
Disseminated cytomegalovirus infection in a newly diagnosed HIV-positivepatient: A Case Report
Disseminated cytomegalovirus infection and AIDS
Authors
Abstract
Introduction Cytomegalovirus (CMV) remains latent in about half of adults and may reactivate in immunocompromised individuals. In advanced HIV infection, CMV can cause systemic disease with end-organ involvement.
Case Presentation A 34-year-old woman with newly diagnosed HIV who had recently started antiretroviral therapy (ART) was referred to our clinic after five days of fever, cough, diarrhea, and ulcerative skin lesions unresponsive to antibiotics. She was hypoxemic and cachectic, with bilateral infiltrates on chest radiography. CMV IgG was positive, IgM was negative, and CMV DNA was detected at 1100 IU/mL. Skin biopsy showed plasma cell–rich dermal inflammation, consistent with disseminated CMV infection involving the lungs, colon, and skin. Intravenous ganciclovir, combined with ongoing ART, led to rapid improvement. After three months, CMV DNA and HIV RNA were undetectable; symptoms had resolved.
Conclusion Disseminated CMV infection should be suspected in newly diagnosed HIV patients during early ART who present with unexplained fever and refractory mucocutaneous lesions.
Keywords
Introduction
Cytomegalovirus (CMV), a member of the Herpesviridae family, exists as a latent infection in approximately 50% of the adult population worldwide.1 In the setting of immunosuppression, the virus can become reactivated and disseminate hematogenously to target organs.1,2 During widespread infection, CMV may be detected in various tissues and cell types, which can serve as evidence of systemic dissemination.3 CMV-related end-organ diseases are most commonly observed when the CD4+ T lymphocyte count falls below 50 cells/mm3.4 In patients with acquired immunodeficiency syndrome (AIDS), end-organ involvement may include retinitis, colitis, esophagitis, hepatitis, encephalitis, and pneumonia. In the present case, we report a disseminated CMV infection in a newly diagnosed HIV-positive patient, presenting with pneumonia, colitis, and cutaneous manifestations.
Case Presentation
A 34-year-old woman with no known comorbidities was admitted to our clinic with a high-grade fever (>38°C) persisting for five days while being followed at another center for newly diagnosed HIV infection. The patient reported a history of suspected heterosexual contact two years prior. At the time of diagnosis, her HIV Ribonucleic acid (RNA) level was 1,300,000 copies/mL, and her CD4+ T lymphocyte count was 48 cells/mm³. She had been initiated on antiretroviral therapy (ART) consisting of tenofovir disoproxil fumarate, emtricitabine, and dolutegravir, along with prophylactic treatment for opportunistic infections, including trimethoprim-sulfamethoxazole and azithromycin.
Upon admission to our clinic, on day 15 of ART and prophylaxis, she presented with a one-week history of cough, sputum production, and watery diarrhea (3–4 times daily). On physical examination, the patient appeared cachectic and in poor general condition, with a body temperature of 38.3°C, pulse rate of 94 bpm, blood pressure of 110 / 50 mmHg, respiratory rate of 30/min, and oxygen saturation of 75% on room air, which improved to 90% with 6 L/min supplemental oxygen. Auscultation revealed bilateral fine crackles. Dermatological examination revealed a non-infected, eroded wound measuring 6x5 cm near the anus in the right gluteal region and an erythematous, eroded lesion surrounding the distal phalanx of the third finger on the right hand. Other systemic examinations were unremarkable.
Further anamnesis revealed that the skin lesions had been present for approximately one month and had not responded to topical treatments. Posteroanterior chest radiography revealed diffuse bilateral opacities (Figure 1). Despite receiving broad-spectrum antibiotics, including meropenem, linezolid, and tigecycline for one week at the external center, the patient’s fever persisted. Given the clinical presentation and immunosuppressed status, empirical therapy with liposomal amphotericin B (3 mg/kg/day), ganciclovir (5 mg/kg twice daily), moxifloxacin (400 mg/day), and dexamethasone (6 mg/day) was initiated.
Investigations into the etiology of fever, including transthoracic echocardiography, abdominal ultrasonography, and contrast-enhanced cranial magnetic resonance imaging (MRI), revealed no abnormalities. Laboratory tests showed negative SARS-CoV-2 polymerase chain reaction (PCR), negative serial serum galactomannan, negative cryptococcal antigen, negative Giemsa stain in sputum, and a tuberculin skin test (PPD) result of 0 mm. Blood cultures were negative. CMV serology revealed IgM negativity and IgG positivity; cytomegalovirus (CMV) deoxyribonucleic acid (DNA) was detected at 1,100 IU/L (Table 1). Ophthalmologic examination did not reveal signs of retinitis.
Skin biopsy from the lesions showed a dermal inflammatory infiltrate rich in plasma cells, extending from the superficial dermis into the reticular dermis. In light of the patient’s immunosuppression, pneumonia, colitis, and cutaneous findings, disseminated CMV disease was considered the most likely diagnosis. By day 18 of treatment, the patient no longer required oxygen, and antifungal, antibacterial, and corticosteroid therapies were discontinued. On day 30 of ganciclovir treatment, CMV DNA became undetectable, and antiviral therapy was stopped.
Although the patient’s clinical condition had improved significantly, persistent bilateral pulmonary opacities on chest radiography prompted high-resolution computed tomography (HRCT), which revealed 24 mm lymphadenopathy in the left hilar region, nodular consolidation in the superior segment of the left lower lobe, and fibrotic changes in the right lower lobe (Figure 1). These findings raised suspicion of primary tuberculosis, and bronchoscopy was performed.
Acid-fast bacilli (AFB) staining and PCR for Mycobacterium tuberculosis from bronchoalveolar lavage (BAL) fluid were negative. No growth was observed in bacterial or tuberculosis cultures. Histopathological analysis showed predominantly necrotic cell blocks with no evidence of bacilli in viable cells, effectively ruling out tuberculosis.
On hospital day 54, the patient was discharged in stable condition with no further oxygen requirement, resolution of diarrhea, and regression of skin lesions, continuing ART and prophylactic antibiotics. At her 3-month follow-up, all symptoms had resolved, and she had gained weight. Her CD4+ T cell count had risen to 247 cells/mm³, HIV RNA was undetectable, and prophylactic antibiotics were discontinued (Table 1). At the patient’s request, ART was simplified to a single-tablet regimen consisting of tenofovir alafenamide fumarate, emtricitabine, and bictegravir. She remains clinically stable and continues regular outpatient follow-up.
Ethical ApprovalFormal ethics committee approval was not required in accordance with institutional and national guidelines.
CARE StatementThis case is reported in accordance with the CARE guidelines.
Discussion
Cytomegalovirus (CMV) is a common viral pathogen in the general population. In immunocompetent individuals, primary CMV infection is typically mild and self-limiting, occasionally presenting with a mononucleosis-like syndrome characterized by fever, fatigue, myalgia, and hepatosplenomegaly, after which the virus enters a latent phase. CMV can remain latent in endothelial cells, bone marrow stem cells, and peripheral blood monocytes.2 In cases of immunosuppression, the virus may reactivate and disseminate hematogenously to target organs.1,2 During the disseminated phase, CMV can be detected in a variety of tissues and cell types, indicating systemic spread. Reactivation is typically triggered by immunological dysregulation in the host.3
High-risk groups include individuals with HIV infection, active hematologic malignancies, recipients of hematopoietic stem cell or solid organ transplants, and patients receiving intensive immunosuppressive therapy due to autoimmune diseases.2 Consistent with the literature, our patient was newly diagnosed with HIV and exhibited profound immunosuppression, which likely predisposed her to CMV reactivation.
CMV and HIV may have a reciprocal relationship, whereby each promotes replication and disease progression of the other.1 Studies in populations with low CMV seroprevalence have shown that CMV coinfection may accelerate the progression from HIV to AIDS and negatively impact HIV-related outcomes, even in the absence of end-organ disease.1 Increasing CMV viremia levels are associated with increased HIV replication, hastening clinical progression and contributing to AIDS-related mortality.2 In our case, the coexistence of CMV-associated end-organ disease and HIV-related immunodeficiency is believed to have had a mutually exacerbating effect.
End-organ manifestations of CMV typically occur when the CD4+ T lymphocyte count falls below 50 cells/mm3.4 In patients with AIDS, CMV-related disease can involve colitis, esophagitis, hepatitis, cerebritis, and pneumonia, although the most frequently affected organ is the eye. Retinitis has been reported in approximately 80% of AIDS patients coinfected with CMV.1 Interestingly, no signs of retinitis were identified in our patient. Cutaneous manifestations are rare during disseminated CMV infection but may occur. These lesions often appear ulcerated with indistinct borders and tend to have a low bleeding tendency.3 The cutaneous lesions observed in our patient were consistent with these typical features.
CMV is considered an uncommon pulmonary opportunistic pathogen in HIV-positive individuals. However, in critically ill AIDS patients who do not respond to empiric treatment for other identified pulmonary infections, CMV pneumonia should be considered.2 Our patient presented with a severe pneumonia accompanied by hypoxemia and impaired pulmonary function.
CMV can be detected in various tissues of HIV-infected individuals.3 Confirmation of CMV infection can be achieved through culture, histopathological examination, and in situ hybridization.5 Light microscopy may reveal characteristic intranuclear inclusions; however, sampling limitations may reduce sensitivity.3 Since tissue sections may not always capture the inclusions, identification of enlarged cells alone may warrant further investigation.6 In our case, histopathological findings consistent with CMV were not detected in the skin biopsy samples, likely due to suboptimal tissue sectioning.
Detection of CMV DNA via polymerase chain reaction (PCR) or culture in respiratory samples is not sufficient for the diagnosis of CMV pneumonia. CMV can be identified in 20–50% of bronchoalveolar lavage (BAL) samples, but this often reflects subclinical infection or colonization. A definitive diagnosis requires cytological or histological evidence of CMV in lung tissue, which is reported in only 5–8% of HIV-positive patients undergoing bronchoscopy with biopsy.2 Due to the patient’s poor clinical status at admission, invasive sampling was not initially feasible. By the time bronchoscopy was performed, she had already been receiving antiviral therapy, likely diminishing the probability of detecting CMV-related pathology.
Before the advent of highly active antiretroviral therapy (HAART), CMV-related opportunistic infections were highly prevalent in AIDS patients, with disseminated CMV infection found in up to 90% of autopsy series.2 With HAART, the incidence of CMV disease has markedly decreased.1,2 The cornerstone of CMV management is immune reconstitution through ART, which suppresses CMV replication and reduces viral load. However, in cases with high CMV viremia and documented end-organ involvement, such as our patient, specific antiviral therapy (e.g., ganciclovir or valganciclovir) is warranted.2
The 2024 updated guideline by Gökengin et al. did not define an optimal duration for the treatment of disseminated CMV infection.7 In line with the current literature, antiviral therapy in our case was continued until full clinical, laboratory, and radiological recovery was achieved.
Limitations
The limitation of our case is that bronchoscopy and colonoscopy could not be performed due to the patient’s general condition, and a sample could not be obtained for pathological diagnosis.
Conclusion
In advanced HIV infection, clinicians must maintain a high index of suspicion for CMV in opportunistic infections with multisystem involvement, particularly when broad-spectrum antibiotics fail. Prompt diagnosis and initiation of appropriate antiviral therapy are essential to prevent disease progression and improve outcomes.
Declarations
Ethics Declarations
This case report was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Animal and Human Rights Statement
All procedures performed were in accordance with institutional and national ethical standards and the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and the accompanying radiological images.
Data Availability
All relevant data supporting the findings of this case are included within the article.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None.
Author Contributions (CRediT Taxonomy)
Conceptualization: R.B., P.B.K.
Investigation: R.B., İ.E., B.K., P.B.K.
Data curation: R.B., İ.E.
Resources: R.B., P.B.K.
Writing – original draft: R.B.
Writing – review & editing: R.B., İ.E., B.K., P.B.K.
Supervision: P.B.K.
Scientific Responsibility Statement
The authors declare full responsibility for the scientific content and integrity of this manuscrip
Abbreviations
AIDS: Acquired Immunodeficiency Syndrome
AFB: Acid-Fast Bacilli
ART: Antiretroviral Therapy
BAL: Bronchoalveolar Lavage
CMV: Cytomegalovirus
DNA: Deoxyribonucleic Acid
HAART: Highly Active Antiretroviral Therapy
HIV: Human Immunodeficiency Virus
HRCT: High-Resolution Computed Tomography
IgG: Immunoglobulin G
IgM: Immunoglobulin M
MRI: Magnetic Resonance Imaging
PCR: Polymerase Chain Reaction
PPD: Purified Protein Derivative (Tuberculin Skin Test)
RNA: Ribonucleic Acid
SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2
References
-
Jabs DA. Cytomegalovirus retinitis and the acquired immunodeficiency syndrome—bench to bedside: LXVII Edward Jackson Memorial Lecture. Am J Ophthalmol. 2011;151(2):198-216.e1. doi:10.1016/j.ajo.2010.10.018
-
Poh KC, Zheng S. A rare case of CMV pneumonia in HIV infection. Respir Med Case Rep. 2019;28:100945. doi:10.1016/j.rmcr.2019.100945
-
Langford A, Kunze R, Timm H, Ruf B, Reichart P. Cytomegalovirus-associated oral ulcerations in HIV-infected patients. J Oral Pathol Med. 1990;19(2):71-76. doi:10.1111/j.1600-0714.1990.tb00799.x
-
Bronke C, Palmer NM, Jansen CA, et al. Dynamics of cytomegalovirus (CMV)-specific T cells in HIV-1–infected individuals progressing to AIDS with CMV end-organ disease. J Infect Dis. 2005;191(6):873-880. doi:10.1086/427828
-
Brady MT, Reiner CB, Singley C, Roberts WH 3rd, Sneddon JM. Unexpected death in an infant with AIDS: disseminated cytomegalovirus infection with pancarditis. Pediatr Pathol. 1988;8(2):205-214. doi:10.3109/15513818809022298
-
Licci S. An HIV-positive man with cough, fever, and progressive dyspnea. Disseminated cytomegalovirus (CMV) infection. Clin Infect Dis. 2008;47(9):1231-1232. doi:10.1086/592297
-
Gökengin D, Korten V, Kurtaran B, Tabak F, Ünal S. HIV/AIDS Tanı, İzlem ve Tedavi El Kitabı. 3rd ed. Istanbul: Nobel Medical Bookstores; 2024:126-130.
Figures

Figure 1. Chest X-ray and high-resolution tomography images of the patient
Tables
Table 1. Laboratory parameters at admission and after treatment
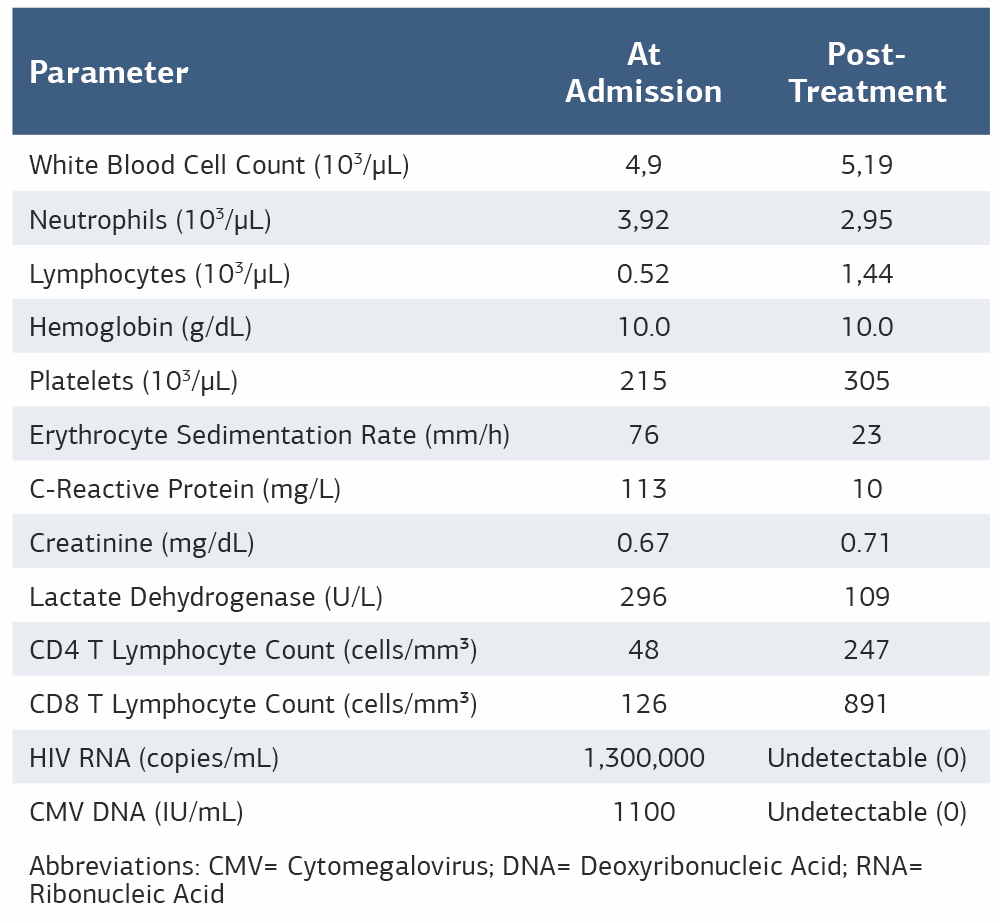
Abbreviations: CMV= Cytomegalovirus; DNA= Deoxyribonucleic Acid; RNA= Ribonucleic Acid
Additional Information
Publisher’s Note
Bayrakol MP remains neutral with regard to jurisdictional and institutional claims.
Conference Presentation
This study was presented as an e-poster at the 13th EKMUD Congress, Antalya, Türkiye, 2025
Rights and Permissions

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License (CC BY-NC 4.0). To view a copy of the license, visit https://creativecommons.org/licenses/by-nc/4.0/
About This Article
How to Cite This Article
Rukiyye Bulut, İbrahim Erayman, Bahar Kandemir, Pınar Belviranlı Keskin.Disseminated cytomegalovirus infection in a newly diagnosed HIV-positive patient: A Case Report. Ann Clin Anal Med 2026;17(3):273-276
- Received:
- October 14, 2025
- Accepted:
- December 15, 2025
- Published Online:
- January 8, 2026
- Printed:
- March 1, 2026