and BMI groups, there was an absence of systematic recording of frailty and functional status. These factors have the potential to influence both approach selection and postoperative outcomes in older patients. The higher pT4 proportion observed in the open cohort suggests case-mix differences, which may partly explain the observed morbidity and lymph node yield patterns. Additionally, conversions from laparoscopy to open surgery were excluded, resulting in a completed-approach comparison rather than an intention-to-treat analysis. As conversion is linked to elevated postoperative morbidity, this exclusion may potentially introduce bias in the observed effect, favouring laparoscopy. Additionally, this is a single-centre experience; the extent to which institutional ERAS adoption, surgeon experience, and pathology processing may influence generalisability is a potential limitation.
Conclusion
Laparoscopic right or extended right hemicolectomy is safe and effective for selected patients aged 65 years and older. It offers lower 30-day morbidity but longer operative time, similar LOS, and preserves staging adequacy. Incorporating standardised frailty assessment and reporting both completed-approach and intention-to-treat analyses will strengthen future evidence and help refine patient selection in geriatric colon cancer surgery.
Declarations
Ethics Declarations
The study was approved by the Ethics Committee of Izmir Tepecik Training and Research Hospital (Date: 2026-01-05, No: 2025/12-29).
Animal and Human Rights Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
The requirement for informed consent was waived due to the retrospective design of the study.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: O.B.N., S.Y.
Methodology: O.B.N., S.Y.
Formal Analysis: O.B.N.
Investigation: O.B.N., H.Y., O.A.
Data Curation: O.B.N., H.Y., O.A.
Writing – Original Draft Preparation: O.B.N.
Writing – Review & Editing: H.Y., O.A., S.Y.
Supervision: S.Y.
Scientific Responsibility Statement
The authors declare that they are responsible for the article’s scientific content including study design, data collection, analysis and interpretation, writing, some of the main line, or all of the preparation and scientific review of the contents and approval of the final version of the article.
Abbreviations
AJCC: American Joint Committee on Cancer
ASA: American Society of Anesthesiologists
BMI: body mass index
CA 19-9: carbohydrate antigen 19-9
CCI: Charlson Comorbidity Index
CEA: carcinoembryonic antigen
CI: confidence interval
ERAS: Enhanced Recovery After Surgery
IQR: interquartile range
LOS: length of stay
OR: odds ratio
SD: standard deviation
References
-
Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263. doi:10.3322/caac.21834
-
Argilés G, Tabernero J, Labianca R, et al. Localised colon cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31(10):1291-1305. doi:10.1016/j.annonc.2020.06.022
-
Vogel JD, Felder SI, Bhama AR, et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the management of colon cancer. Dis Colon Rectum. 2022;65(2):148-177. doi:10.1097/DCR.0000000000002323
-
Quyn AJ, Moussa O, Millar F, Smith DM, Steele RJ. Open versus laparoscopic right hemicolectomy in the elderly population. World J Gastrointest Surg. 2013;5(6):187-191. doi:10.4240/wjgs.v5.i6.187
-
Luo W, Wu M, Chen Y. Laparoscopic versus open surgery for elderly patients with colorectal cancer: a systematic review and meta-analysis of matched studies. ANZ J Surg. 2022;92(9):2003-2017. doi:10.1111/ans.17972
-
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373-383. doi:10.1016/0021-9681(87)90171-8
-
Amin MB, Edge S, Greene F, et al., eds. AJCC cancer staging manual. 8th ed. Springer; 2017.
-
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205-213. doi:10.1097/01.sla.0000133083.54934.ae
-
Reif de Paula T, Simon HL, Profeta da Luz MM, Keller DS. Right sided colorectal cancer increases with age and screening should be tailored to reflect this: a national cancer database study. Tech Coloproctol. 2021;25(1):81-89. doi:10.1007/s10151-020-02329-z
-
Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233-254. doi:10.3322/caac.21772
-
Morgan E, Arnold M, Gini A, et al. Global burden of colorectal cancer in 2020 and 2040: incidence and mortality estimates from GLOBOCAN. Gut. 2023;72(2):338-344. doi:10.1136/gutjnl-2022-327736
-
You K, Park HC, Park SC, et al. Laparoscopic approach for T4 colon cancer can be associated with poor prognosis in right-sided T4b tumours. Eur J Surg Oncol. 2021;47(7):1645-1650. doi:10.1016/j.ejso.2021.01.009
Tables
Table 1. Summary of baseline characteristics, key outcomes, and predictors of complications
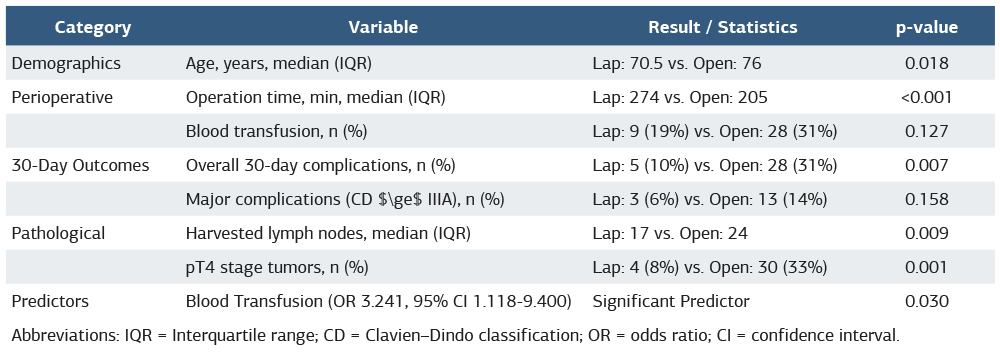
Abbreviations: IQR = Interquartile range; CD = Clavien–Dindo classification; OR = odds ratio; CI = confidence interval.
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Ozan Barış Namdaroğlu, Hilmi Yazıcı, Olcay Atbaş,Savaş Yakan. Analysis of short-term outcomes of laparoscopic versus open right hemicolectomy for right colon cancer in patients aged 65 years and older. Ann Clin Anal Med 2026;17(3): 254-258
- Received:
- January 21, 2026
- Accepted:
- February 23, 2026
- Published Online:
- February 28, 2026